Today I am showing a case seen one month ago. Radiographs belong to a 64-year-old man with intermittent fever for the previous two weeks. What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
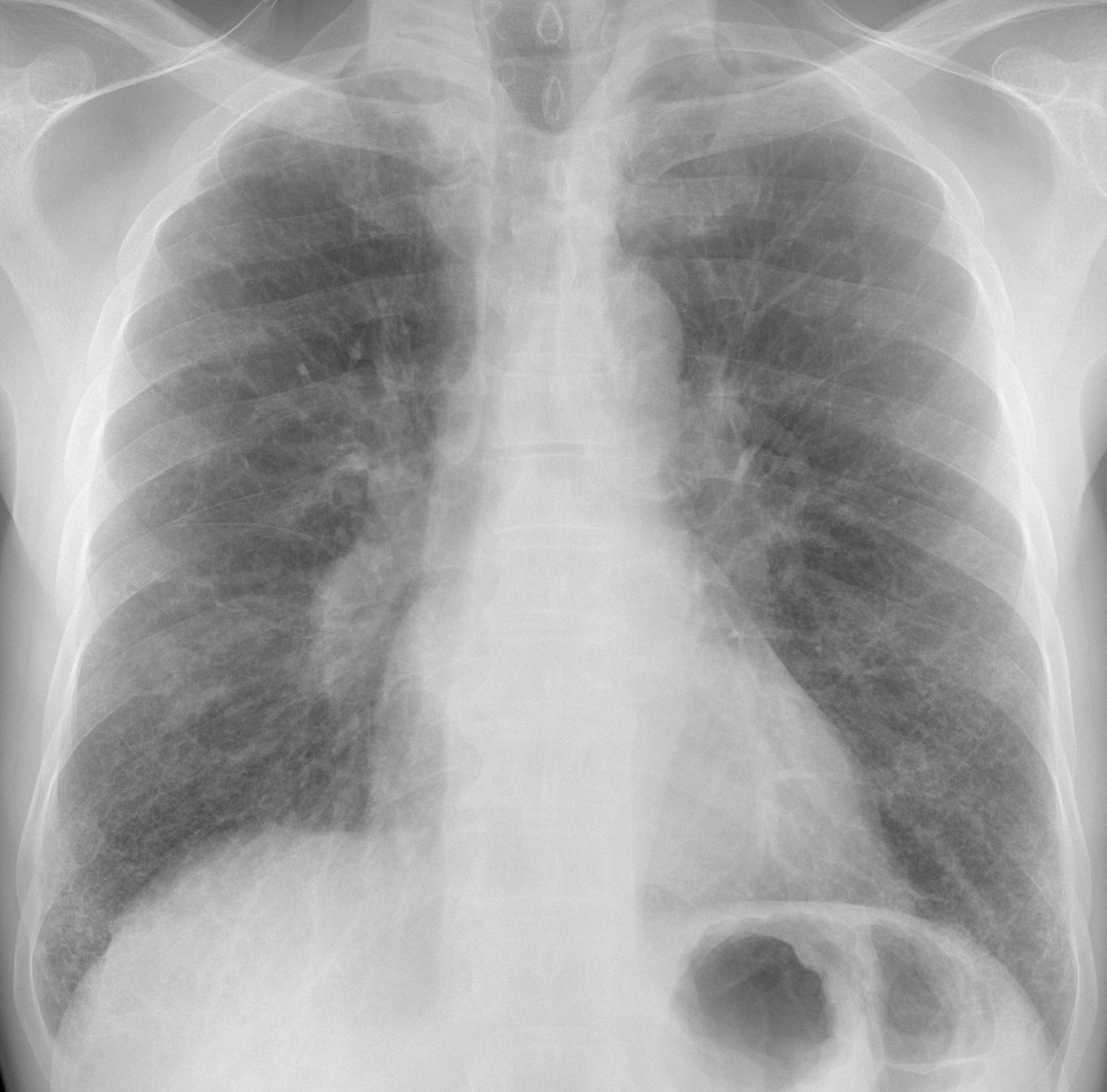
Findings: in the PA view there is a fine interstitial pattern in both lung bases. I believe that the rest of the lung is normal. What caught our attention was the increased opacity of the lower right hilum, visible in the PA and lateral projections (A-B, arrows).
