Today we’ll start the second part of The Beauty of Basic Knowledge series, titled ‘To err is human: how to avoid slipping up’. In the next six chapters I intend to analyse the most common causes of errors in chest imaging and how to avoid them. As Cicero said: All men can err, but only the ignorant persevere in the error.
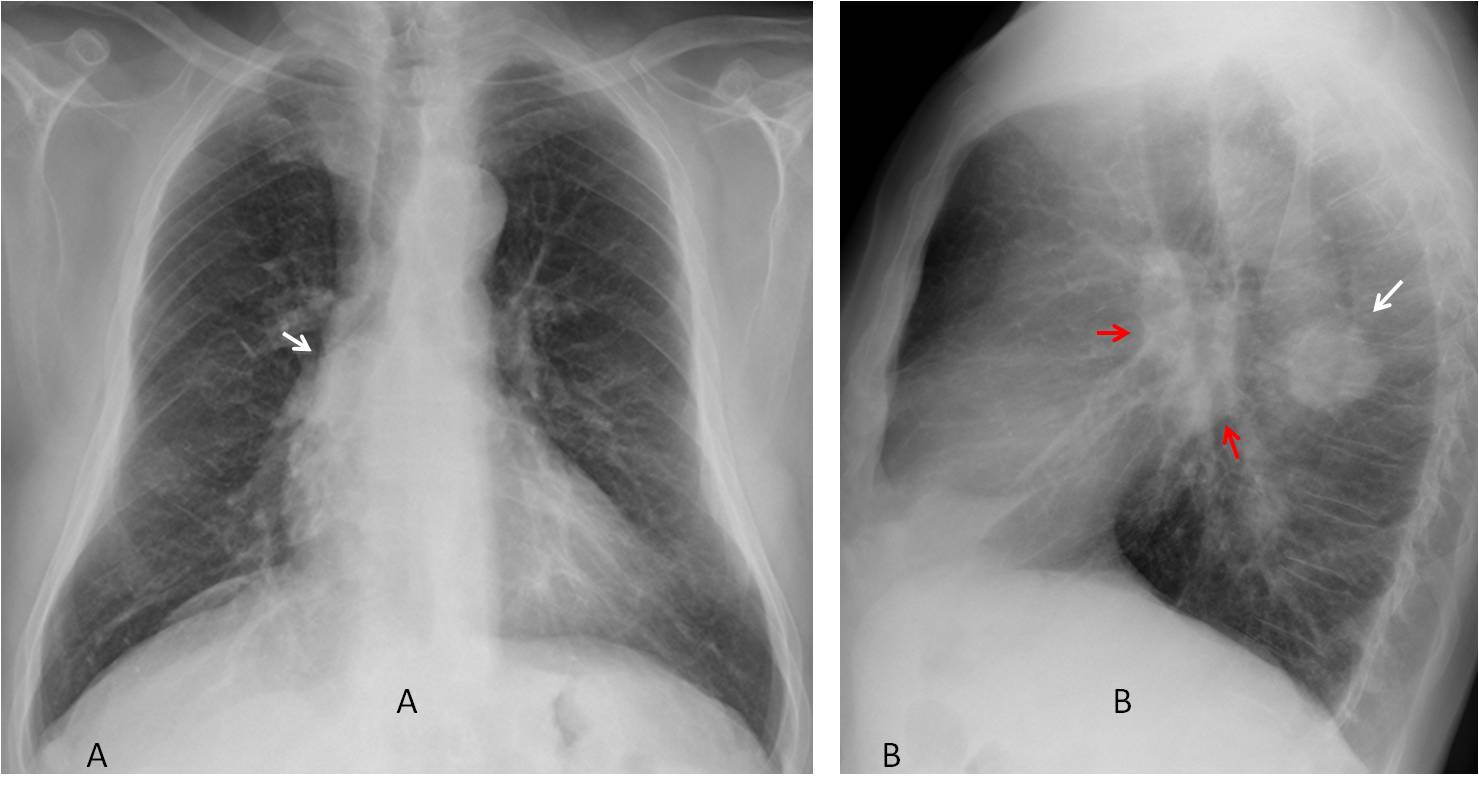
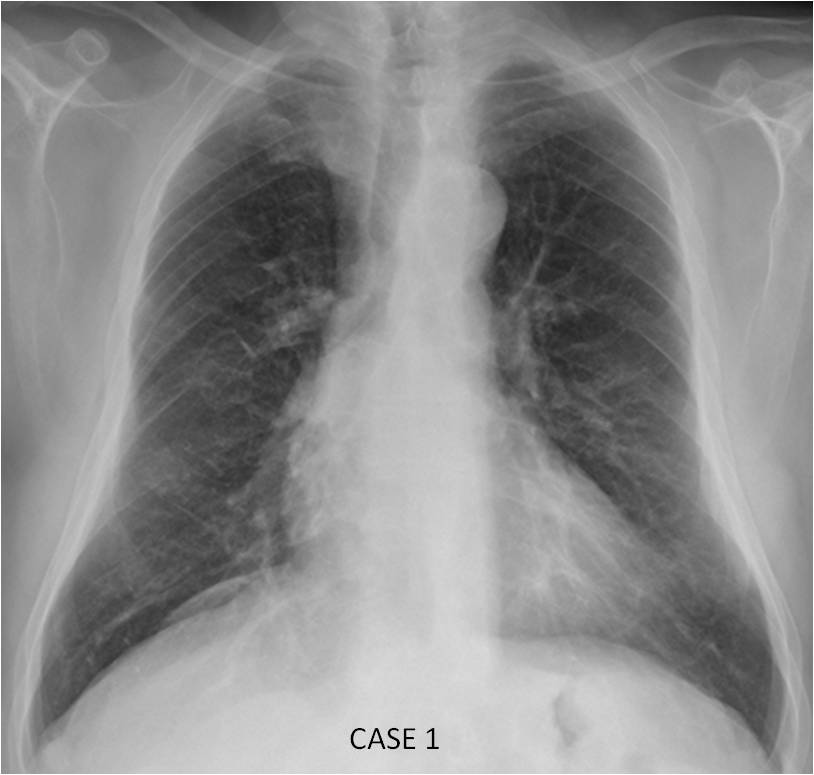
This week I am presenting two cases. Case 1 shows the PA radiograph of a 57-year-old man with a cough. Would you say the chest is normal?
