Dr. Pepe’s Diploma Casebook: Case 105 – To err is human: how to avoid slipping up (Chapter 4) – SOLVED!
Dear Friends,
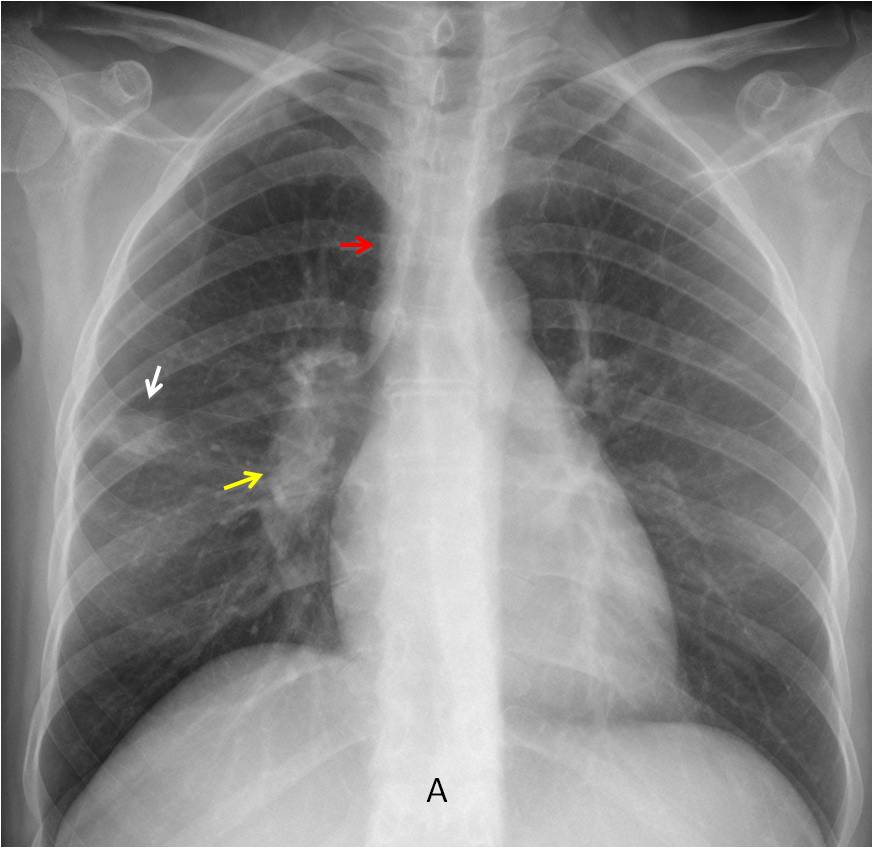
Continuining with the next chapter of “To err is human”, I present PA radiograph of a 45-year-old woman with chest pain and mild fever.
How many significant findings do you see?
1. One
2. Two
3. Three
4. Four
Check the image below, leave your thoughts in the comments section, and come back on Friday for the answer.

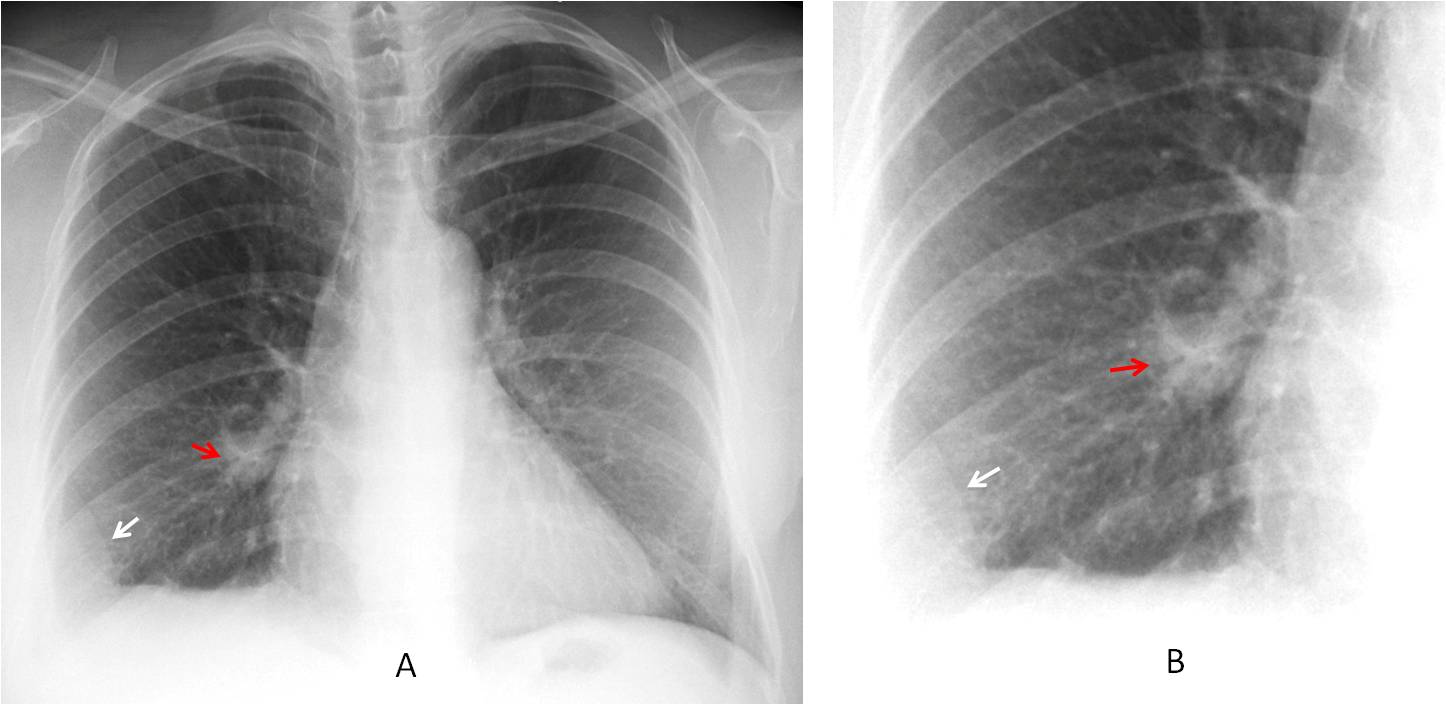
Findings: The answer is 3. The PA chest film shows a rounded opacity in the right lung (A, white arrow), and an increase in size and opacity of the right hilum (A, yellow arrow) compared to the left one. In addition, there is thickening of the paratracheal line (A, red arrow). These findings are highly suggestive of enlarged lymph nodes.