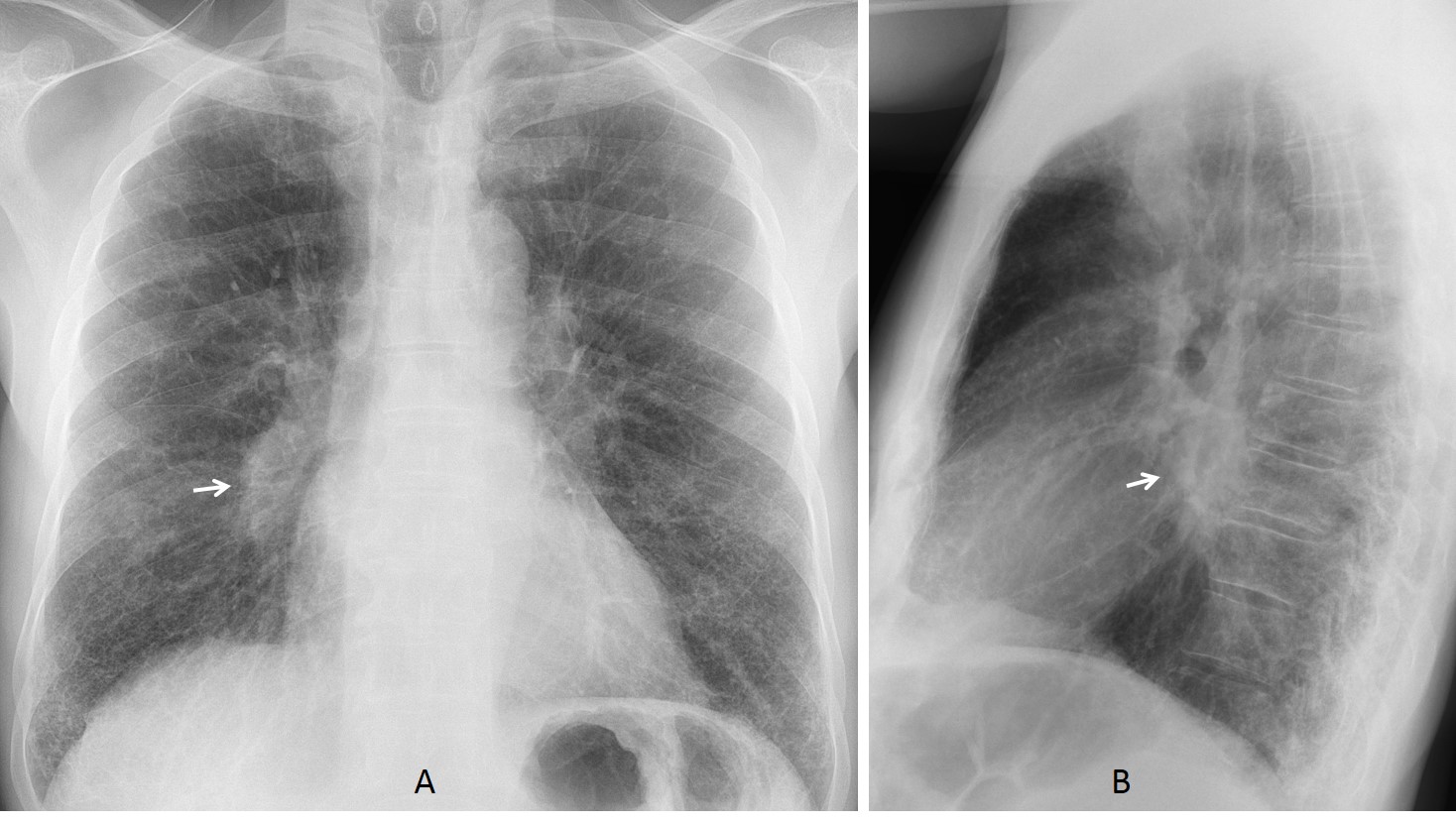
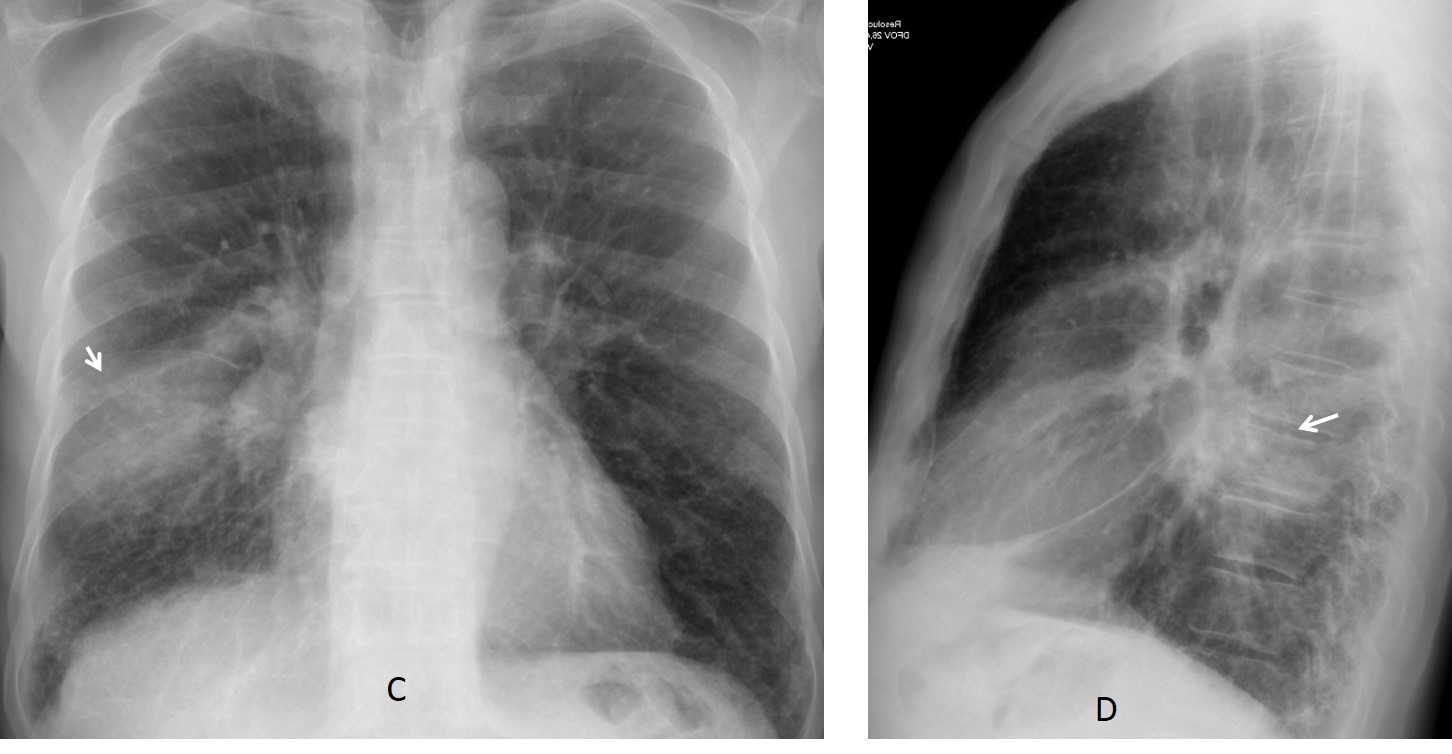
We suspected unilateral enlarged lymph nodes and recommended CT. The attending physician did not follow the recommendation until the patient returned three weeks later with high