1.Yes
2.No
3.Need a lateral view
4.Need a CT
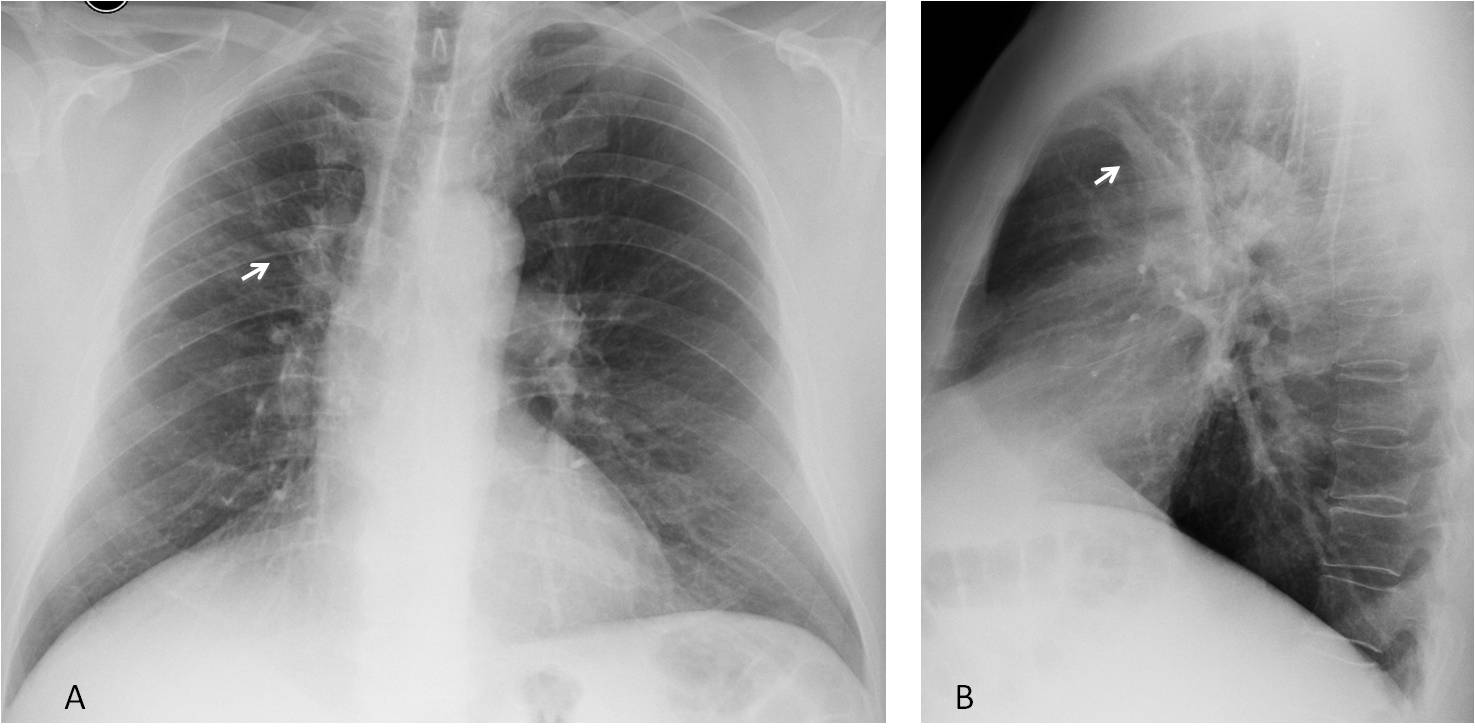
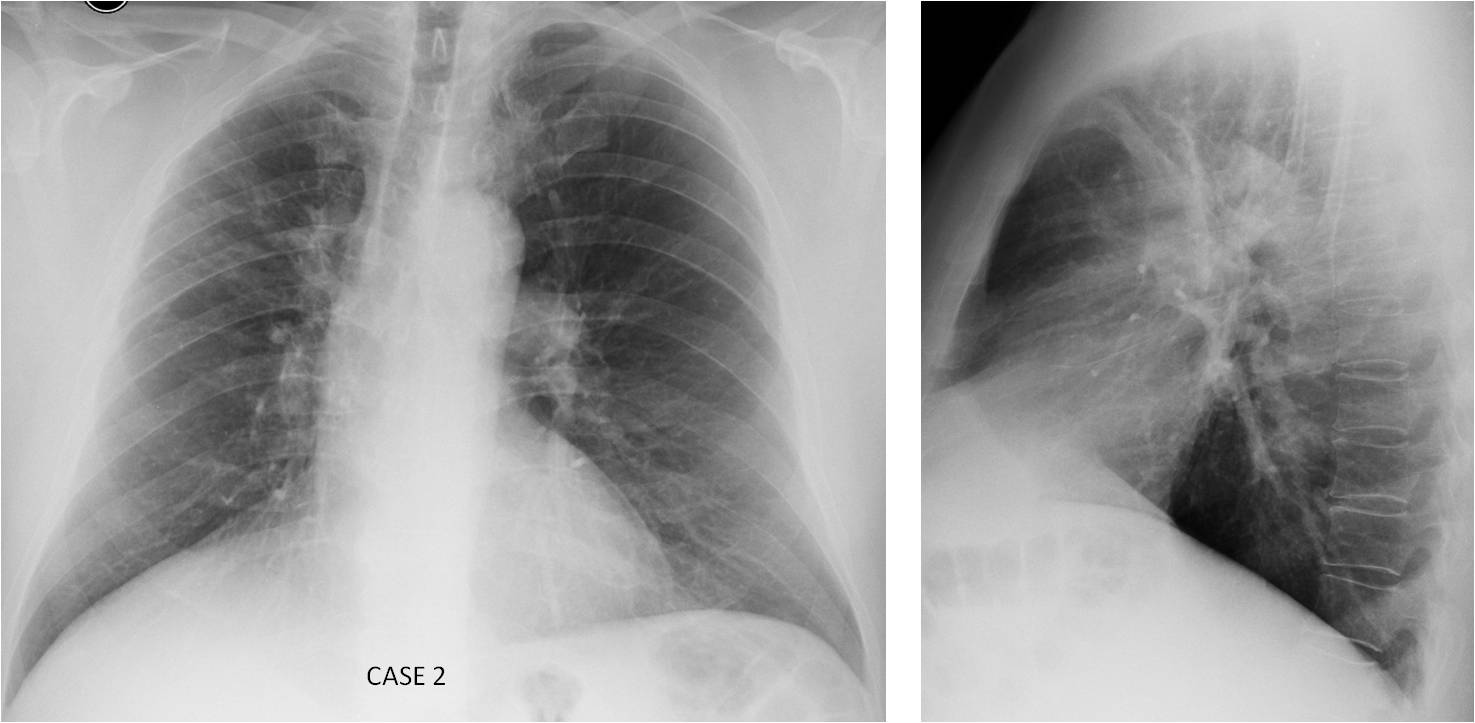
Case 2 presents PA and lateral radiographs of the yearly check-up of a 70-year-old man. CT done in another institution was reported as chronic post-TB changes. Do you agree?
Check the images below, leave your thoughts in the comments section and come back on Friday for the full solution!
Case 1. Findings: PA radiograph shows increased opacity of the right hilum (A, arrow). A lateral view taken hours later shows a rounded nodule in the apical segment of the RLL (B, white arrow). In addition, there is a hilar donut sign (B, red arrows), highly suspicious of enlarged lymph nodes.
Enhanced axial CT confirms the nodule (C, white arrow) as well as subcarinal lymph nodes (C, red arrow). PET-CT shows marked uptake of both (D, arrows).
