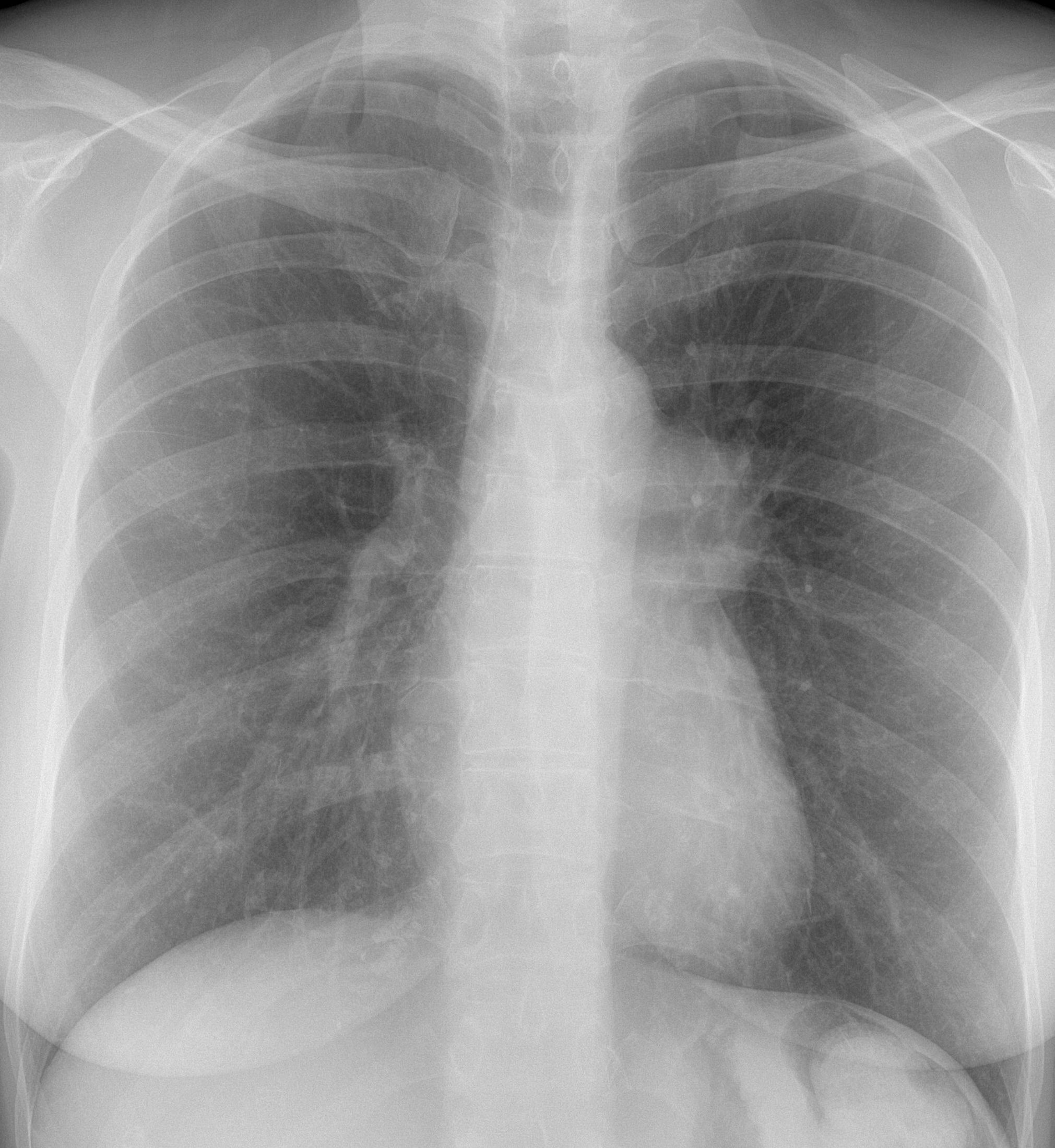
Since you will be tired after the ECR Congress, I am showing an easy case. These images were taken during a routine check-up of a healthy 55-year-old woman. What do you think?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Findings: the PA chest radiograph shows an enlarged right hilum (A, arrow). Axial unenhanced CT confirms the hilar mass (B, arrow) with a central calcification. Enhanced coronal CT shows marked contrast enhancement of the mass (C, arrow).