fever and an infiltrate in the right lung (C-D, arrows).
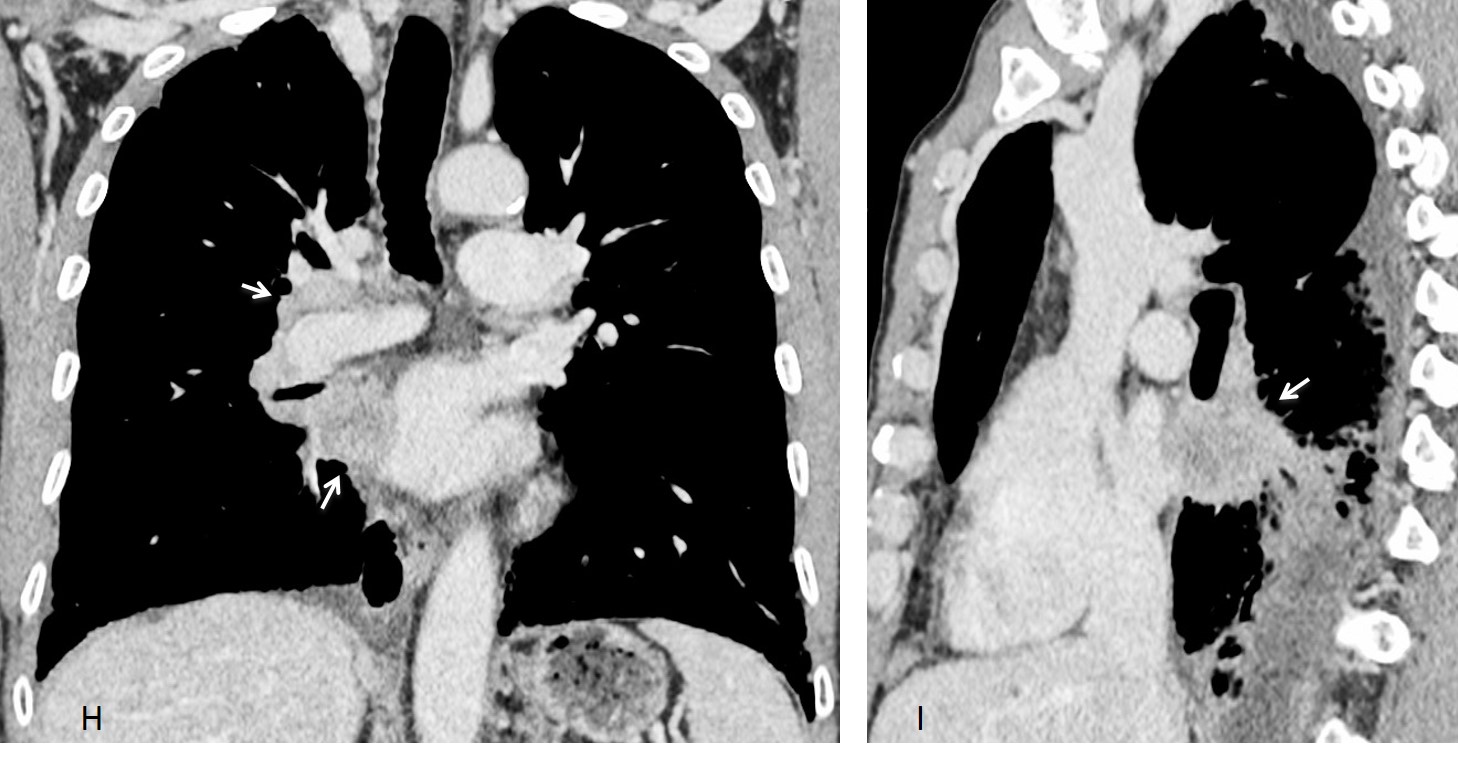
Enhanced CT confirms the basal fibrosis (E) as well as a large PET positive mass in mediastinum and right hilum (F-G, arrows), better seen in the coronal and