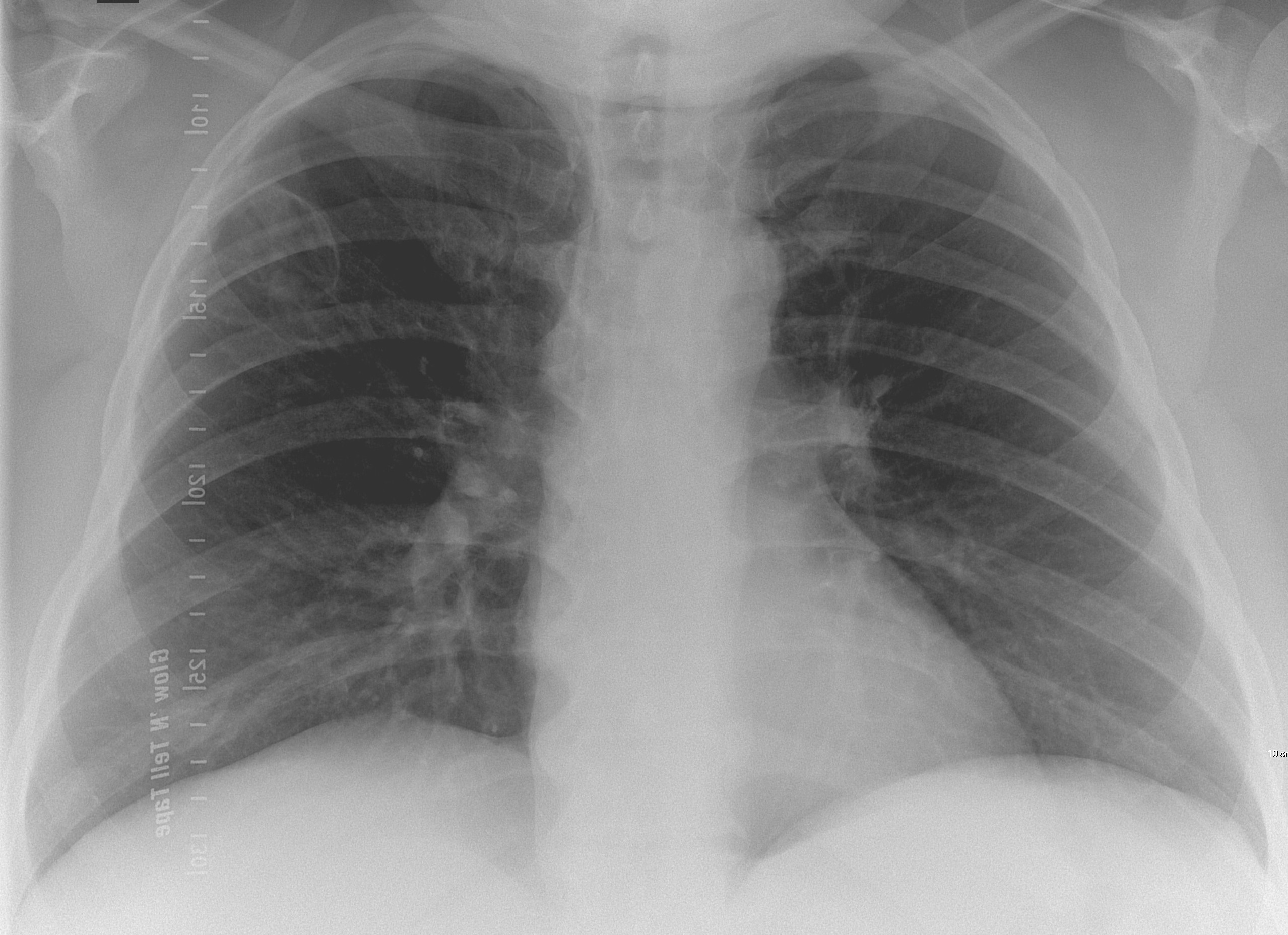
Today I am presenting a recent case, seen last January. Below is a preoperative PA chest radiograph for bariatric surgery in a 44-year-old woman. Check the image and leave me your thoughts in the comments section. I will show more images on Wednesday, followed by the final answer on Friday.
