Muppet cannot find difficult cases and, despite himself, is forced to show easy ones. Today we’re showing radiographs of a 48-year-old woman who has had moderate dyspnea for a while.
1. Swyer-James syndrome
2. Tumour left main bronchus
3. Old TB left lung
4. None of the above
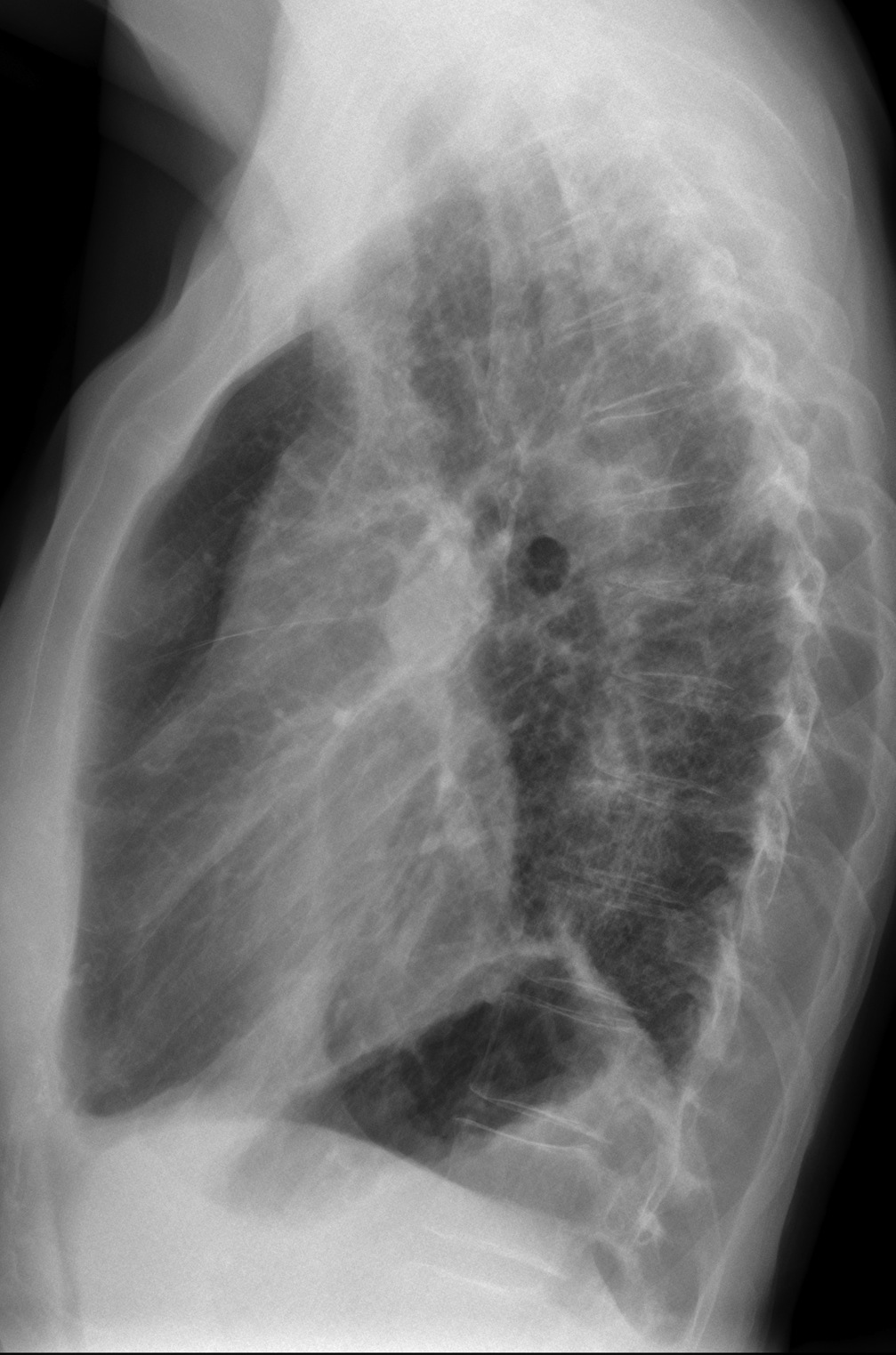
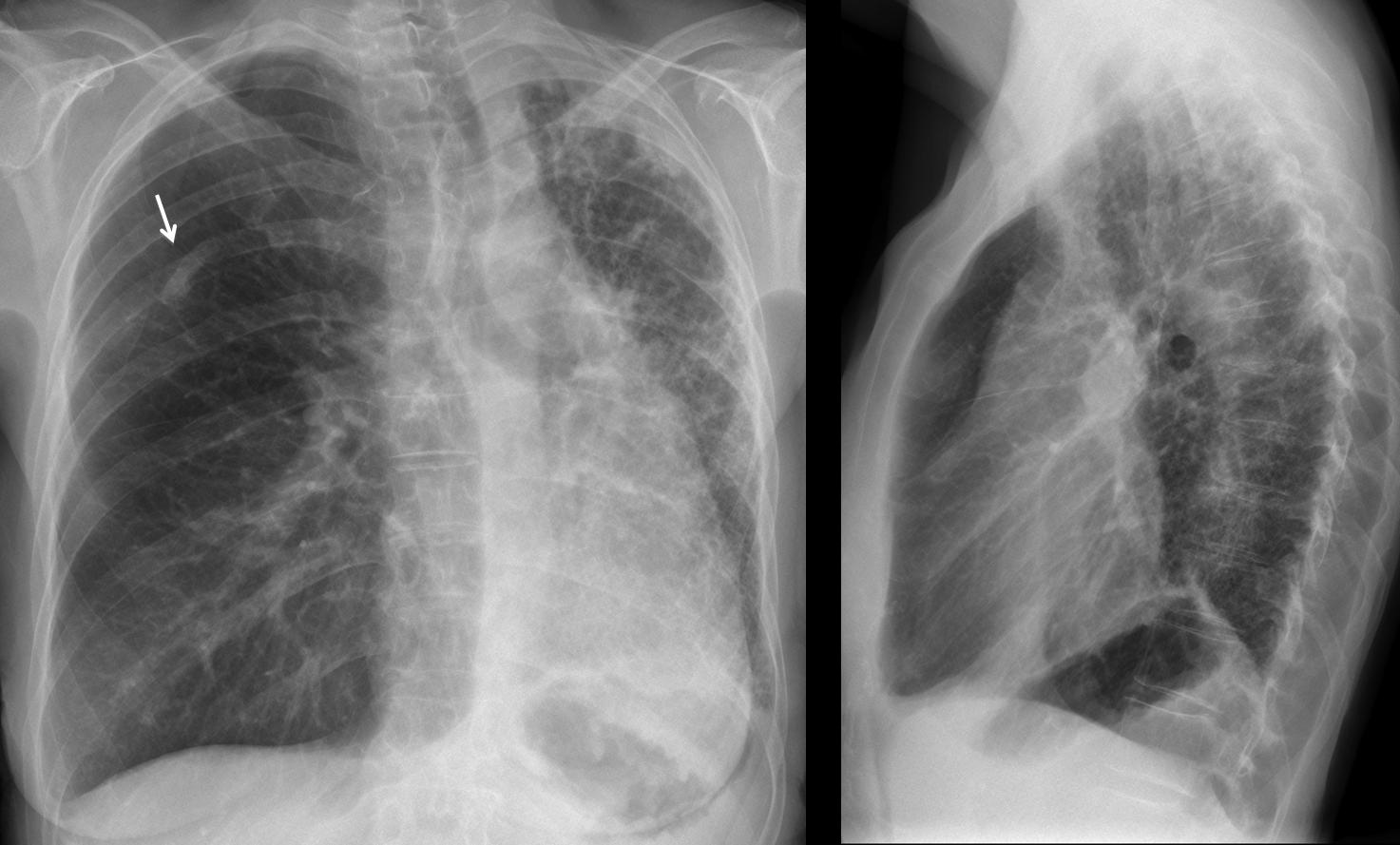
Findings: PA and lateral radiographs show a small left hemithorax with diffuse lung disease. Right lung is expanded and mediastinal structures are displaced towards the left. Obviously, the diseased lung is the left one. This raises the question of why the right lung is spared. And the answer is very simple: the right lung is OK because it is transplanted. A clue to the diagnosis is the surgical fracture of the right 6th rib (arrow).