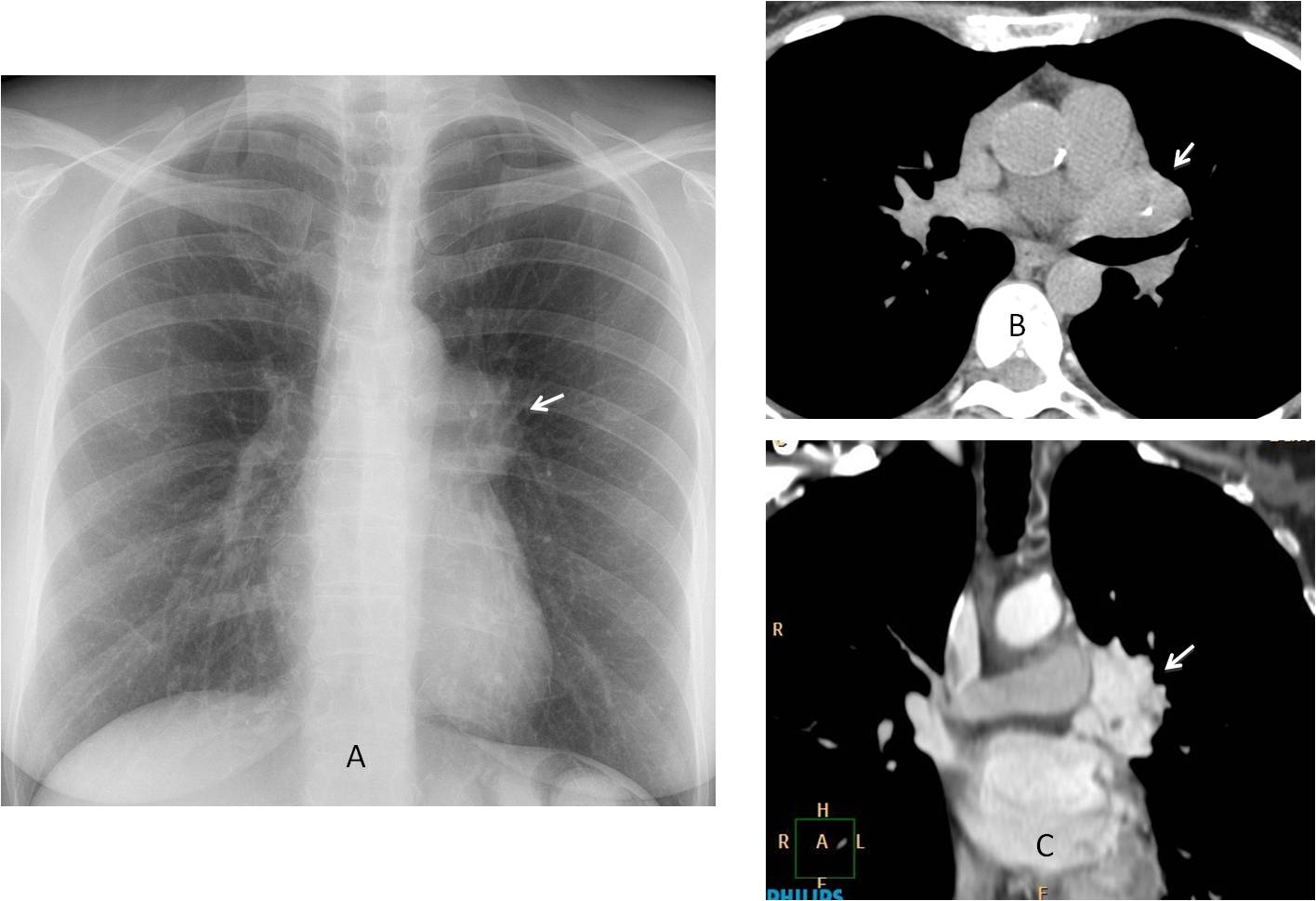
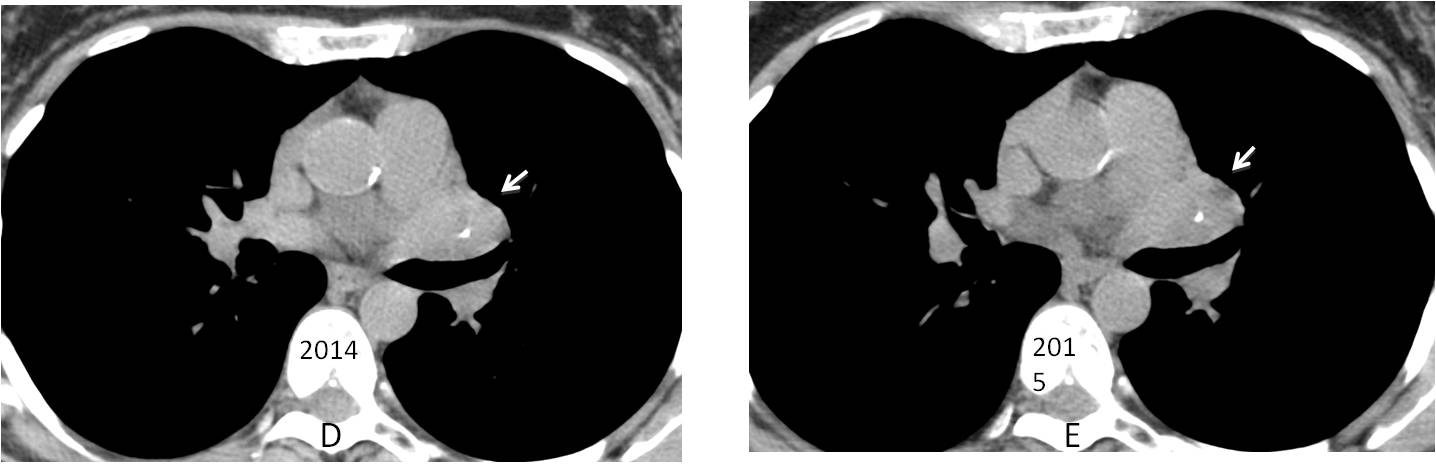
This case has an interesting history. The patient had a routine check-up in 2014 with an unenhanced CT (D) diagnosed as normal. Repeated CT in 2015 (E) was reported as unchanged. Fortunately, a chest radiograph was taken at that time and the hilar abnormality was discovered. It prompted an enhanced CT, which clearly showed the markedly enhancing hilar mass.
The main differential diagnosis of markedly enhancing masses in the chest is limited: Castleman’s disease, carcinoid, glomus tumour and thyroid. Because the location of the mass, I made the diagnosis of Castleman’s.
The patient was operated on and a benign carcinoid was found.
Final diagnosis: central carcinoid tumour of the lung.
Congratulations to all of you who participated and offered a correct differential diagnosis: tr, MK, 19Medicus83 and ren.
Teaching point: this case emphasises one basic principle: “always think of a rare manifestation of a common disease than a common manifestation of a rare disease”. I chose to ignore it and made the wrong diagnosis.




Hi,
I can see prominence of the left hilum on the cxr.
on the CT scan, the lesion location and enhancement suggest pulmonary vein varix.
Good morning,
The aorta-pulmonary window is busied. In the coronal CT there is a communication between the vascular left hilar lesion and the left atrium, so it is a pulmonar vein increased in size.
Perhaps an anomalous unilateral single pulmonary vein?
Unilateral single pulmonary vein has a different appearance.
Carcinoid tumor with the feeding artery visible in the coronal view at the left paratracheal margin?
Calcification and avid enhancing are good qualities for them
Hi,