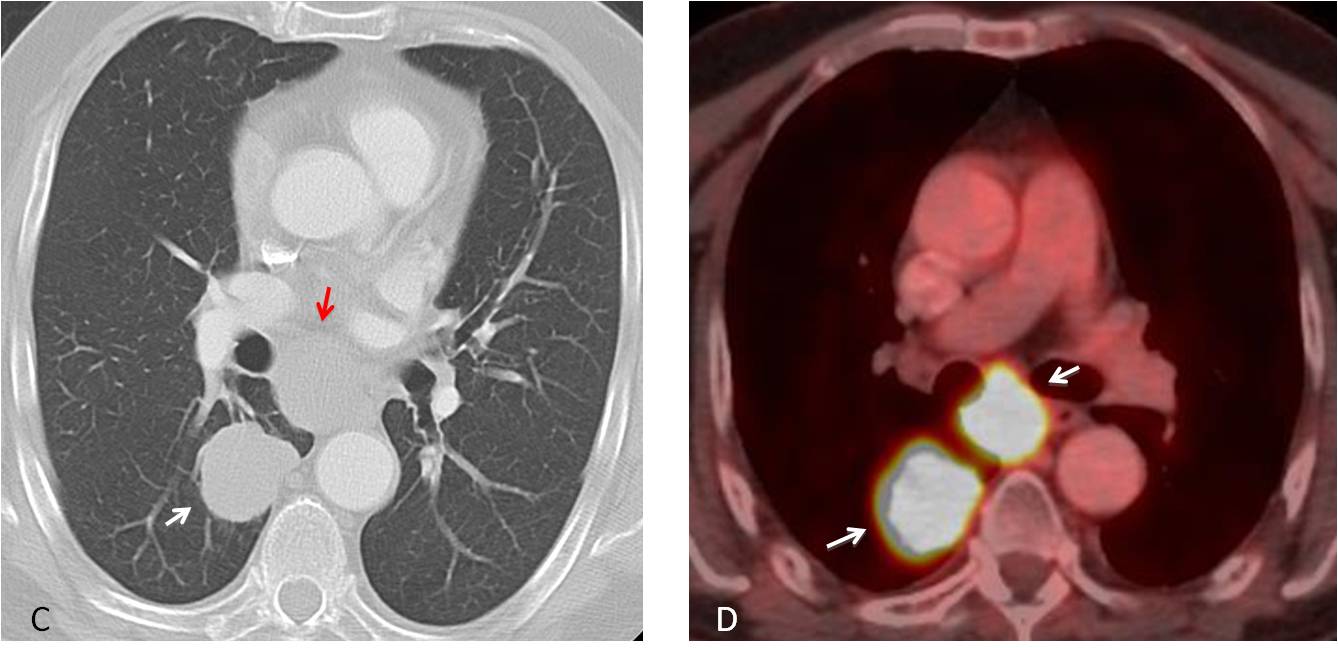
Final diagnosis: Carcinoma of RLL hidden by the right hilum in the PA view, with metastasis to subcarinal lymph nodes.
Case 2. Findings: PA radiograph shows a nondescript infiltrate in the RUL (A, arrow), with probable elevation of the right hilum. The infiltrate is located in the anterior segment of the RUL in the lateral view (B, arrow). This location is unusual for TB, which tends to involve the apical or posterior segments of the upper lobe.
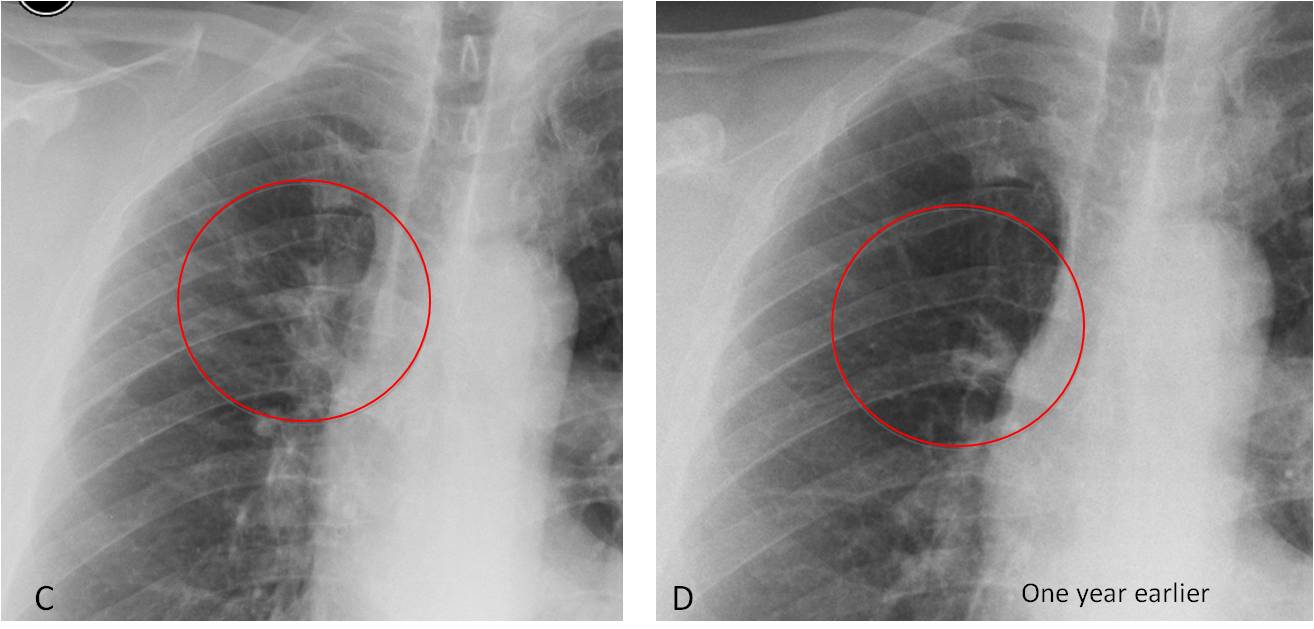
Comparison with a previous radiograph taken one year earlier demonstrates that the RUL was normal at that time (C and D, circles). This finding ruled out chronic changes post-TB and prompted a revision of the external CT.