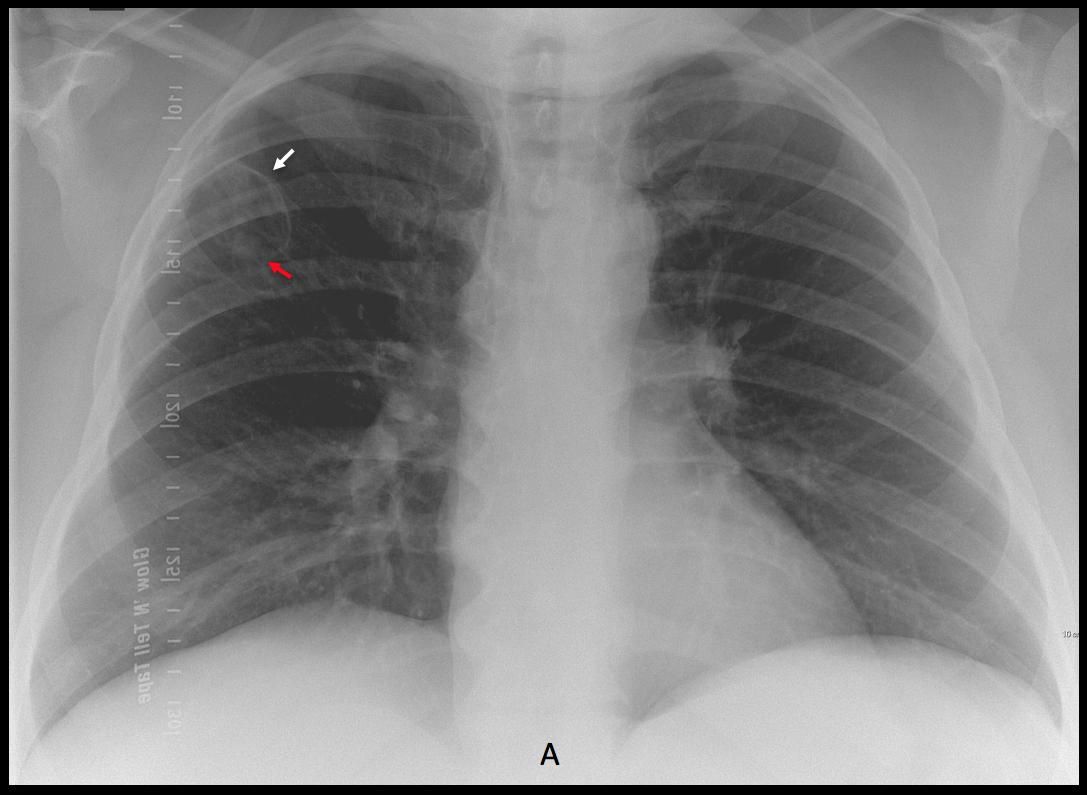
Findings: the preoperative PA chest radiograph shows a thin-walled cavity in the RUL (A, arrow) with a small nodule inside (A, red arrow).
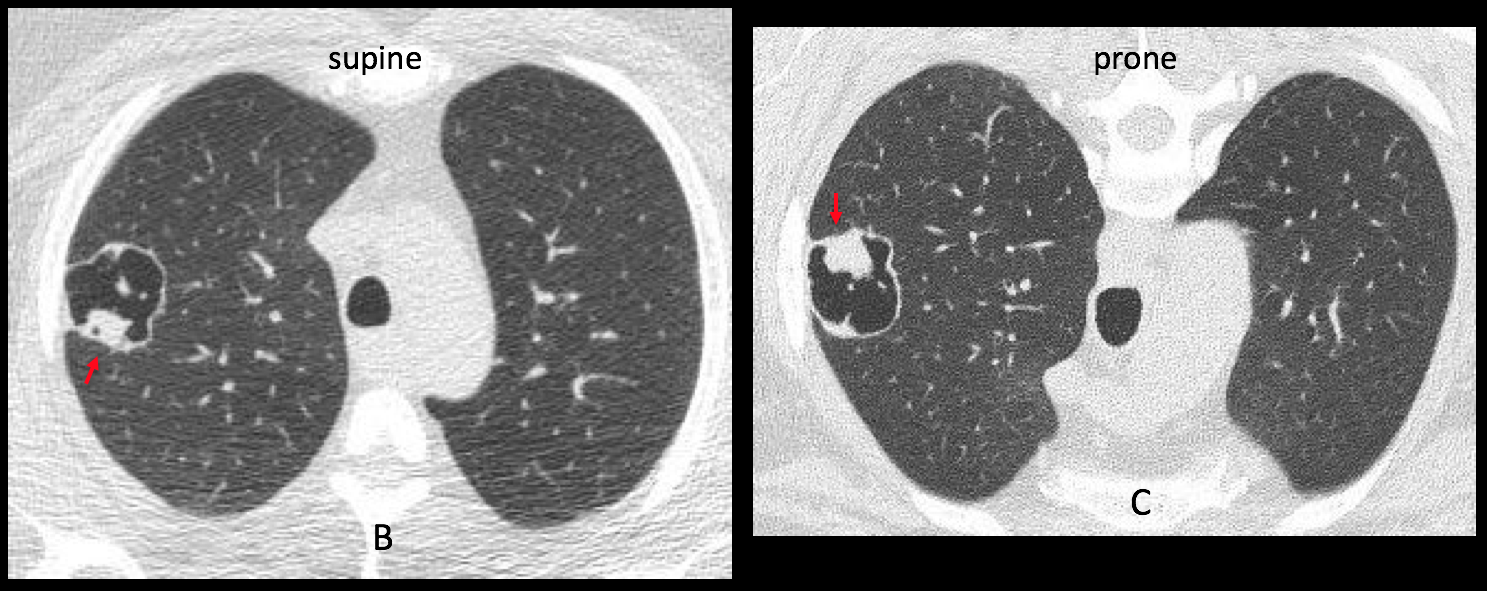
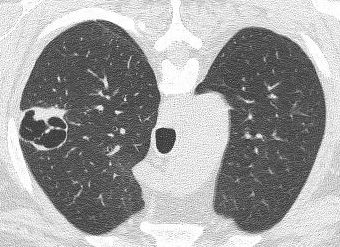
Axial CT confirms the thin-walled cavity and the nodule, which does not move in the prone position (B-C, red arrows).
An additional finding is the presence of a pulmonary infiltrate in the proximal RUL bronchus (D-E, arrows).