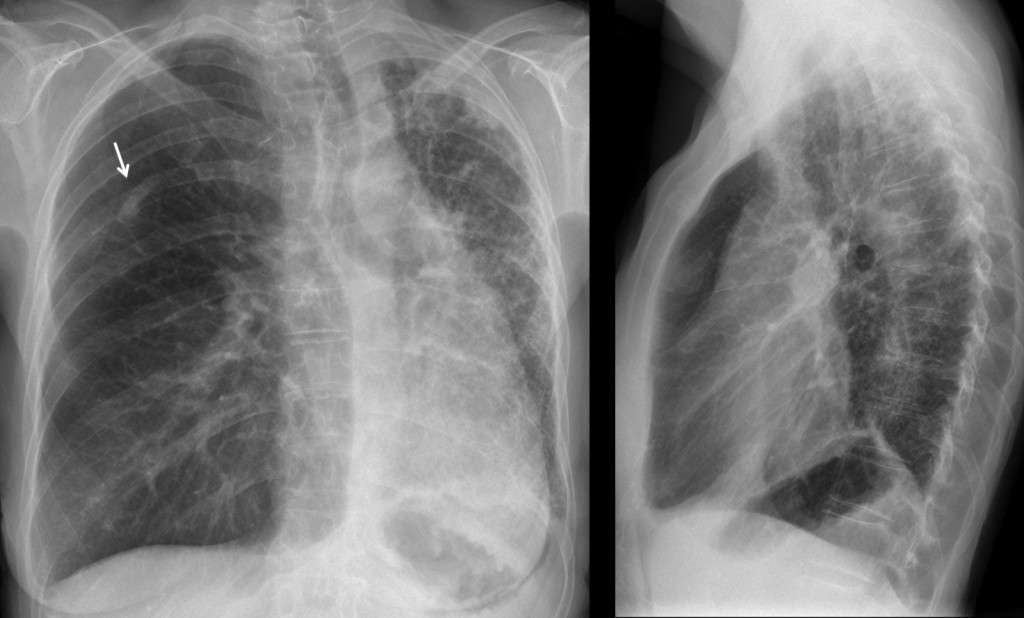
Fig. 1
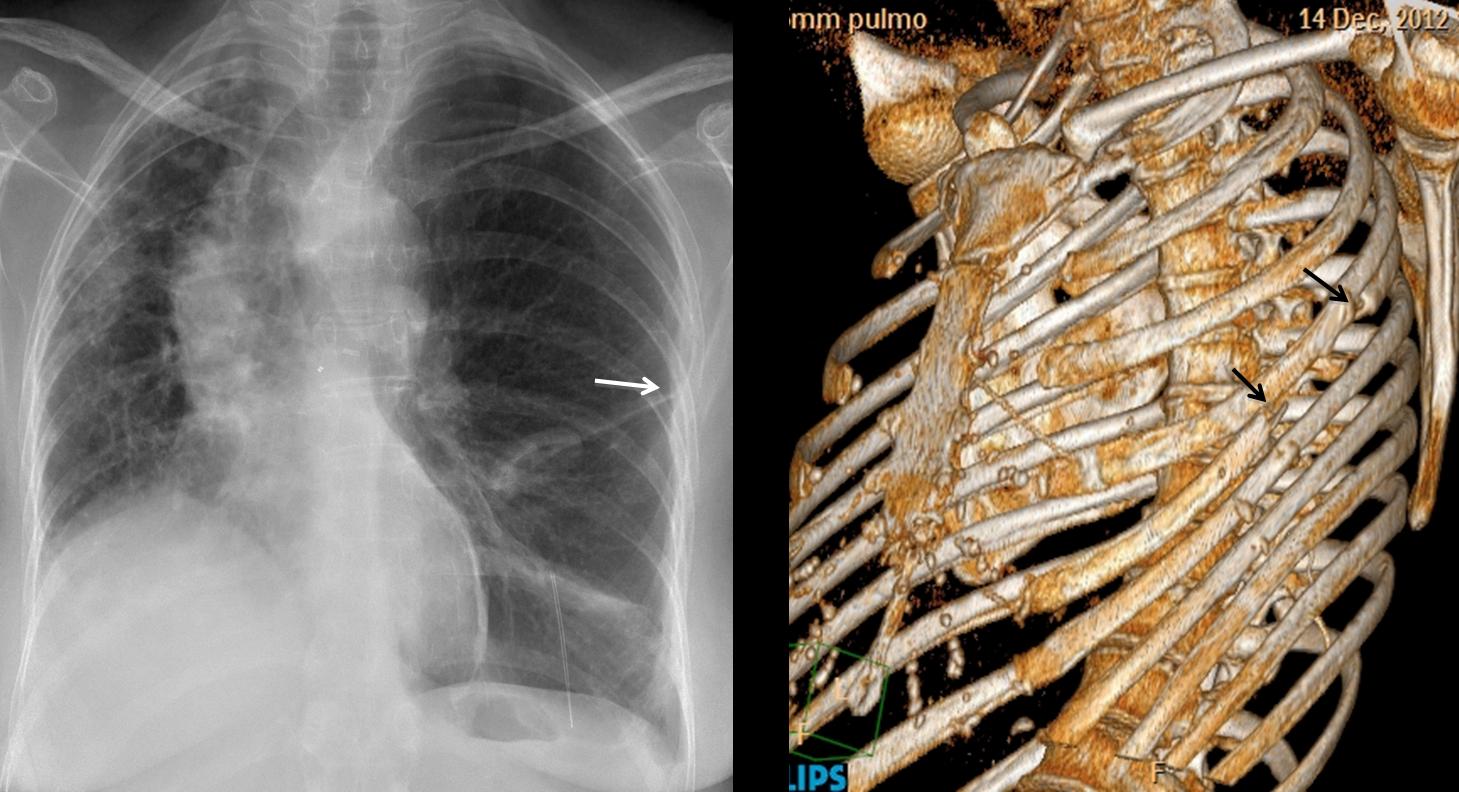
I wanted to show the typical appearance of a condition that it is not uncommon. About 4,000 lung transplants are performed each year; 1,677 of them in the European Union. Knowing this appearance (they all look the same, see Fig. 2) will prevent errors, especially if you are taking an examination.