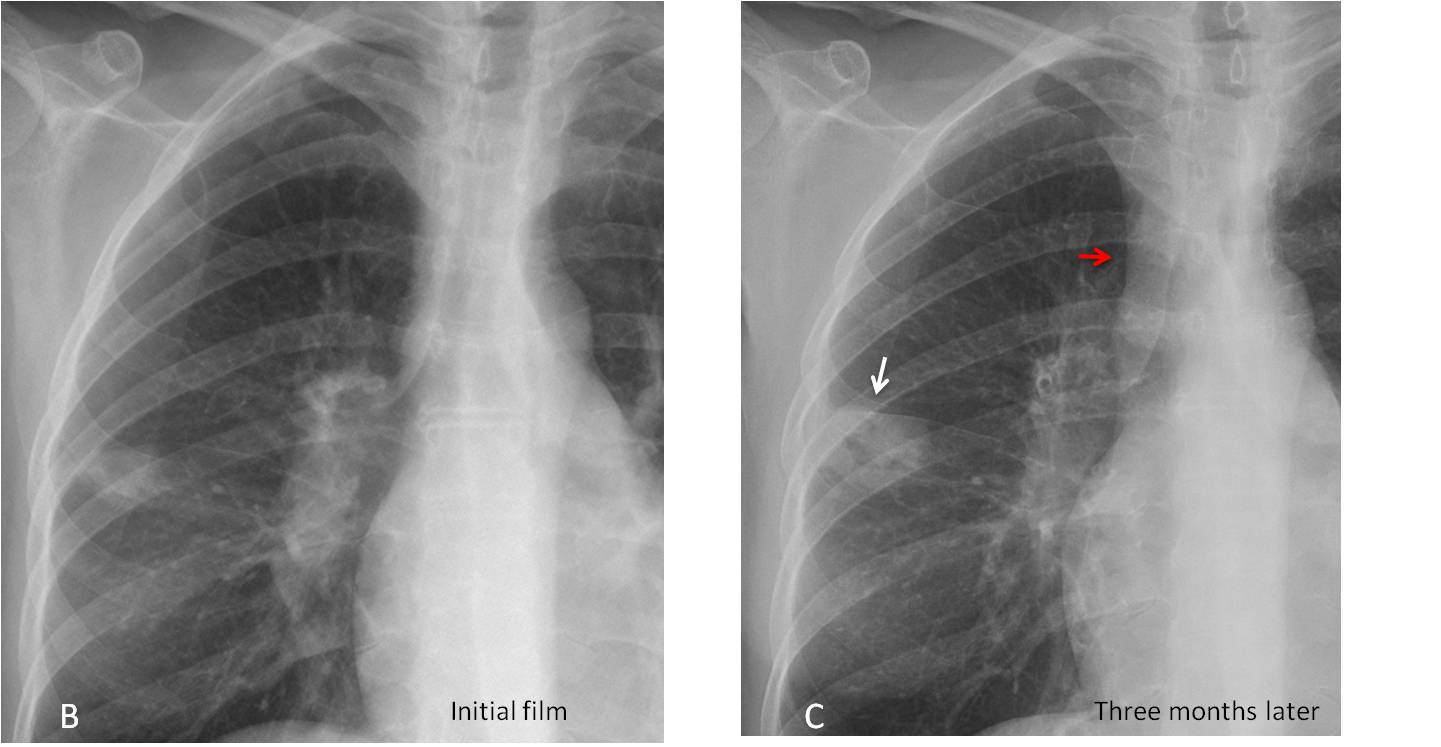
The enlarged nodes were overlooked and the patient was diagnosed with an infectious process. Three months later, the peripheral mass had enlarged and cavitated (C, white arrow) and the paratracheal line had thickened further (C, red arrow).