sagittal reconstructions (H-I, arrows). Biopsy confirmed a squamous-cell carcinoma.
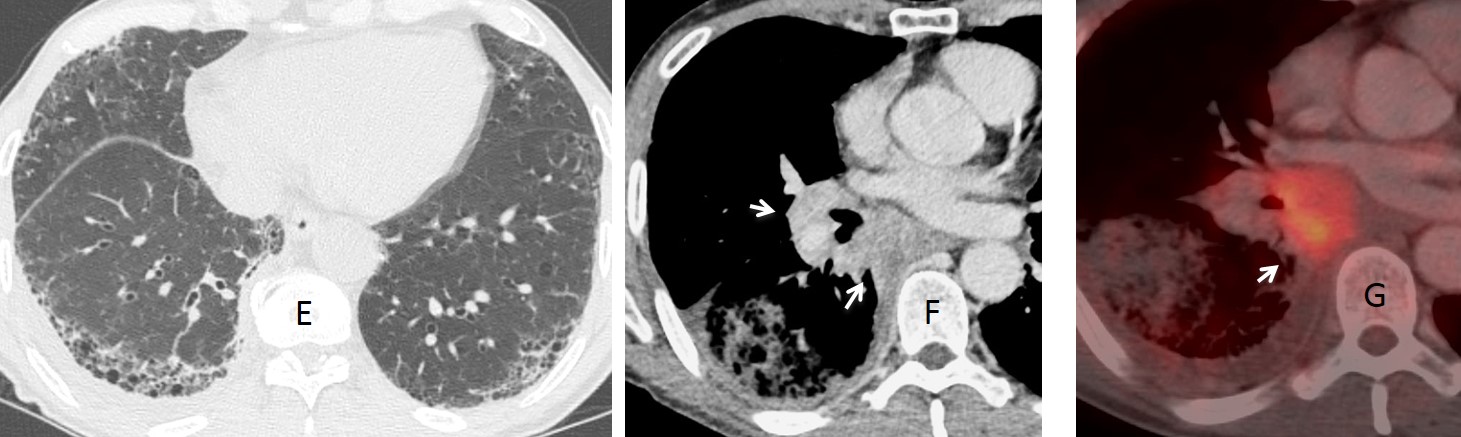
Final diagnosis: Squamous-cell carcinoma of right hilum and mediastinum, barely visible in the chest radiograph. Basal pulmonary fibrosis.
