Dear Friends,
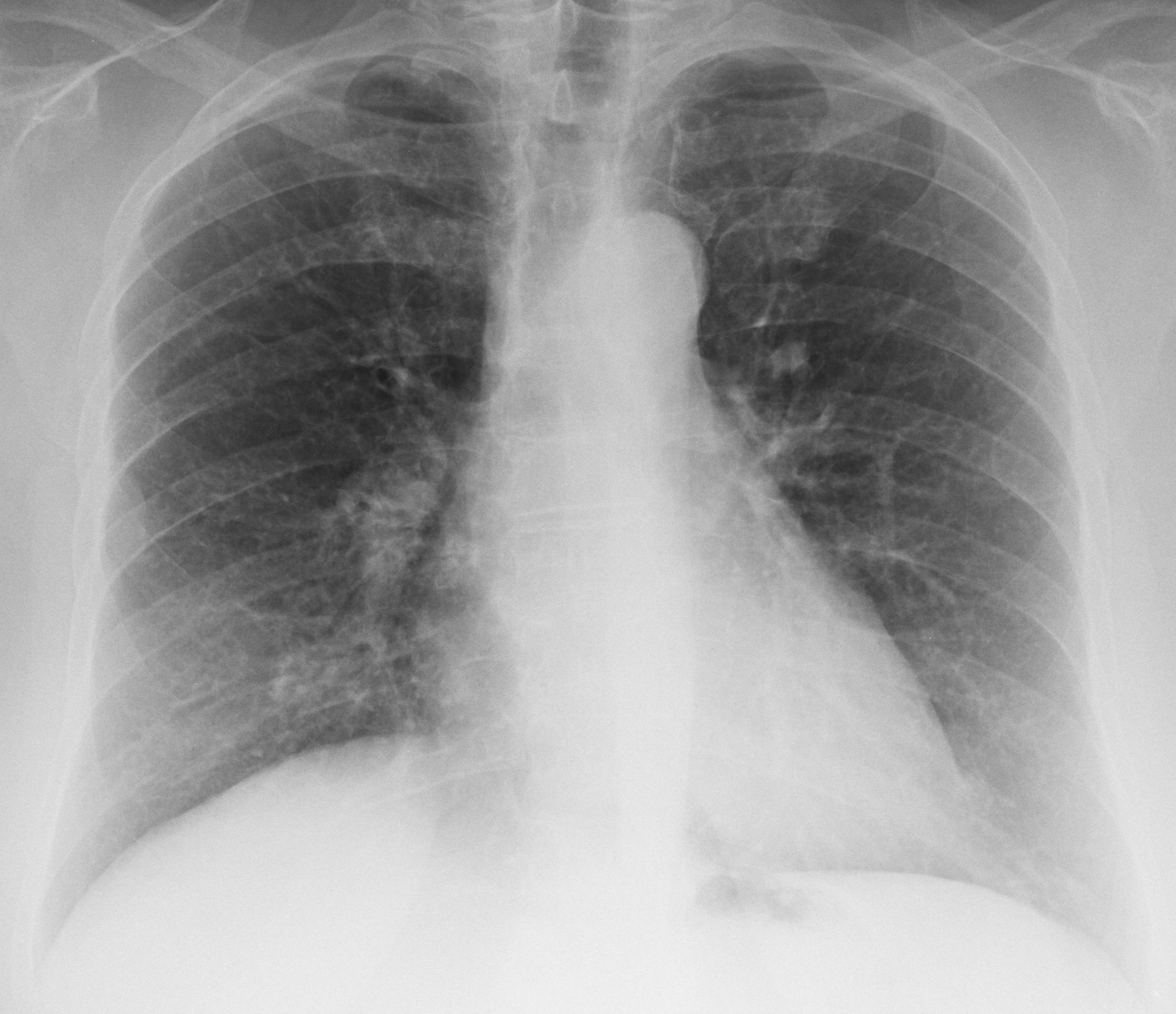
Today’s images are a routine annual control of a 55-year-old woman operated on for carcinoma of the breast five years ago. What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Click here for the answer