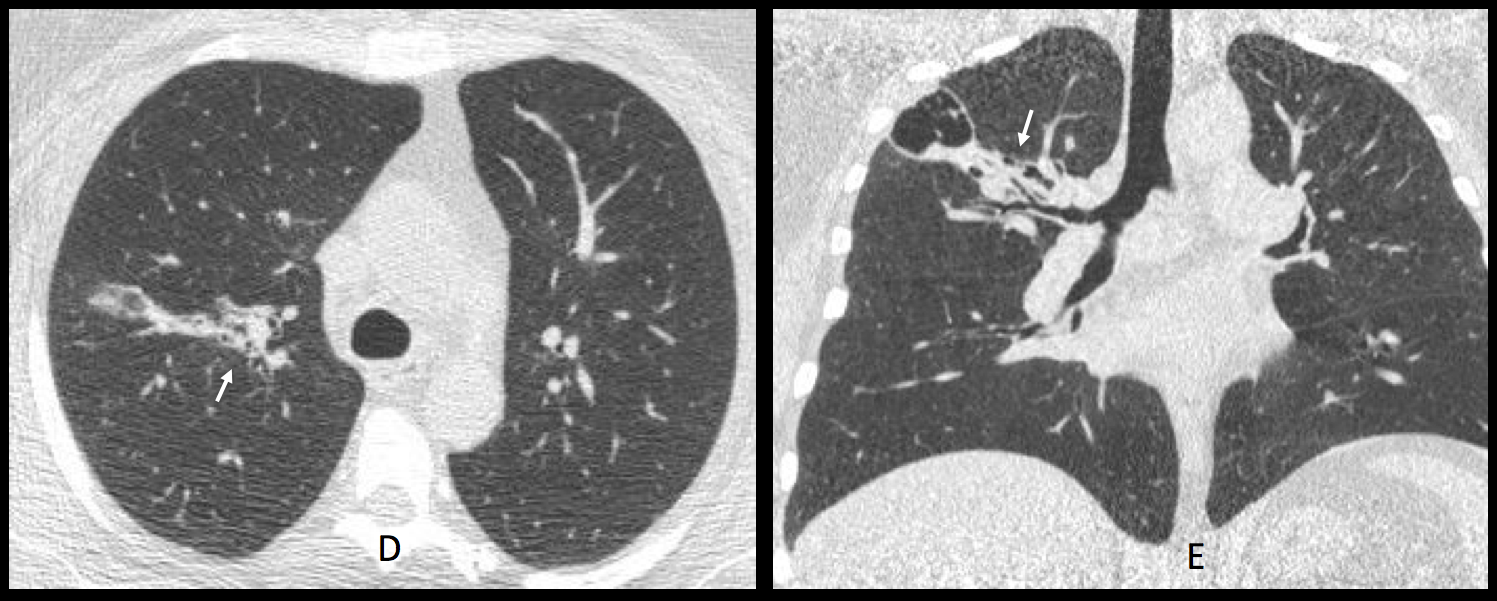
This case presents conflicting evidence: on one side, the nodule does not move, suggesting an intracavitary neoplasia. On the other hand, the thin walls of the cavity point to a benign lesion and the pulmonary infiltrate suggests an inflammatory process. In my opinion, this last finding is the one that carries more weight towards benignancy. Bronchoscopy was done and demonstrated Aspergillus in the proximal bronchi.