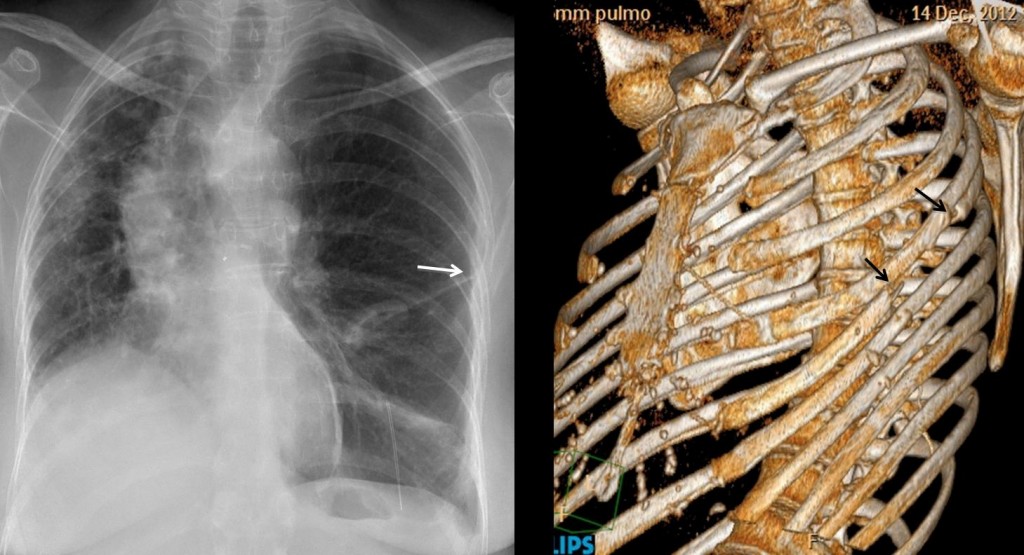
Fig. 2. Left lung transplant. Note post-surgical changes in the left 5th rib (arrows)
Final diagnosis: right lung transplant
Teaching point: When seeing a unilateral hyperlucent lung, consider a previous transplant.
In any patient, isolated fractures of 5th or 6th ribs should raise the question of previous surgery.



PA film shows loss of volume in left hemithorax with ipsilateral mediastinal displacement and diaphragm elevation. There is a reticulonodular pattern in the parenchima representing chronic lung damage. Maybe some bronchiectasias?( I cannot see them well)
Lateral film shows right pulmonary hilium anterior to the trachea but no left hilium is seen. So, my diagnosis: congenital absence of left pulmonary artery.
Swyerjames syndrome
Volume loss of left lung, but left lung vascular structures seem normal or at least not clearly reduced. I think left pulmonary artery Is visible on the lateral. Consolidation of lul in apex of the left lung and reticular opacities in left lower lobe. Compensatory hyperinflation of right lung.
No pulmonary or mediastinal calcifications. No pleural effusions.
Old rib fracture on the right.
I am against old TB (no calcifications) and Swyer James Syndrom (age of patient, changes of left lung not exactly fitting).
I choose 2. Tumour left main bronchus because of lul volume loss as a main finding.
In lateral view I can’t identify shift of the fissures what say against tumour. It doesn’t look atelectasis. I think Gotzon is correct. congenital absence of left pulmonary artery would explain a small left lung with no signs of air trapping.
Sorry to insist. To identify air trapping you need inspiration and expiration films.
I think I used a wrong word. I wanted to say is that there’s no hiperlucent lung as we expect in Swyer James. And I’m not sure if there’s volume loss in left lung. I think it is a small lung with no atelectasis.
positive findigns:
1. definite volume loss (ipsi mediastinal shift and elevated left dome) of left lung due to fibrosis
2. left lung shows frank dirty reticular markings with few upper zone linear bronchiectasis
3. definite left apical pleural thickening (quite irregular)
4. compensatory overinflation of the right lung (upper-mid zone lucency with spaced out vessels)
5. vertebrae are osteopenic for a 48 year old and an incidental old fracture of the right sixth rib posteriorly
negative findings: relevant
1. no obvious nodules / calcifications / cavities / pleural effusion / hilar nodes
from above discussion this CXR is still most probably >
3. old kochs left lung
also of note is that in sawyer james the lung with volume loss is more lucent (which is reverse here with the left lung)
and no bronchial tumor should cause bilobar parenchymal reticularity; otherwise as well the lack of a hilar mass, and atleast a resultant segmental consolidation (the golden s sign) are lacking.