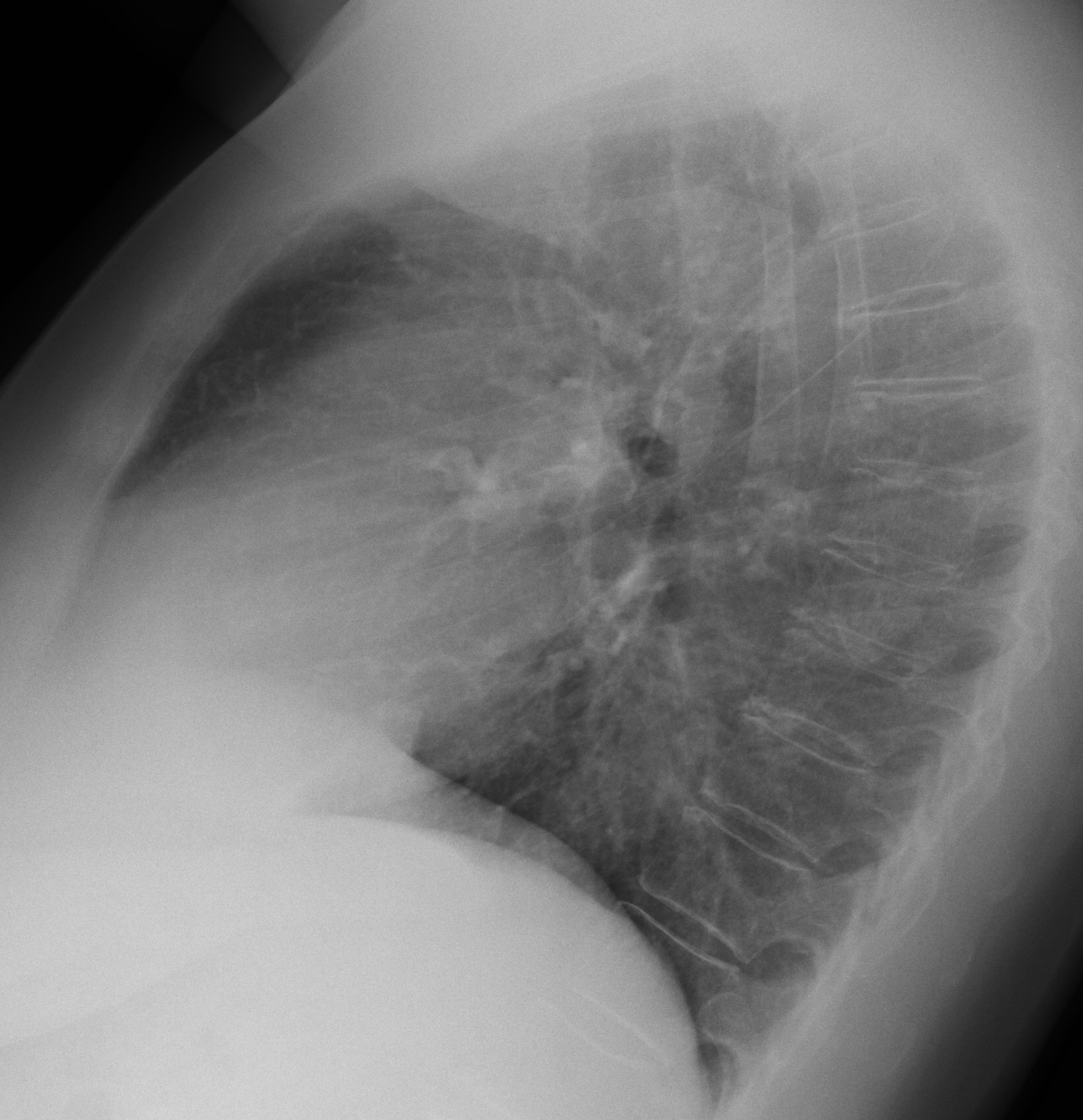
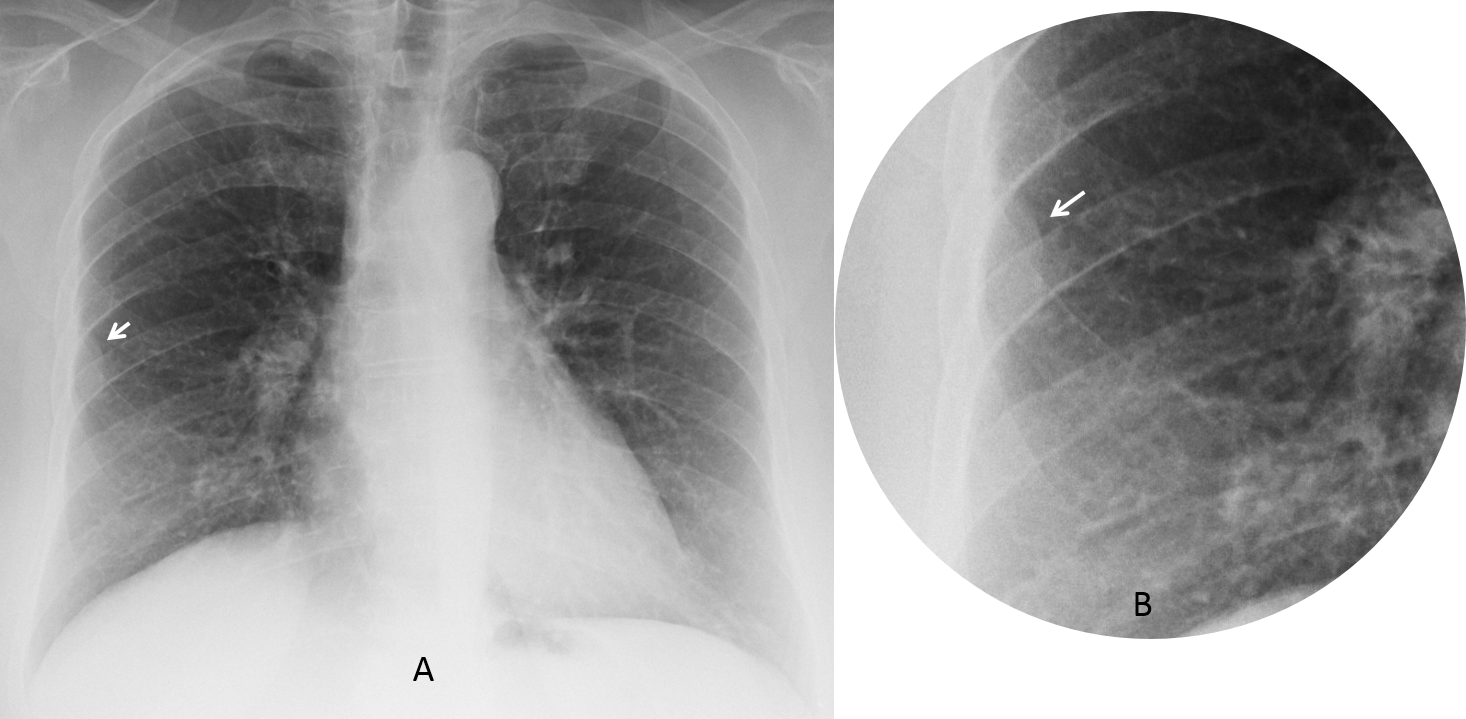
Findings: an extrapulmonary lesion is visible in the lateral aspect of the right hemithorax in the PA radiograph (A-B, arrows). The lateral view is unremarkable. The lesion was not present in images taken one year earlier. Although it has been mentioned by one of you, I do not see any rib fractures. When I saw the images, my first impression was a metastatic pleural implant.
Unenhanced CT two weeks later shows healing fractures of the 5th and 6th ribs (C-E, arrows). The lesion has disappeared.