Enhanced axial and coronal CT show a thick-walled peripheral cavity (D and E, white arrows) and numerous hilar and mediastinal lymph nodes (D and E, red arrows).
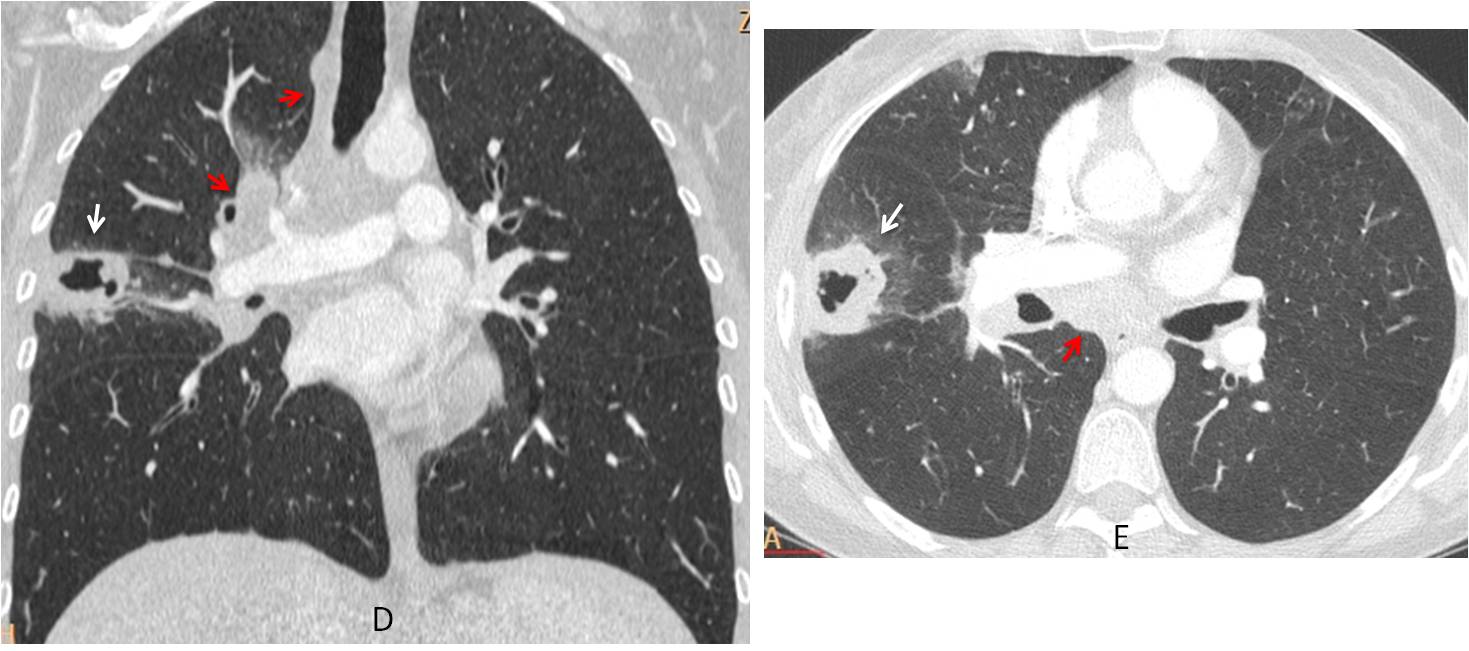
Final diagnosis: carcinoma of the lung with metastases to the mediastinum
The purpose of this presentation is to discuss another cause of perception errors:
satisfaction of search (SOS). In this type of error, findings are missed because we don’t search for additional abnormalities after the first one is found. When there are multiple findings, additional ones are discovered less than 50% of the time.
SOS accounts for about 22% of all errors and can be prevented by using checklists. As I have spoken extensively about checklists in previous chapters, I won’t insist on deploying them again here. Instead, to emphasise the importance of SOS, I will show four cases previously published in the blog in which SOS significantly contributed to the viewers’ answers.