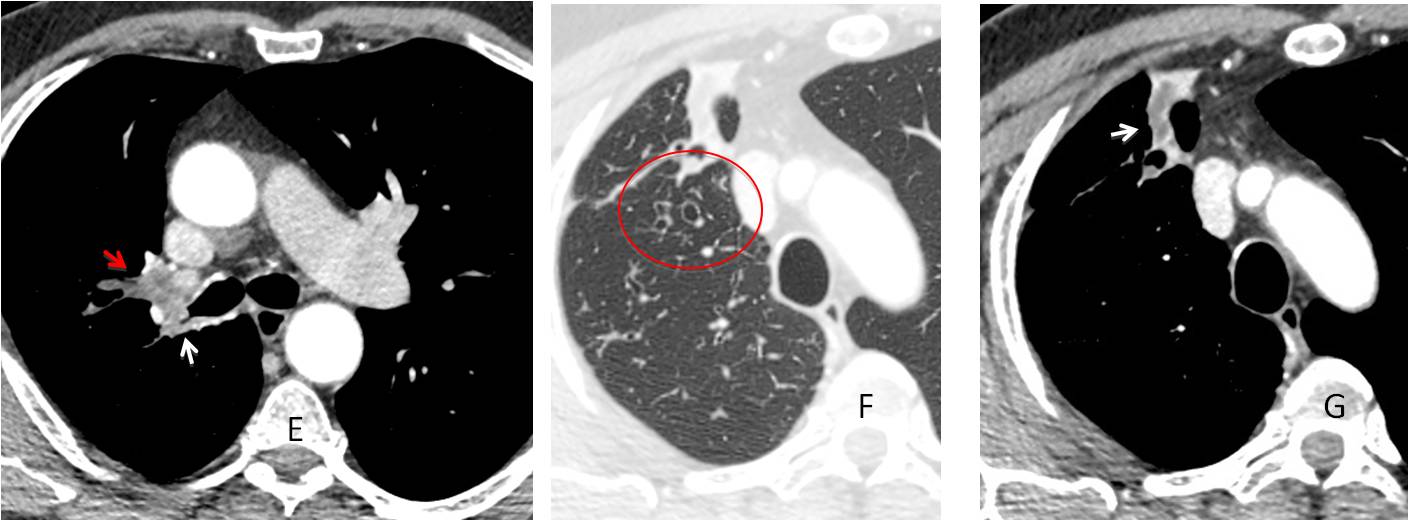
Enhanced axial CT showed narrowing of the RUL bronchus (E, white arrow) and a mass (E, red arrow). CT with lung window shows dilated bronchi (F, circle). Mediastinal window depicts a distal mucus impaction (G, arrow). The findings are highly suggestive of carcinoma of the RUL with obstruction.
Final diagnosis: Carcinoma of the RUL bronchus diagnosed erroneously as chronic TB changes because previous films were not examined.
Errors in diagnostic imaging are not uncommon and the radiologist is responsible for most of them. In the next six chapters I intend to analyze the most common causes of errors in chest imaging and how to avoid them.
Basically, diagnostic errors can be classified into four categories:
1. Methodological errors
2. Errors of visualization (perceptual errors)
3. Errors in interpretation
4. Communication errors
In this chapter I would like to address methodology errors. As was seen in Cases 1 and 2, the most important are:
a) Failing to obtain a lateral chest view
b) Neglecting to look at previous films
These two errors are easily corrected by doing the right thing.
Failing to take a lateral radiograph is, in my opinion, a capital sin. About 25% of the lung parenchyma is obscured by other structures in the PA view, mainly the mediastinum and diaphragm (Fig. 1). If we include the sternum and spine, which are only visible in the lateral view, it is evident that more than one fourth of chest conditions may not be visible in the PA film.
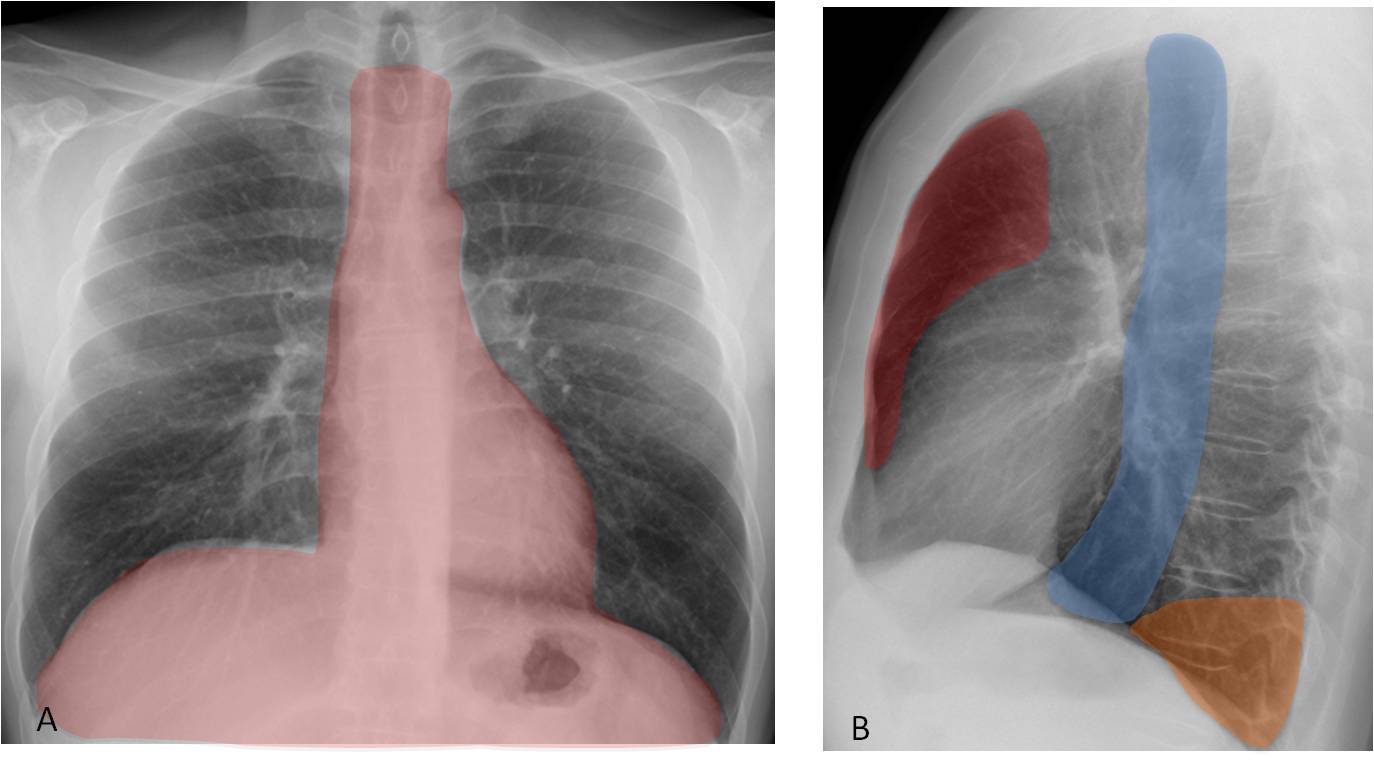
Fig. 1
Fig. 1. Shaded areas in the PA radiograph (A) obscure about 25% of the lung parenchyma. The obscured areas are represented in the lateral view by the anterior clear space (B, red), middle mediastinum (B, blue), and posterior clear space (B, orange).