Il professore dice che il caso è semplice: ma non sarà una trappola( come quella che hanno preparato il Milan ed il Real per il”desaparecido” Messi? Auguri comunque per la “remuntada”).Si esclude la S. S-James, perchè a dx, non c’è perdita di volume polmonare ed a sx non c’è rarefazione della trama vascolare.Il cr del bronco principale di sx si deve escludere perchè in LL si vede bene la sua immagine libera. Ci sono i segni di pregresse lesioni pleuro-polmonari a sx che possono essere aspefiche( escludo la TBC). Il polmone dx è iperespanso, per compenso ed ernia controlateralente. Vi è una opacità triangoliforme con base sul diaframma(in LL), che sembra contenere immagini bronciectasiche , da trazione, in un segmento atelettasico , che corrisponde al territorio della lingula. Risposta finale:4.
Alice mentioned the old fracture of the right sixth rib. Does it help you with the case?
There is still the probable operative intervention in a right upper lobar segment which could be neoplastic or even a cavity of tuberculosis..
So 3: old kochs left lung still stays my primary choice as I elaborated above ..
But if I have to choose another differential then maybe lymphangitis carcinomatoses can explain some features of the left lung changes ..
old post primary TB
While considering the clue concerning the rib I noticed apparent slight antelisthesis of T7, for what its worth…
possibly an old pathologic fracture on basis of a metastasis or post-surgery (but no surgical clip material visible).
the consolidation in apex of left lung seems to be mostly pulmonary (especially on the lateral where it is better visible.
no. 2 seems unlikely i have to agree because of inflation of left ll.
but what about a malignant disease after treatment (radiation pneumonitis in apex of ll?l) – another cause of volume reducing consolidation would be chronic organizing
pneumonia, but that seems totally unlikely.
Adenocarcinoma with lepidic growth does not leed to volume loss I guess.
I am really looking forward to the solution.
What do you think of when seeing a fracture of the 5th. or 6th. rib?
well, my first thought is a singular metastasis.
primary bone tumours are rare.
other causes like inflammatory diseases or hormonal diseases seem even more unlikely.
breast carcinoma is a possibility, but both breasts are visible without obvious post-surgical changes.
no other suspect bone lesions.
if it was a metastasis the opacities on the left could be therapy-related.
lymphangitic spread without pleural effusion seems less unlikely.
still haven’t got a clue unfortunately. ;-(
Myself, when I see a fracture of 5th/6th rib, think that the patient has been operated on
Do you really? 🙂 I am wracking my brain over this…
The right lung is the supposedly “normal” one.
Maybe minimal invasive surgery and wedge resection?
Avevo avvertito i colleghi della “trappola” del “galactico blau-grana”( sta andando male , terza sconfitta di seguito!):il caso non era facile. Se la chiave di lettura è la 6 costa di dx, quello che vedo anomalo in essa è il tipo di consolidamento, con monconi non in asse, ma a cuneo con monconi sporgenti all’interno: questo potrebbe spiegare una complicanza della frattura costale, con lacerazione polmonare e conseguente idro.pneumotorace ipertensivo.Si spiegherebbe l’iperespansione polmonare ,”bloccata” da aderenze-briglie pleuriche-cicatriziali.
This could make sense:
Left lung is fibrotic, native.
Transplanted right lung.
Yes
Very interesting case, professor. Congratulations Dr Strangelove with the hypothesis of right lung transplant. It’s important to observe that there’s no evident sign of left atelectasis that would favor tumour.
In our institution we do a fair amount of transplants. The appearance is so typical that I wanted to show a case.
L’avevo detto che era un caso-trappola!Complimenti mitico Professore ed auguri per la “remuntada”!!!!
It was a “piccola trappola” but a learning case. And Barcelona is out of the race!
Don’t get me wrong, but if I had this xray without the information of a prior lung transplantation I would call the referring doctor and ask him if he’s crazy not providing me an information like that!