Diagnosis: Aspergillus infection, probably a mild form of semi-invasive aspergillosis.
This was a difficult case and I want to congratulate all the participants because all of you did your best.
Teaching point: when confronted with a case with conflicting finding, choose the one that, in your experience, is the most likely to be of help.





In right upper lung field there is cavity with irregular wall thickness. Considering the wall is mostly thin, it looks more like a benign finding.
Also there is paucity of blood vessels in right upper field, but it is probably due to contrast/brightness adjustment and doesn’t represent a pathologic finding.
ON CT I see multiple septae, and also there are mural nodules of variable thickness suspicious of cavitating magnancy, especialy indicative in fourth CT slice, where nodule extends into surrounding lung parenchima and first CT slice where thickened interstitium is seen extending to hilum.
Oval lesion in the RUL with a well defined superior margin but its inferior one is bad defined. it has hifh densities inside (calcium?)
Is the patient inmunocompromied or any history of Tuberculosis?
The x-ray lesion remembers me to a cavity aspergillus….
Really I don´t know if the lesion is intra or extrapulmonary…
It is surrounded by air; it should be intrapulmonary.
CT Wednesday.
…..aspergilloma …..
Considering that the right upper lobe image is a cystic intrapulmonary lesion the differential is very broad. It appears to have a relatively thin capsule and a mural nodule(?), also there are some parts in its interior that seem to be less Lucent than the others. I would include many many things in the differential: infectious diseases like hidatid disease and aspergilloma in a previously existing cavitary lesion, tb sequelae, pneumatocoele( maybe also infected), neoplastic lesions (primary or secundary), vasculitis, cystic bronchiectasis, bronchocoele, congenital lesions like cpam… Probably would go for a ct since it could be good or bad…
Nice discussion. CT images today.
Remarkable!!!
There is a mass in cavity that is changing it’s position,so it looks like aspergiloma..
Cavitary lesion in the RUL with thickened and irregular wall with some septum inside and a nodular lesion that dont move with the movements of the patient…
We have to rule out malignancy. If the intracavitary component will be movile it would be a fungical process (aspergillus)
RUL thin walled solitary cavitary lesion with mural nodule which is not declive in prone position (aspergilloma excluded)
Some vessels seems to be in contact with the lesion all suggestive of pseudo aneurysm (ex Rasmussen Aneurysm) have to be confirmed in soft tissue window with contrast
Malignancy can not be excluded in absence of contrast study
Hello and thank you for this case. Given that the patient is asymptomatic without any specific history and this lesion was merely found on a preoperative chest Xray, I tend to think about benign etiologies. Could this be a localised cystic bronchiectasis or some congenital malformation? Aspergilloma is unlikely since the mural nodule is well attached. Cavitating lung cancer remains possible as a diagnosis.
Hello, it looks like mycetoma (fungus ball)
Cavitary lung lesion seen at the apical segment of the Upper lobe RT lung. Cross sectional CT scan in supine & prone position revealed immobile mural nodule attached to the posterior aspect of the cavity, the picutre is likely suggestive of malignant process.
CXR: Lung cavitary lesion, with linear and thin wall, and a basal nodular lesion inside it.
CT: Lucent lesion seem to have septae, and prone position shows that the nodule is attached to the wall.
At first, I think about an emphysematous lesion, with an aspergyloma inside, but, now I am considering a complicated (neoplasic??) sequestration.
(Sorry the bad English)
Your discussion is correct and I was thinking about the same lines. Your English is also correct. Mine is no better! ,-)