The two main advantages of taking a lateral chest radiograph are
1. To discover conditions hidden in the PA view (Fig. 2) and
2. To clarify inconclusive findings in the PA view (Fig. 3).
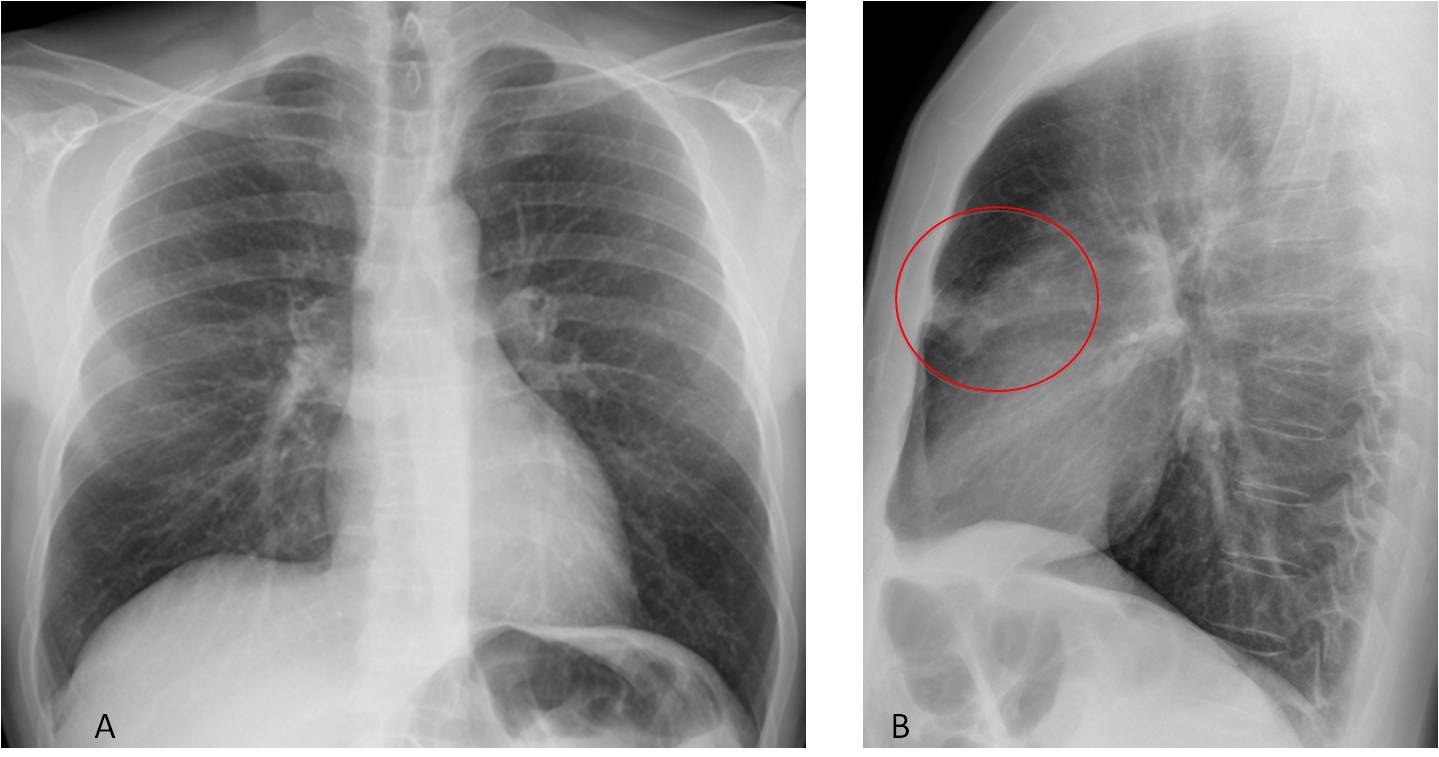
Fig. 2
Fig. 2. 42-year-old man with fever. PA chest film (A) is unremarkable. Lateral view shows a poorly-defined infiltrate in the anterior clear space (B, circle). Diagnosis: pneumonia.
Chest lesions may present an oblique interface to the X-ray beam in the PA projection and become indistinct. In these cases the lateral view better depicts the appearance of the lesion, facilitating the diagnosis (Fig. 3).
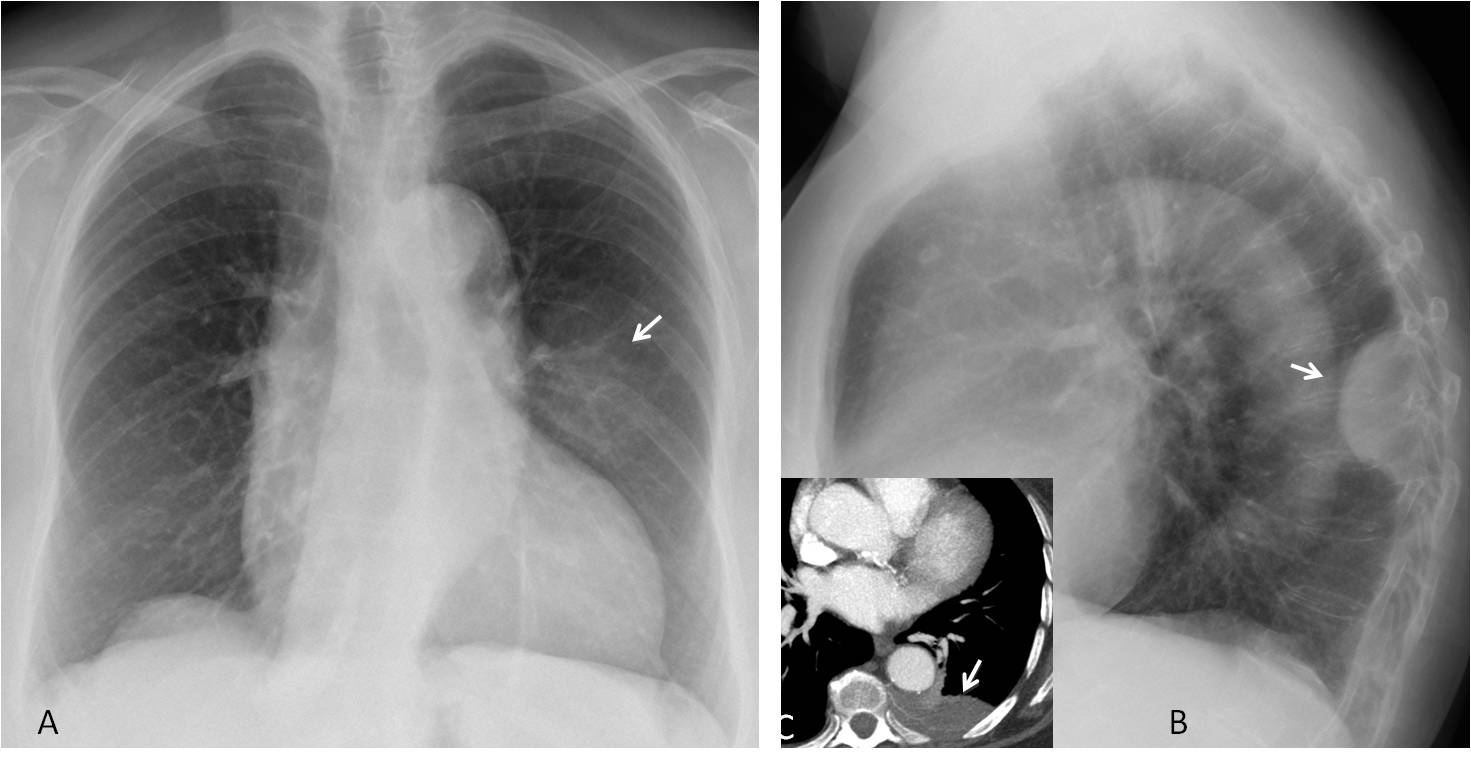
Fig. 3
Fig. 3. 63-year-old woman with chest pain. The PA radiograph shows a poorly-defined opacity in the left hemithorax (A, arrow) that seems to be located in the lung. The lateral view shows a typical posterior extrapulmonary lesion (B, arrow), confirmed with CT (C, arrow). Diagnosis: chest wall lymphoma.