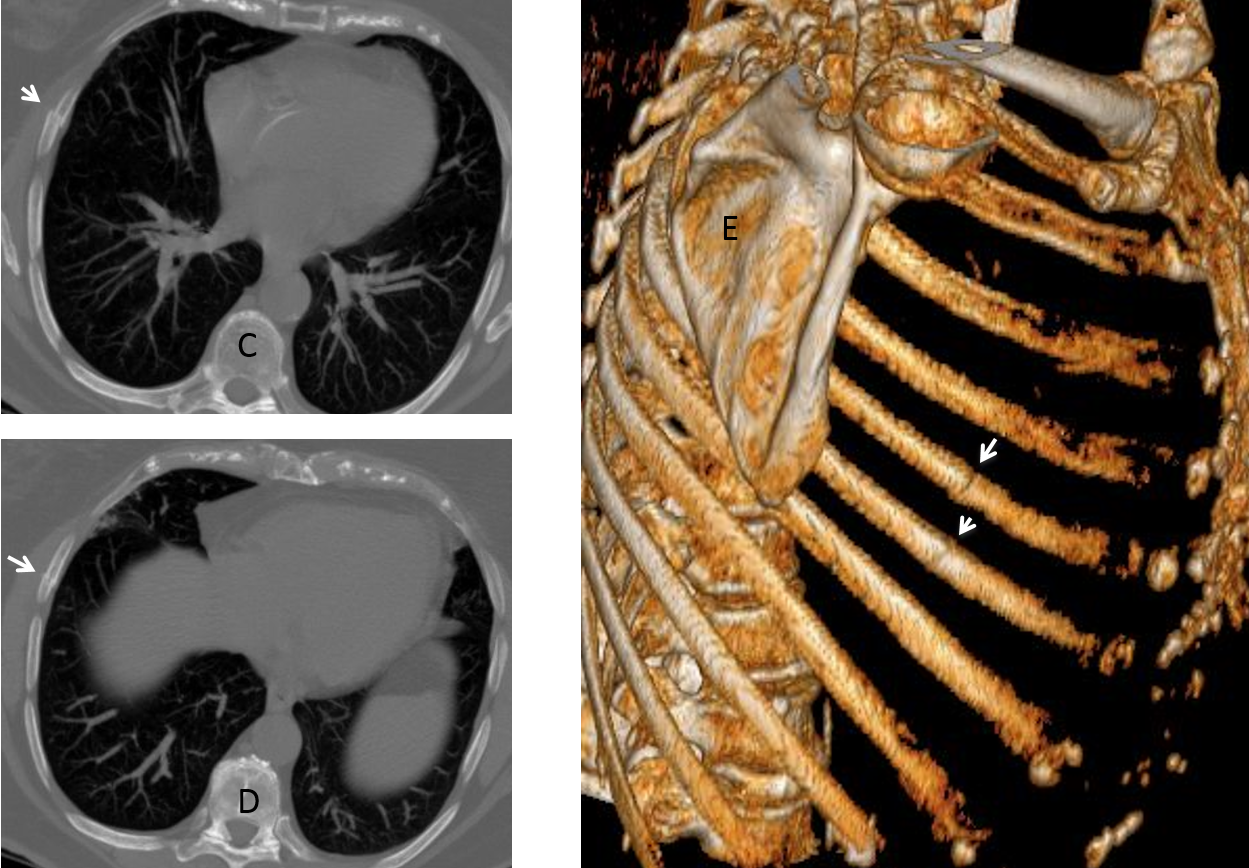
Final diagnosis: unsuspected rib fractures with extrapleural haematoma.
Congratulations to Maria P. who was the first to mention the right diagnosis.
Teaching point: I will repeat my advice of a recent similar case (Caceres’ corner161), which I promptly forgot and made an ass of myself! Rib fractures are common and should always be considered even if the findings are not clear.


Let’s have a try…
I think there is an extrapleural lesion adyacent to the 5th right costal arch (axillary part), and a costal fracture associated.
Metastasic disease should be ruled out if there isn’t traumatic context.
Good moornig!!!
There is an extrapleural lesion between the 5 and 6 costal arch. Which side was the surgery? My first option is metastasic disease, but I would like to compare with previous x-rays.