This was a difficult case and I believe most of you gave your best. I must single out Olena, because she described the alterations in the right hilum and was very perseverant.
Teaching point: avoid satisfaction of search and remember to look at the lateral view.



On the level of trachea lumen (trachea is normal) there is hyperlucency which I can not see on the lateral view.
There are interstitial changes in both lungs with small multiple barely noticeable nodules mostly in lower parts of both lungs – reticulonodular pattern.
On lateral view there is an ill-defined opacity on the level of left lower bronchus and LLL hypoventilation suggested (the major fissure on the left is shifted down).
Both hila are enlarged – suggesting bronchopulmonary lymphadenopathy
1/ lymphangitis carcinomatosis
2/ occupational disease (silicosis)
3/ sarcoidosis
Are there previous X-ray?
There are no previous radiographs
Are there any information about connective tissue disease – rheumatoid arthritis?
I suppose some variant of the interstitial pneumoniae should be added for differential diagnosis
I wrote that both hila are enlarged.
Is there an oval mass which is projected on interlobal artery on the right?
Yes
Are there two nodular opacities on the right on the level of the first rib in subpleural region?
Is this patient HIV positive?
I suppose tuberculosis also should be added – it could be tuberculoma on the hila level and miliary dissemination, but distribution is not typical
The question also is there on lateral view opacity in front of trachea (lymphadenopathy? Mass?)
What are the clinical data except fever? Sputum analysis? Bronchoscopy?
There is also slightly obsuring lung space on the right on the apex and near mediastinum – visceral pleura thickening, or I “see” too much?
Greetings,
– bilateral symmetrical fine reticulonodular interstitial pattern in the lung bases without remarkable volume change.
prominence of the right descending pulmonary artery.
– unusually prominent shadow of the steroncleidomastoid muscles giving the V-shaped lucency over the trachea.
Impression:
the findings indicate interstitial lung disease with predilection to the lower zones with no significant volume change, the differential diagnosis is wide, and the presentation suggests acute/subacute disease: acute interstitial pneumonia (viral, mycoplasma..), LIP, inhalation disease, drug reaction, connective tissue disease, and idiopathic disease.
Thanks
How do you value the prominence of the right pulmonary artery?
Greetings,
I think it is fair to say that there is bilateral hilar prominence, and possibly a pretracheal density, with the interstitial disease I think it is reasonable to consider stage II pulmonary sarcoidosis (a great mimicker), although the interstital pattern is not in favour of it.
Thanks
Hello!
Prominent hilios and reticular bilateral pattern. Right paratracheal line is thickened. In the lateral view there is an increased density anterior to the trachea.
Sarcoidosis or TBC
Associated tracheal diverticulum?
Sorry, yugular notch (like in the film “El paciente inglés”)
You did your research. Good. It is a normal finding.
Hyperlucent lesion in tracheal level. Zenker diverticulum? We can think in chronic aspiration with an intersticial pattern in lower lobes. There is also hilar prominence bilaterally.
Greetings
Lucretius – Brazil
Glad to have a Brazilian on board! The hyperlucent lesion is a suprasternal notch, which is a normal finding.
Keep looking 😉
Maybe shooting for the stars, but I would build a differential diagnosis over pulmonary cavities + micronodules… in this case TB would be quite all right except for the distribuition. Poliangiitis with granulomatosis (Wegener) would be a good fit, but quite uncommon. Squamous carcinoma metastases and septic emboli would also be in the possibilities.
If, however, my “quijotean” eyes made the cavities… I’d stick with the previous opinions and go for sarcoidosis.
Final bet still Wegener.
Your eyes deceived you 😉
Windmills not giants… So I guess our colleagues have already said it…
Don Quixote never gave up. Why should you? I still don’t have a clear winner.
You are right, professor… the dice rolls still. Maybe I am still hitting on the windmills, but with the cavities out of the way, I would go for hypersensitivity pneumonitis. The enlarged lymph nodes are not that commonly associated, but they can be, so that is my new bet.
interstetial lung disease ,rt lowe r lung opacity
I’m Brazilian and I’m doing a radiology course and I always look for extra knowledge on the internet. I just found out your blog and I’ve already put it in the favorites.
I do not speak English so I have to use Google Translate.
Welcome! You can write your answer in Brazilian if you feel more confortable. I believe I can understand it.