Today I am showing a recent case seen by my good friend Dr. Josep Mata. Radiographs belong to a 48-year-old man with haemoptysis and history of previous TB. Have a look at the images below, leave your thoughts and diagnosis in the comments section, and come back on Friday for the answer.
1. Infected bulla
2. Reactivation TB
3. Carcinoma in previous cavity
4. None of the above
Findings: PA radiograph in June 2013 shows a cavity in the RUL (A, arrow), with moderate peripheral pleural thickening (A, red arrow). One and a half years later, the wall of the cavity is thicker (B, arrow) and there is increased thickening of the pleura as well (B, red arrow).
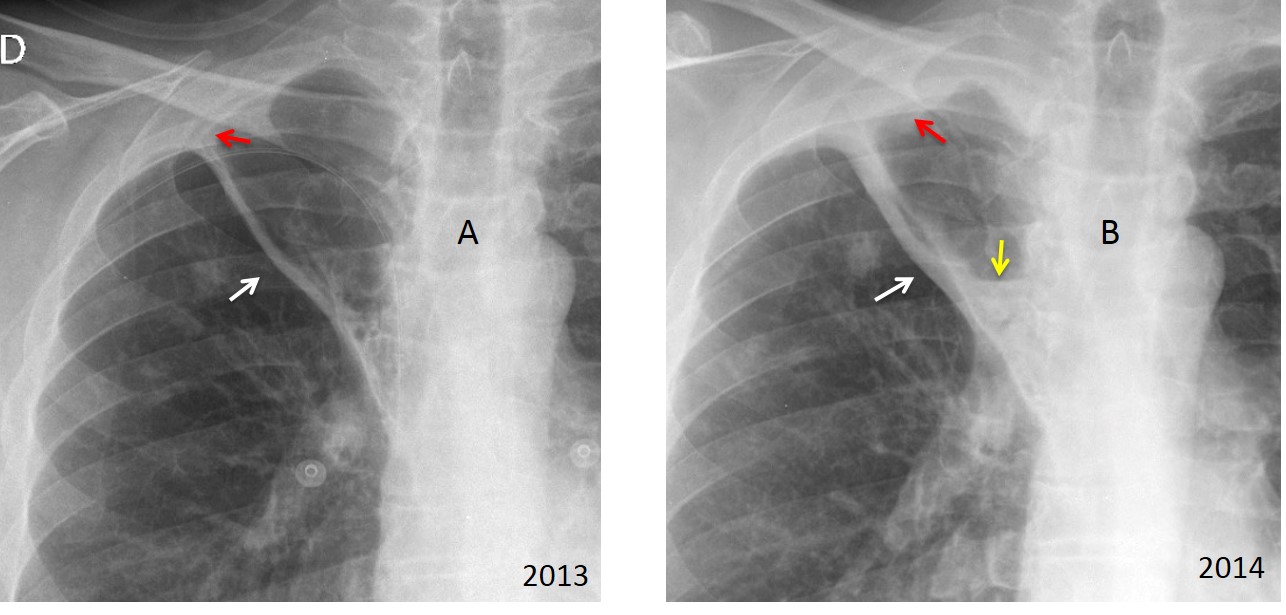
There is a small air-fluid level (B, yellow arrow). This progression is suspicious of aspergillus colonising a pre-existing cavity. CT demonstrates spongiform tissue of fungal strands inside the cavity (C-F, arrows).
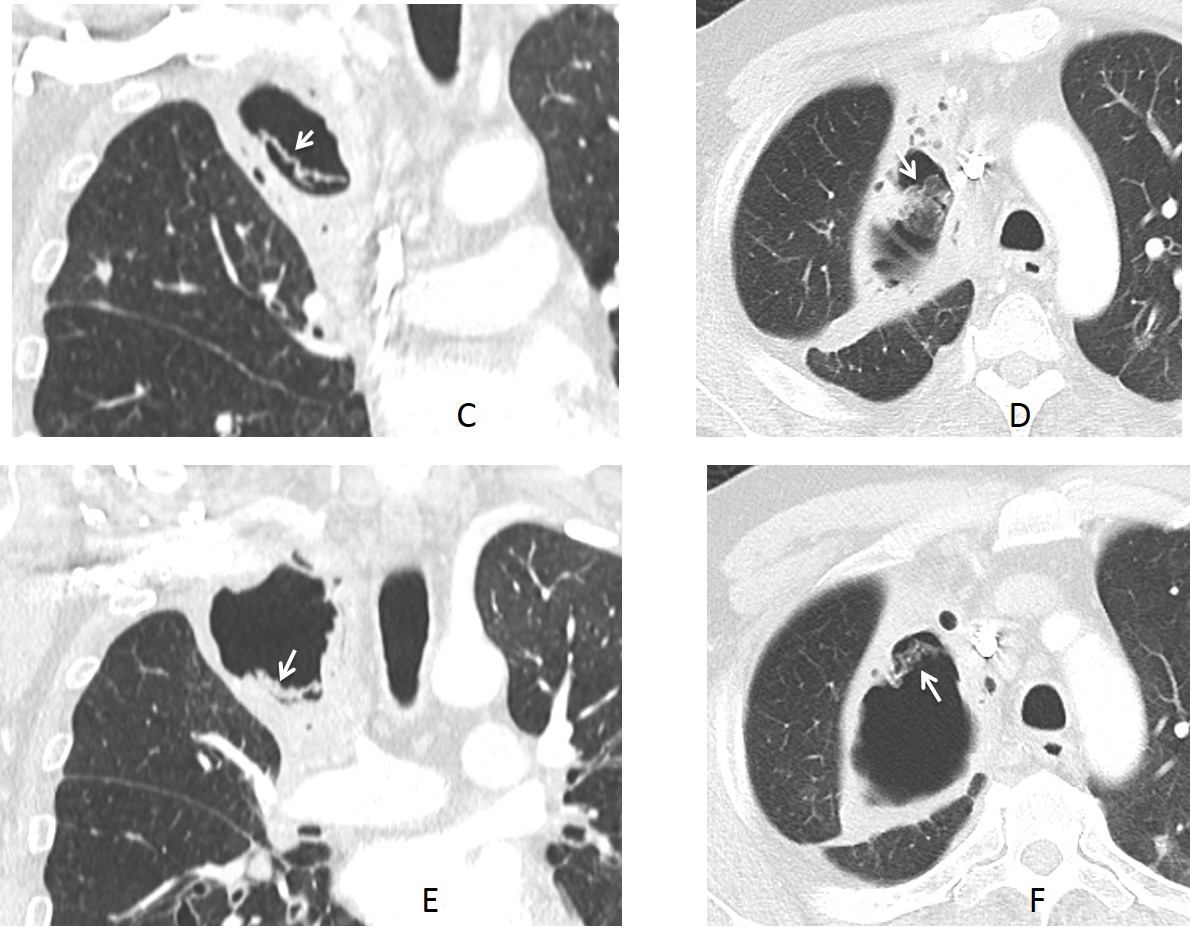
Final diagnosis: Mycetoma
Congratulations to Nicky, who was the first to suggest mycetoma.
Teaching point: remember that progressive pleural thickening in the periphery of a pre-existing cavity is an early indicator for mycetoma.



Crucial qustions: Is the pateint febrile? Does he have night sweats? Did he loose any weight?
Answers: no, no, a little.
Reactivación de TB.
Infected bulla
It is infected with newly depicted fluid level
Infected bulla
Dilated azygos vein, enlarged central pulmonary arteries, the right upper costal and mediastinal pleural thickening. Pulmonary hypertension and fibrosing mediastinitis?
non of above
None of the above. Fungal ball in cavity
Lobula v. azygos with apical carcinoma (Pancoast?)
Apical carcinoma of lobe of v. azygos
I think is not cancer why?
– The pulmonary nodes on both lungs is stable in a long time (without chemiotherapy).
– no other change on both images except thickening on the right apical cup.
– no rib involvement.
– the thickening is growth in azygos lobe und in oblique fissure too.