Case 1 was presented in Cáceres’ Corner on May 29, 2013. Radiographs belong to a 57-year-old woman with chronic cough and mild fever. Diagnostic options were:
1. Bronchogenic spread of TB
2. Hypersensitivity pneumonitis
3. Sarcoidosis
4. None of the above
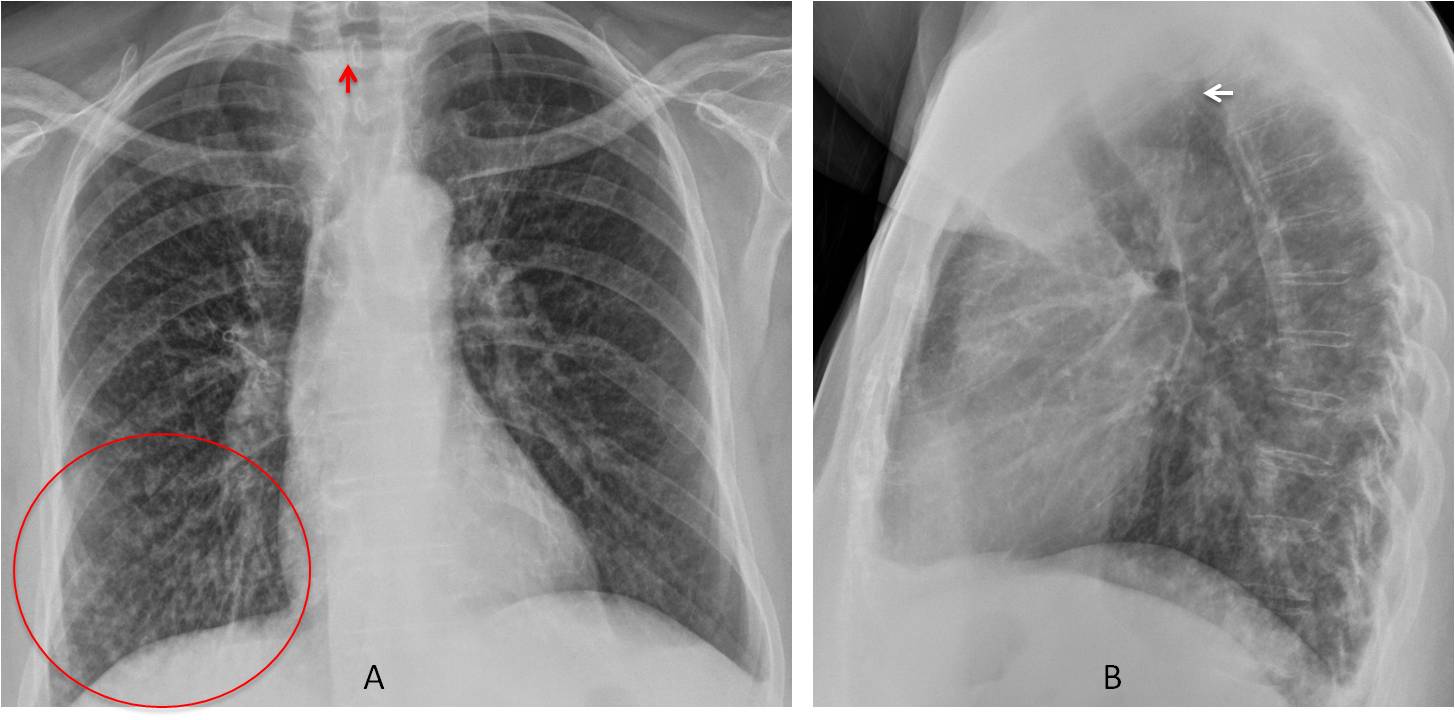
PA chest shows a small diffuse nodular infiltrate that is more evident in the right lung, especially in the RLL (A, circle). An air-fluid level is visible in the upper mediastinum (A, arrow). The lateral view shows anterior displacement of the trachea (B, arrow) by a retrotracheal mass in the Raider triangle. The findings are highly suggestive of pulmonary aspiration secondary to a dilated upper esophagus or a Zenker diverticulum.
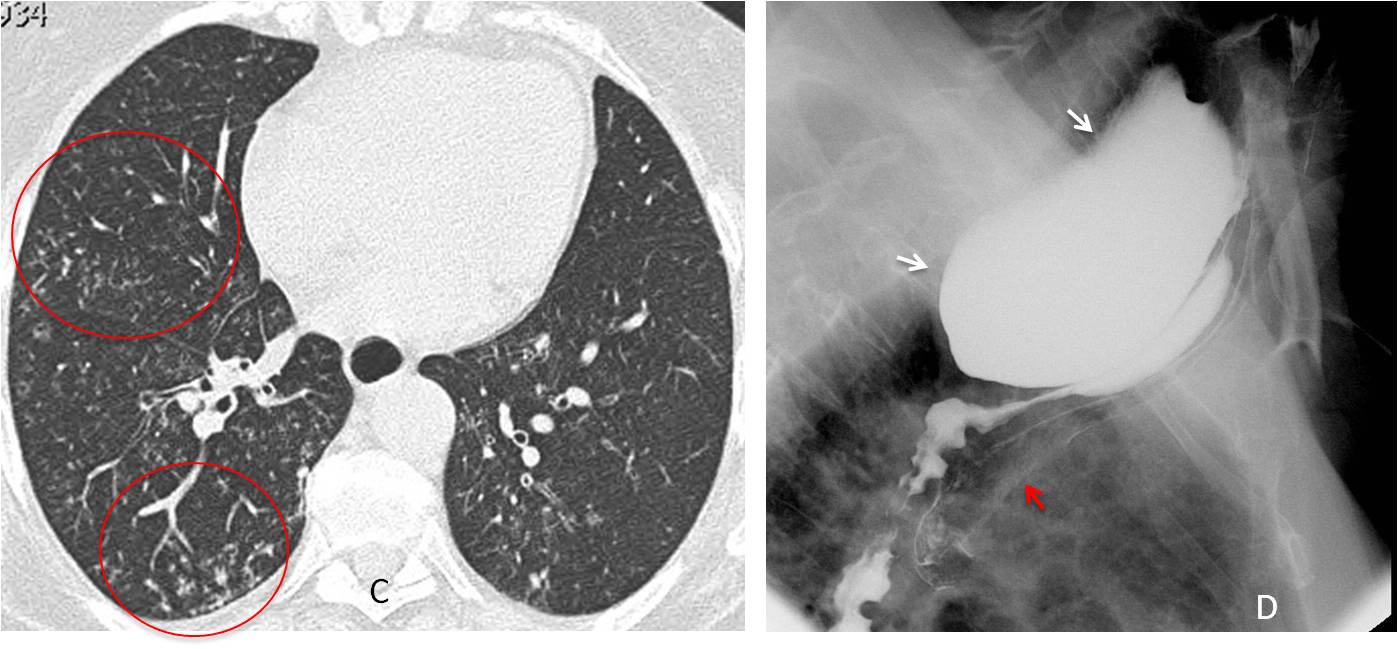
Axial CT shows non-descript nodular lung infiltrates (C, circles). Esophagogram depicts a large Zenker’s diverticulum (D, white arrows), with aspirated barium in the trachea (D, red arrow).