interestingly, there is a small calcification within the lesion on the axial section, and two small filling defects on the coronal section which leads me to incline toward solid lesions, the lesion is enhancing homogeneously and avidly, and I think with only two sections provided, one can think of: castleman disease, enhancing middle mediastinal masses like neurogenic tumors, connective tissue tumors (leimyoma…).
Your discussion is correct. Any other alternatives?
Hi,
Tha calcification might be simply a calcified lymph node.
A phlebolith in a vascular malformation can be considered, although uncommon, because of the tortuous vessel at the left side of the trachea which might be a feeding artery or a draining vein.
Thanks
Pulmonary artery aneurysm
In the pa chest x ray an obvious rounded lesion adjacent to the aorto-pulmonary window with sharp contour is visible.
Reformated coronal CECT shows an enhancing lesion with fat plane separating it from the pulmonary trunk, while a small calcification in axial NECT is seen.
Being an bright enhancing lesion with small calcification in the middle mediastinum I don`t think of an vascular origin. I would also favor Castleman disease, DD: thymoma.
Your discussion is correct, although I would not include thymona in the DD (middle mediastinum y too much enhancement). Can you think of other alternatives?
Hm, like already mentioned a partly calcified lymph node? Although systemic disorders like silicosis or sarcoidosis seem quite unlikely to me (no lung changes, normal right hilum).
Another idea would be a teratoma (partly calcified, partly fat containing, not infiltrating) keeping in mind that anterior mediastinum is the usual location.
i think there is a lesion in the aorto-pulmonary window
Reformated coronal CECT shows an avidly enhancing lesion ,with a small calcification in axial NECT is seen.
Being an bright enhancing lesion with small calcification in the middle mediastinum. vascular origin like hemangioma .castlemans ,lymphnodal mets from a hypervascular tumor, ectopic carcinoid would be my differentials
….grande Prof……grande Barca… !!!!!
I am average compared to Barça!