In my opinion, comparison with previous films is extremely useful in the diagnostic process. Review of previous radiographs has been judged valuable in up to 89% of cases.
In the old days we had to look at previous radiographs one by one. Now, with the availability of PACs, it’s inexcusable not to look at previous examinations. It’s no trouble and can save your behind more often than not.
Previous images are mainly used to document progression, regression, or stability of disease (Figs. 4 and 5).
A classic example of the usefulness of previous films is the solitary pulmonary nodule. The most reliable criterion on plain films is nodule growth (or lack of it). For that reason, it is essential to compare with previous films, when available. A nodule that has grown in the interval is probably malignant and should be acted upon (Fig. 4).
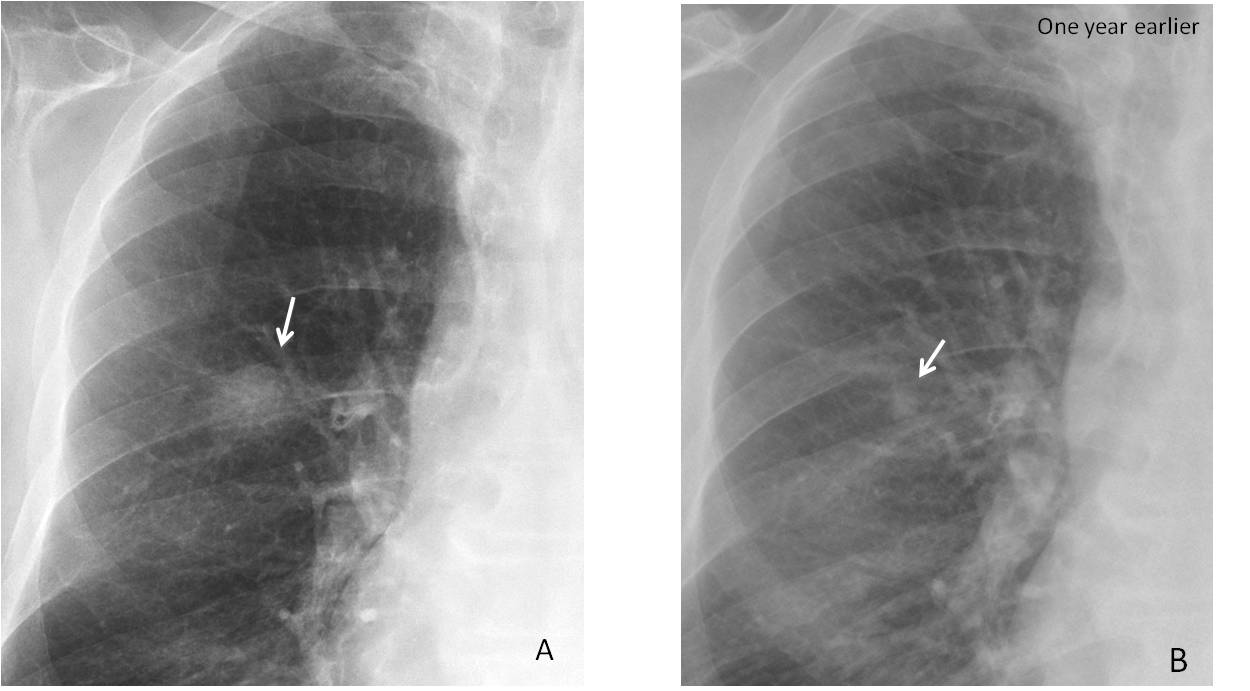
Fig. 4
Fig. 4. Indeterminate nodule in the right lung (A, arrow). Plain film one year earlier shows the nodule, which was considerably smaller (B, arrow) and missed at that time. Diagnosis: adenocarcinoma
No changes in a solitary pulmonary nodule over a two-year period is a reliable indication of benignancy and avoids invasive procedures (Fig. 5).
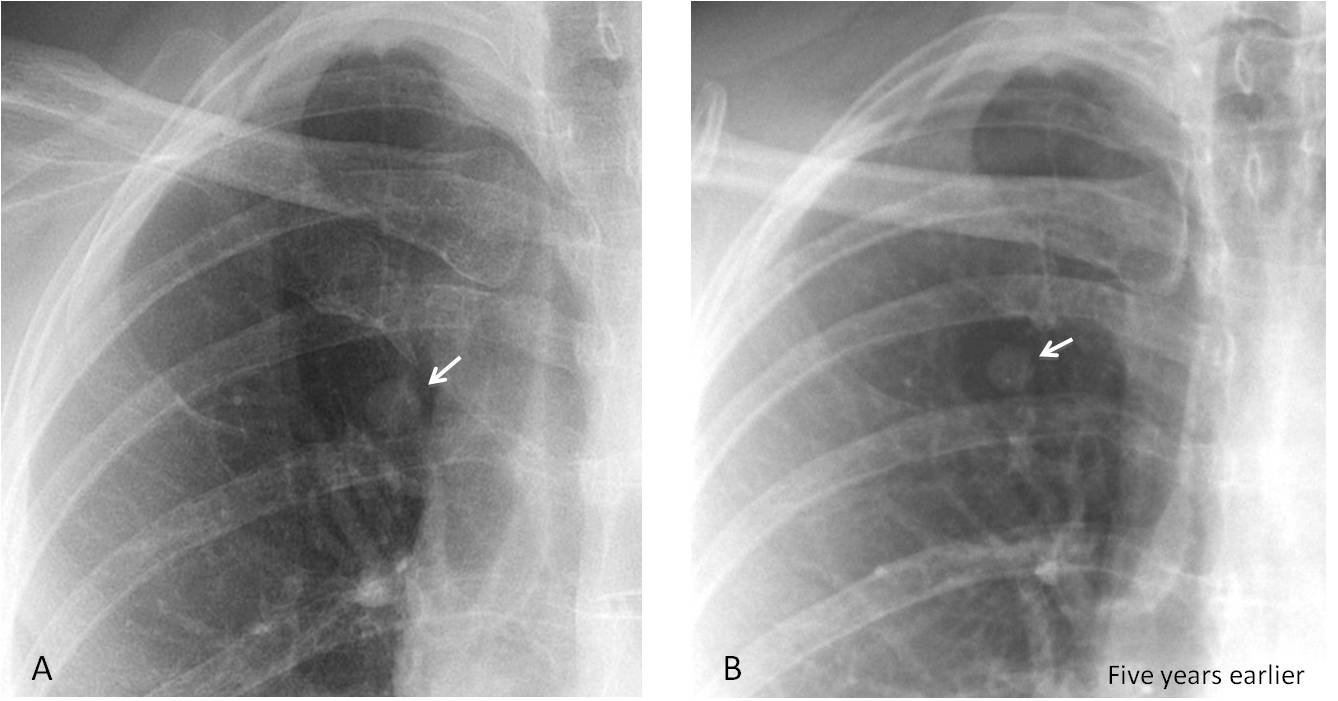
Fig. 5
Fig. 5. Preoperative radiograph for hernia surgery in a 54-year-old man, depicting a solitary nodule (A, arrow). Comparison with a previous film shows that the nodule was present five years earlier and has hardly increased in size, confirming benignancy (B, arrow). Review of the previous report discovered that the nodule was missed in the initial examination!