I think is pleural fat in chronic tb
There is also an air-fluid level, not visible in 2013.
sorry no azygos lobe. is a catheter on june film
Given onlt chest x-ray I cant exlude anything.
I’m waiting for CT.
This is the easy way out. The plain fim findings give you grounds for especulation. Of course, you need CT to confirm your suspicions.
None of the above
There is pleural thickening in the right apical area and that happened in a year and a half more or less. There is also thickening of an oblicque line probably an azygous lobe fissure.
Before this I would think about
1.- Pancoast tumour
2.- Occult aspergilloma where you only see the pleural reaction
Between both I would choose tho second one regarding no pain and no significant weight loss is reported. Haemoptysis is a complication of aspergilloma and history of TB is also suggesting.
Nice to see Dr Mata in white coat.
There is an air-crescent sign and its suggestive of aspergylloma in chronic cavity TB.
Reactivation T.B
It can be infected bulla
There is an azygos lobe with cisuritis an and an air-fluid level, so it seems inflammatory or infectious proccess. I choose option 1, infected bulla.
In view of h/o Koch’s it can be thick walled cavity with fluid level limited by the azygous fissure due to reactivation TB
…radiogramma 2013: esiti di scissurite lobo accessorio v.azygos e presenza di immagine bollosa in apice( pareti sottili della bolla)….radiogramma 2014….iperplasia delle ombre ilari di natura adenopatica….ispessimento pleura corticale e versamento interscissurale del lobo v.azygos….presenza di piccolo livello idroaereo nella bolla, senza che di riesca a vedere(all’Rx) eventuali masse da “ospiti” indesiderati…..ipotesi diagnostica….Ripresa di attività TBC….Saluti da Bari alla eccellente coppia !
infected bulla
2014 Upper lobe volume loss with dislocation and thickening of minor fissure (and obstruction of the upper lobe bronchus/ subatelectasis ).
In 2013, there seems to be a port A Cath ( cancer treatment ?) . Lung cancer ?