There were 25 answers to Case 1. The most common was scleroderma with pulmonary changes (8 answers). The responders failed to detect a negative finding: lack of dilatation of the whole esophagus, which practically excludes scleroderma. Only 5 of them mentioned Zenker diverticulum. TB was diagnosed 5 times.
Overall, about 50% of the responders failed to mention the air-fluid level, a crucial finding to suggest aspiration as the cause of the pulmonary changes.
Case 2 was presented in Cáceres’ Corner on July 16, 2012. Radiographs belong to a 38-year-old man who came to the emergency room with moderate chest pain. Diagnostic options were:
1. Pleural metastasis
2. Neurogenic tumour
3. Fibrous tumour of pleura
4. Any of the above
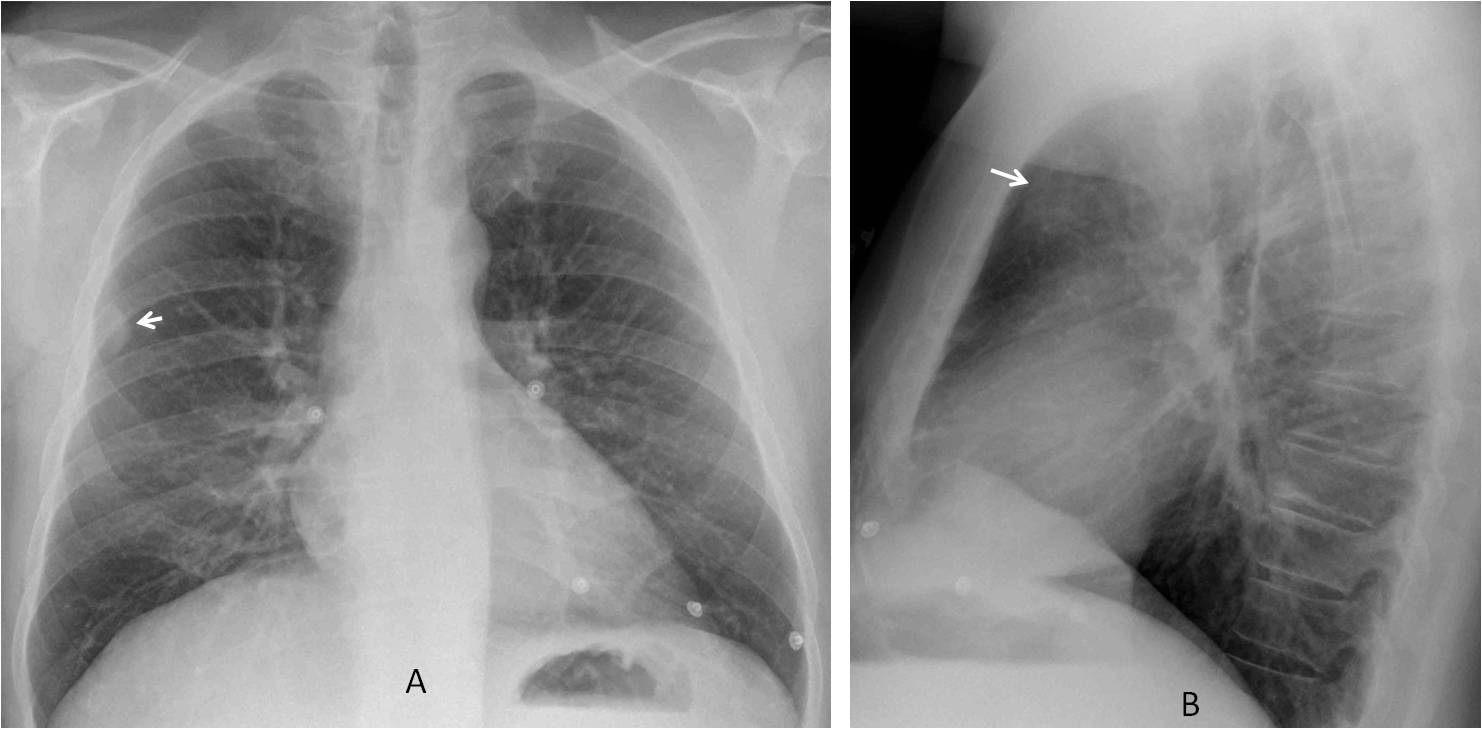
The PA chest film shows a peripheral extrapulmonary nodule (A, arrow). The lateral film depicts a rounded opacity in the anterior clear space (B, arrow).