Other times, comparison with previous radiographs helps to arrive at an immediate diagnosis, precluding the use of unnecessary and more expensive examinations (Figs. 6 and 7).
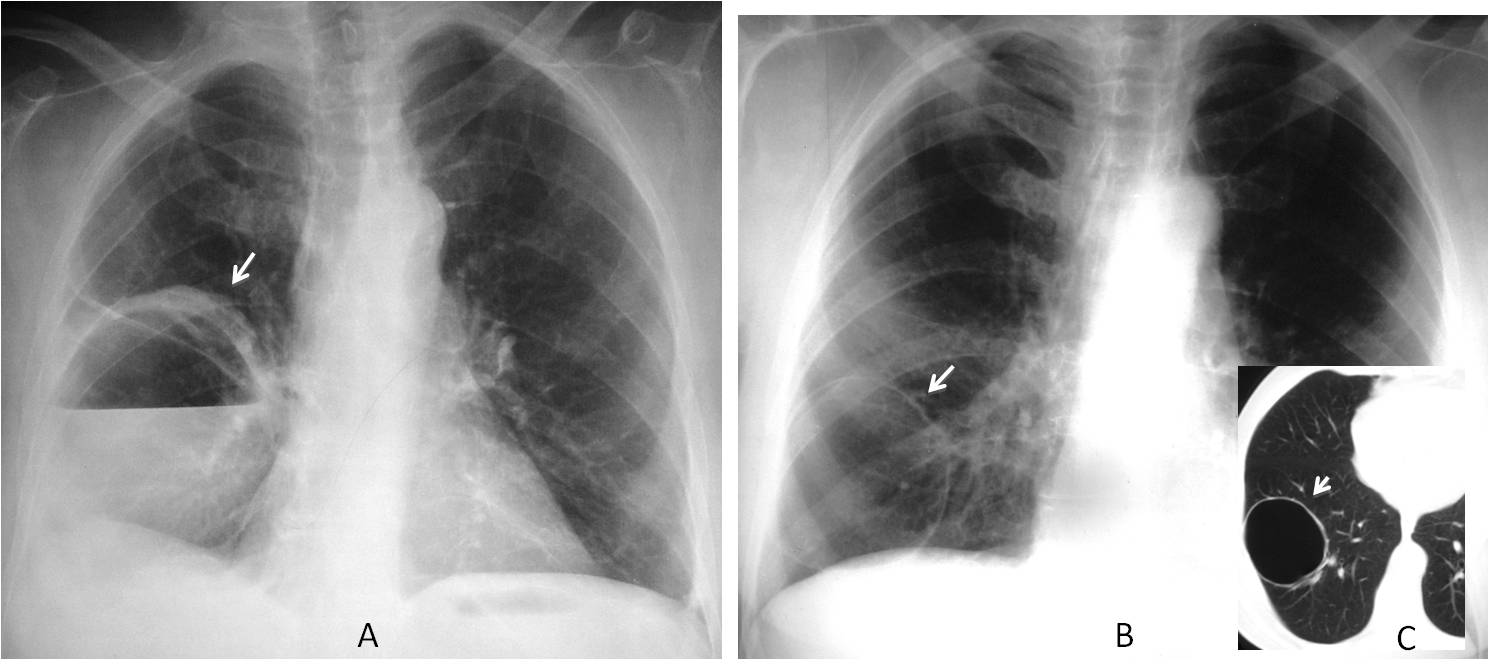
Fig. 6
Fig. 6. 45-year-old man with high fever. PA radiograph shows a large mass in the RLL with and air-fluid level (A, arrow), which could be an abscess or a tumor. Comparison with previous films taken five years earlier shows a thin-walled cyst in the same location (B and C, arrows). This finding confirms the diagnosis of a lung abscess in a previous cyst.
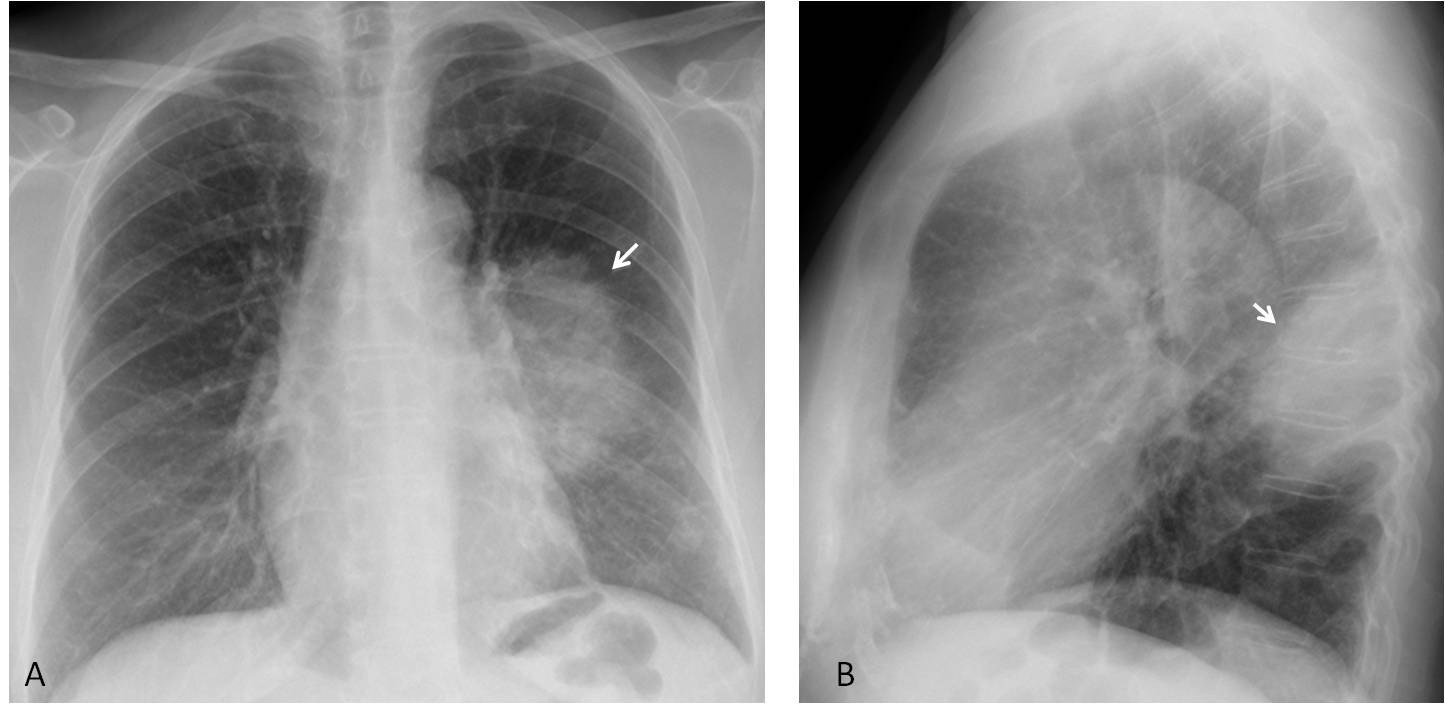
Fig. 7
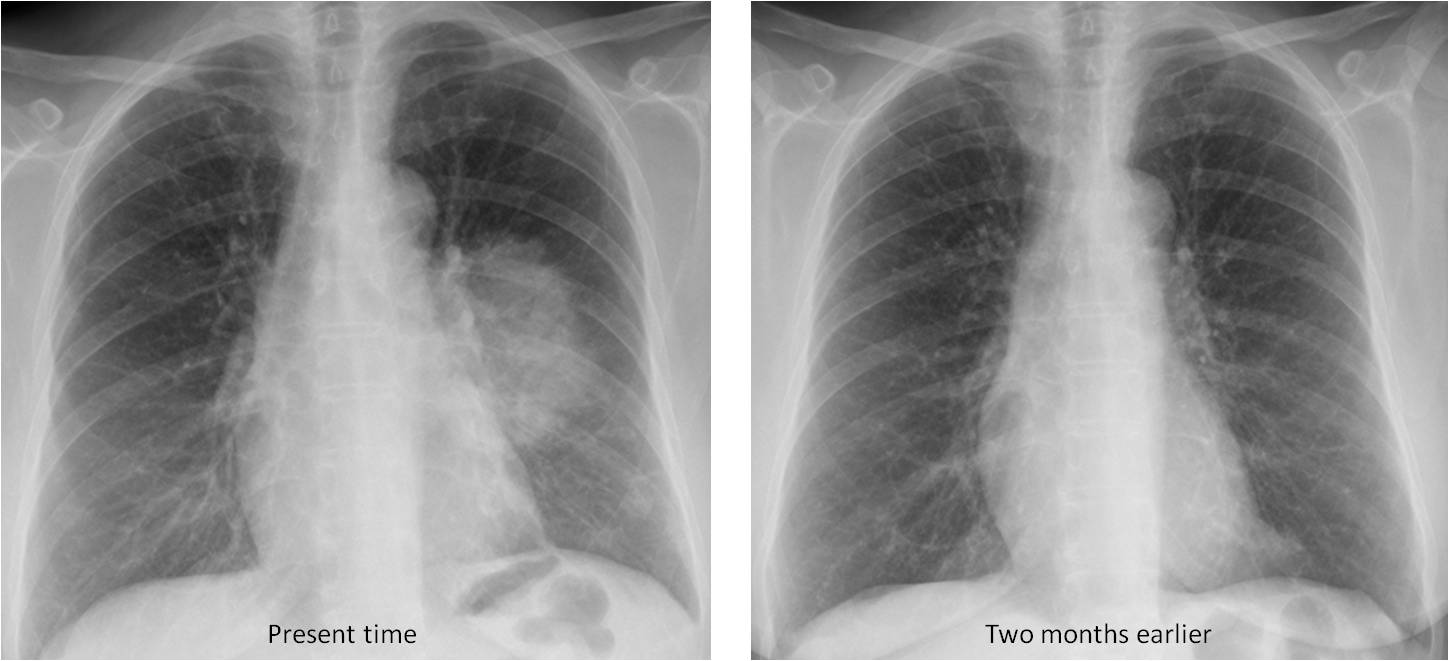
Fig. 7. 58-year-old woman with chest pain and moderate fever. Chest radiographs shows a rounded ill-defined opacity in the apical segment of the LLL (A and B, arrows). The appearance of the opacity raises the question of rounded pneumonia vs. carcinoma.
A previous radiograph taken two months earlier shows no abnormalities, excluding the diagnosis of carcinoma and confirming acute pneumonia, which healed after treatment.

Follow Dr. Pepe’s advice:
Most diagnostic errors are attributable to the radiologist.
Methodological errors are easily avoided if
– A lateral view is always taken and
– We make a habit of comparing with previous studies
“The answer is in the folder” (B. Felson)


In case 1, there is a widening of the right superior paratracheal line. I would like to check the lateral view, but if only I can choose one complementary study I prefer a CT.
In case 2 there is a loss of volume of the right hemithorax with a superior elevation of the hilum and hemidiaphragm. An atelectasia of the ULL? I can not say the cause of this with only a radiography.
Sorry to disagree with you. In my opinion, the paratracheal line is of normal width. What you see outside the line is the SVC. 😉
Case 1: Perhaps there is a narrowing of the main right bronchus with an elevation of the ipsilateral hemidiapgrham? Lateral view?
Taking a lateral view is always a wise decision.
RML atelectasi un case 1?
Sorry, URL nor ULL
Case 1: I see a pulmonar nodule at the right base. I would like a lateral view, too check if it’s or not a real nodule (nipples?).