The retrocardiac space is increased in density (it seems to be the descending aorta)
Subtle reticular pattern in pulmonary parenchyma?
Previous chest radiograph taken one year earlier was normal
If the previous x-ray was normal and no history of trauma, I have to think on mtx disease.
That’s correct. And we both made the same mistake!
Greetings,
– Removed left breast.
– Small isodense lesion with incomplete round sclerotic margin over the pedicles of the lowest dorsal vertebra.
– Elevation of the anterior aspect of the right hemidiaphragm (normal lobulation, loculated subpulmonic effusion,..).
– otherwise unremarkable chest radiograph.
Impression:
– Focal lesion with non-aggressive features over the pedicles of the lowest dorsal vertebra; seen on the lateral view.
– Elevation of the anterior aspect of the right hemidiaphragm (normal lobulation, pleural/diaphragmatic or sub-diaphragmatic lesions..).
extrapleural lesion
RETICULARE PATERN (LYMPHANGITIS CARCINOMATOSIS?
there is obvious decrease in volume of the right lung – the elevation of right hemidiaphragm and obscured cardio-diaphragmal angle
but there are no corresponding triangular opacity on lateral view (if suggesting RML atelectasis/hypoventilation or displacement of any fissures – if it is about RLL atelectasis/hypoventilation)
so this volume loss could be the result of fibrous changes after oncological treatment – after chemotherapy and|or radiotherapy (anamnesis morbi needed)
on the level of II intercostal space near the upper part of the left hilum there is oval-shape opacity hight intensive which is hard to distinguish on lateral view (in anterior segment left lung closely to hilum?) – suggesting lymphatic nodule ? mts nodule ?
conclusion: fibrotic changes of the basal parts of the right lung due to chemo- and/or radiotherapy; nodular opacity of the left upper lobe; previous chest radiographs are needed to compare – if there where no changes on previous examination, the patient should undergo CT with contrast enhancement
Greetings,
I would like to add something; that is the PA view is mildly underpenetrated which limits the evaluation, and exaggerate the bronchovascular markings.
Possible small opacity over the cardiac apex margin that I cannot see in the lateral view, which raise the suspicion of pulmonary metastases.
thanks
What do you think of the extrapulmonary lesion in the right hemithorax?
Greetings,
Well, I have to admit that I did not catch it until I checked the image on a different device.
There is a faint pleural based density in the right chest, but I do not see destruction of the adjacent ribs or pleural effusion, which makes the metastatic disease very unlikely, I think it should be some kind of benign pleural lesion (lipoma, fibrous tumor, leiomyoma..), but on the other hand, I am not sure if these can develop over a one year period, since that the previous cxr was normal.
I see a reticular pattern in both lungs.
Chest wall lesion located between the 4th and 5th anterior ribs on right (pregnancy sign)
Increased thickness of right paratracheal stripe?
Without CT my best guess would be lymphangitic cacinomatosis.
Right paratracheal line is widened.
I believe the paratracheal line is of normal width. The shadow of the SVC simulates a widened line
Hello,
As we have a patient with breast cancer in her history we have to look for metastasis.
The main targets for metastasis in case of breast cancer are the bones and lung.
I think the lungs are clear.
Suspicious bony regions are:
Right 5th rib lateral part with a cortical step sign (previous pathological fracture?) surrounded by well circumscribed object (callus?).
On the lower region of the lateral image the back part of the lowest vertebra (Th.XI.?) there is a well-defined region with sclerotic edge (metastasis?).
My conclusion is multiple bone metastases.
….sulla parete laterale dx tra la 6 e la 7 costa, tenue opacità rotondeggiante, a limiti netti e sede extrapolmonare, come da espanso benigno( lipoma)….da Bari, con stima….
…od ematoma osseo.
Due to an informatic glitch, answer will be posted next Monday. Correct answer is: extrapleural hematoma secondary to rib fracture. CT showed dissapearance of the hematoma and two broken ribs.
Sorry about the delay 😉