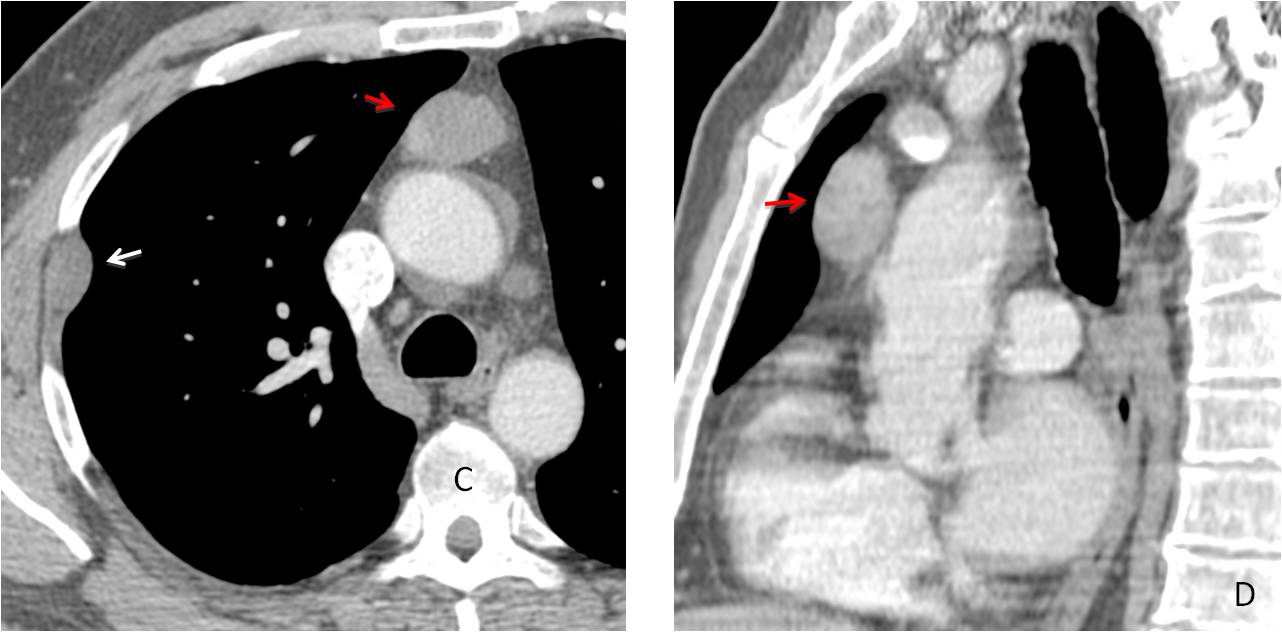
Enhanced CT confirms an extrapulmonary nodule (C, white arrow), as well as a rounded anterior mediastinal mass (C and D, red arrows). This combination suggests a malignant thymoma with pleural metastasis, as thymomas metastasize along the pleural layers. However, a thymoma with a coincidental chest wall mass could not be excluded. Therefore, the correct answer should be 4. Any of the above
The patient underwent surgery, and the final diagnosis was benign thymoma and chest wall schwannoma.
Case 2 had 14 answers. Six responders diagnosed neurogenic tumour. The remaining 8 (62%) did not mention the anterior mediastinal mass visible in the lateral view.
Case 3 was presented in Cáceres’ Corner on February 23, 2015. The radiographs belong to a 57-year-old woman with acute chest pain and mild fever. Diagnostic options were:
1. Pneumonia
2. Pulmonary infarct
3. Pleural fluid
4. None of the above
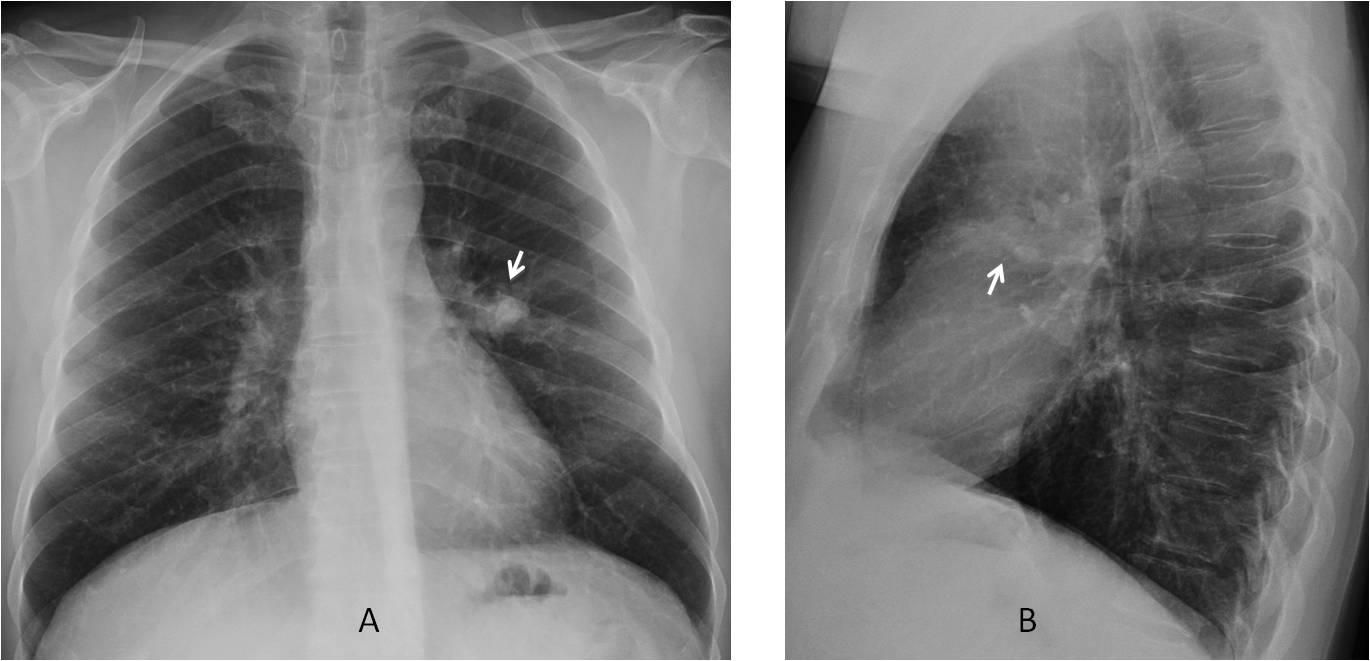
PA radiograph shows a triangular pulmonary opacity at the right costophrenic angle (A and B, white arrows), with the characteristic appearance of a Hampton hump, suggesting a pulmonary infarct. In addition, a rounded nodule is visible in the lower area of the right hilum (A and B, red arrows).