Case 2: I see a lost of volume of the right hemithorax and a pseudonodular image/enlargment of the superior margin of the right hilum, it could be post-tbc changes, but a CT image or previous studies would be great
CT in another institution was reported as chronic TB changes. Would you believe it?
Both cases show reduced volume of right hemithirax, subtle mediastinal shift to right side, depressed right hilum, finding are suggestive of right lower lobe collapse in both cases.
In case 2: there is triangularity opacity in lateral view in posteroinferior corner which represent the collapsed right lower lobe
In case1: the lateral view is recommended next.
In the first case I think there is a round opacity on the right lung (middle to lower portion of lung) and firstly I would like to see a lateral view to confirm the existence of the finding and furthermore to assure that it is an intraparenchymal lesion.
In the second case I think there is volume loss of right lung, and hyperventiltion of the left lung. I can also see opacification of right apex, propably because of URL collapse (in my opinion also right hilum is a bit elevated).endobrochial mass cannot be excluded.
Hello,
I fully agree with Mahmoud in case 1 – round opacity in the middle zone of right lung – need lateral for further investigation of location of the lesion.
In case 2 I think there is lingula segment atelectasis with corresponding hiperinflation of left lung. Left hilar mass need to be excluded.
Case 1- tracheal narrowing just above bifurcation, tm? vascular anomaly? lymphadenopaty?.
Case 2- retrosternal opacification – segmental atelectasis of RUL?
case 1: it seems there’s an opacity superimposed on the right hilum, specifically on the ascending branch of the right pulmonary artery. A lateral view could be useful.
case 2: RUL volume loss. Comparison with previous films or CT to evaluate possible endobronchial lesion.
What about the CT report of chronic TB changes?
Case 1: RLL atelectasis. First check previous films. Need lateral view. If confirmed, chest CT to rule out/in obstructive atelectasis.
Case 2: RUL anterior segmental atelectasis expanding at the hilum in the lateral view. First check previous films, I think it is alway wise to do that to support the reading, but very suspicious for right hilar mass + obstructive atelectasis.
Muchas gracias Dr.
priceless information Dr.
thanks!