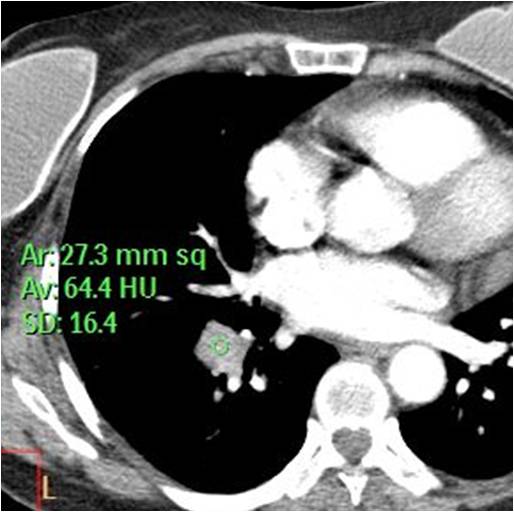
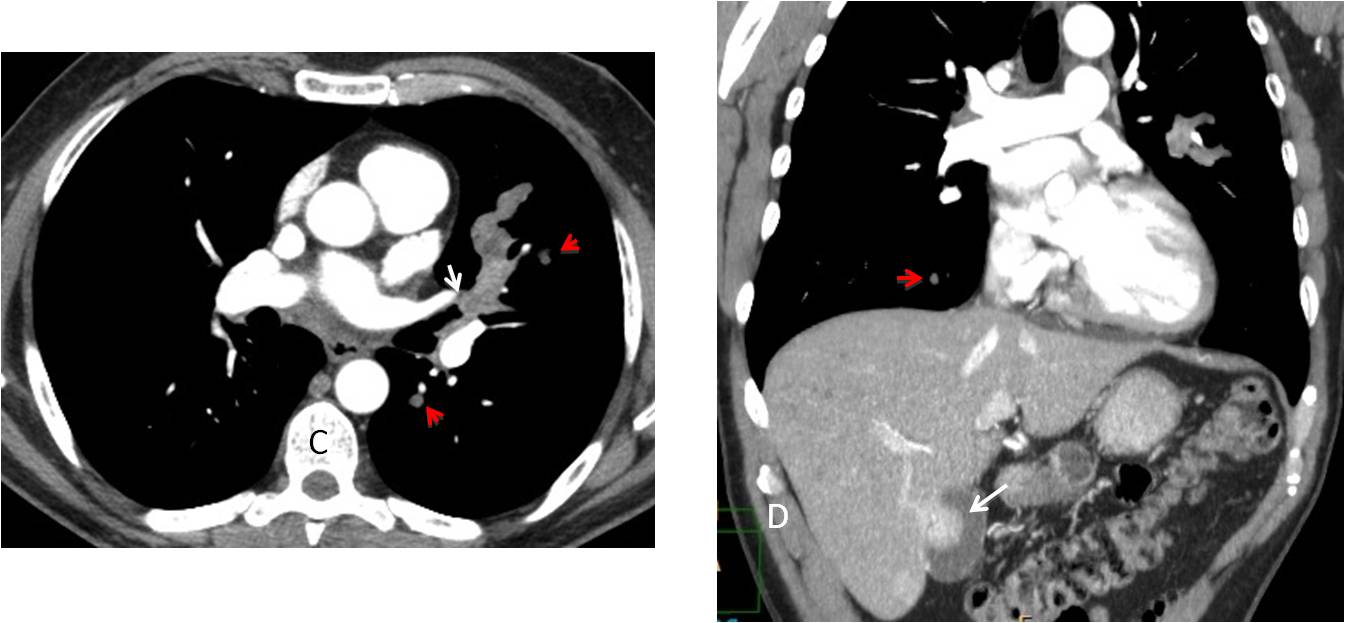
CT confirmed the pulmonary embolism and a RLL mass (C, red arrow) that enhanced to 42 H.U. after contrast injection, suggesting malignancy (D, red arrow). The final diagnosis was carcinoma of the lung with pulmonary infarct.
Case 3 elicited 10 answers. Five of them diagnosed pulmonary infarct. Nine of them (90%) missed the nodule in the lower part of the right hilum. Only one responder mentioned the nodule and considered the possibility of cancer with associated pulmonary infarct.
Case 4 was presented in Cáceres’ Corner on May 23, 2012. Radiographs belong to a 51-year-old male smoker with moderate cough, no fever. Chest radiographs and enhanced axial and coronal CT were shown. Diagnostic options were:
1. Metastases
2. Carcinoma of the lung
3. Allergic aspergillosis
4. None of the above
The PA chest film shows an opacity in the left mid-lung field (A, arrow). Its shape in the lateral view suggests mucus impaction (B, arrow).
Enhanced axial CT shows an endobronchial lesion (C, white arrow) with distal bronchial impaction, as well as two small lung nodules (C, red arrows). Coronal CT shows another small nodule (D, red arrow) as well as an enhancing nodule inside the gallbladder (D, white arrow).
The combination of an endobronchial lesion, pulmonary nodules and a gallbladder mass suggests widespread metastases, with a high probability of melanoma as the primary lesion. Bronchoscopy confirmed a melanotic lesion in the bronchus. Final diagnosis: widespread metastases from melanoma.
There were 23 answers to case 4. The most common one was allergic aspergillosis (15 answers). Only 3 responders saw the lung nodules and mentioned the diagnosis of widespread malignancy. Altogether, 20 responders (86%) failed to detect the lung and gallbladder nodules.

Follow Dr. Pepe’s advice:
1. When one abnormality is found, around 50% of additional findings are missed.
2. Satisfaction of search accounts for approximately 22% of errors.
3. Satisfaction of search can be avoided by using checklists.


Good morning!!!
I think that there are 2 abnormal findings: the right hilum is increased in size and density, with a nodular appearence. Also I see a horizontal increased density area proyected over the RUL (the first idea is a mucus plug).
Perhaps 3, if we count the low diffuse density of the right hemithorax
Hello.
I see a nodule on the right lung, the right hilum is enlarged, there is an irregularity in the upper portion of the left hilum, associated with a small linear and vertical opacity. And I also think there is a very small lung nodule just above the left hilum.
Four findings, then.
Hi,
1- enlargement of the right pulmonary artery (Fleishner sign).
2- oligaemia in the right mid and lower zones compared with the left (Westermark sign).
3- faint wedge- shaped opacity over the right mid zone (Hampton sign).
4- abrupt cutoff of the pulmonary artery branches over the right mid zone (knuckle sign).
my suggestion is right pulmonary artery embolism.
Thanks
Hi
i thimk there is only one abnormality which is enlargment of the right hilum.
4:
1) widened paratracheal line,
2) enlarged right hilum,
3) opacity projected over the anterior part of IVth rib
4) linear opacity near the pulmonary trunk
1.enlarged right hilum with nodular opacities and few nodular bopacities in left hilum as well? lymphnodes
2. Few opacities in right mid /lower zones ?linear opacity in right mid zones. these may represent mucous impacted bronchi/ infective nodules.
3. haziness in bilateral lower zones left>right
4. thickeng of minor fissure
Hi!
Prominent rignt hilum could be consistent with right pulm.a. embolism, and opacity in the perifery of the middle zone infarction, anamnestic sign is mild fever, maybe septic emboli?
Also could be pneumonic infiltration with hilar adenopathy, but the case should be complex, so..
I can also see faint soft tissue shadow in the left upper zone near the aortic knuckle between posterior parts of the 5th and 6th rib
….gentilissimo Prof…..ci sono due segni evidenti….iperplasia ilo dx ed opacità ground-glass in campo medio omolaterale…..vi è poi un terzo segno,….l’ispessimento della linea paratracheale e mediastinica, bilateralmente, che potrebbe essere di natura adenopatica….il quarto segno potrebbe essere l’immagine aerea, ipertasparente nell’ambito dell’ilo dx iperplastico(broncocele?)…..in caro saluto ….
…grazie Prof…..possiamo dire che il Bari è andato vicino al goal ?
Dear friends, the aim of this case was to explore satisfaction of search. Of all the responders only two (ania and genchi bari) mentioned the enlarged paratracheal line, which reinforced the presence of adenopathy and the likely diagnosis of malignancy.
Dear my question
Why this case pospond for 3 months later
This case was initially diagnosed as infection and treated as such. The next radiograph was taken two months later as well as the CT. I chose the radiograph at three months because the changes were more obvious. Still, a two month delay is significant. Perhaps the patients’ symptoms improved or she missed an appointment with his doctor
Thanks professor. indeed an eyeopener. I have a doubt. How do we differenciate thickened paratracheal stripe from the shadow of SVC, on occasions i have reported it as thickened paratracheal stripe and others have refuted terming it as simply vascular shadow.
This a difficult question. Will write to your mail with one image of each, giving you my approach