Dr. Pepe’s Diploma Casebook: Case 106 – To err is human: how to avoid slipping up (Chapter 5) – SOLVED!
Dear Friends,
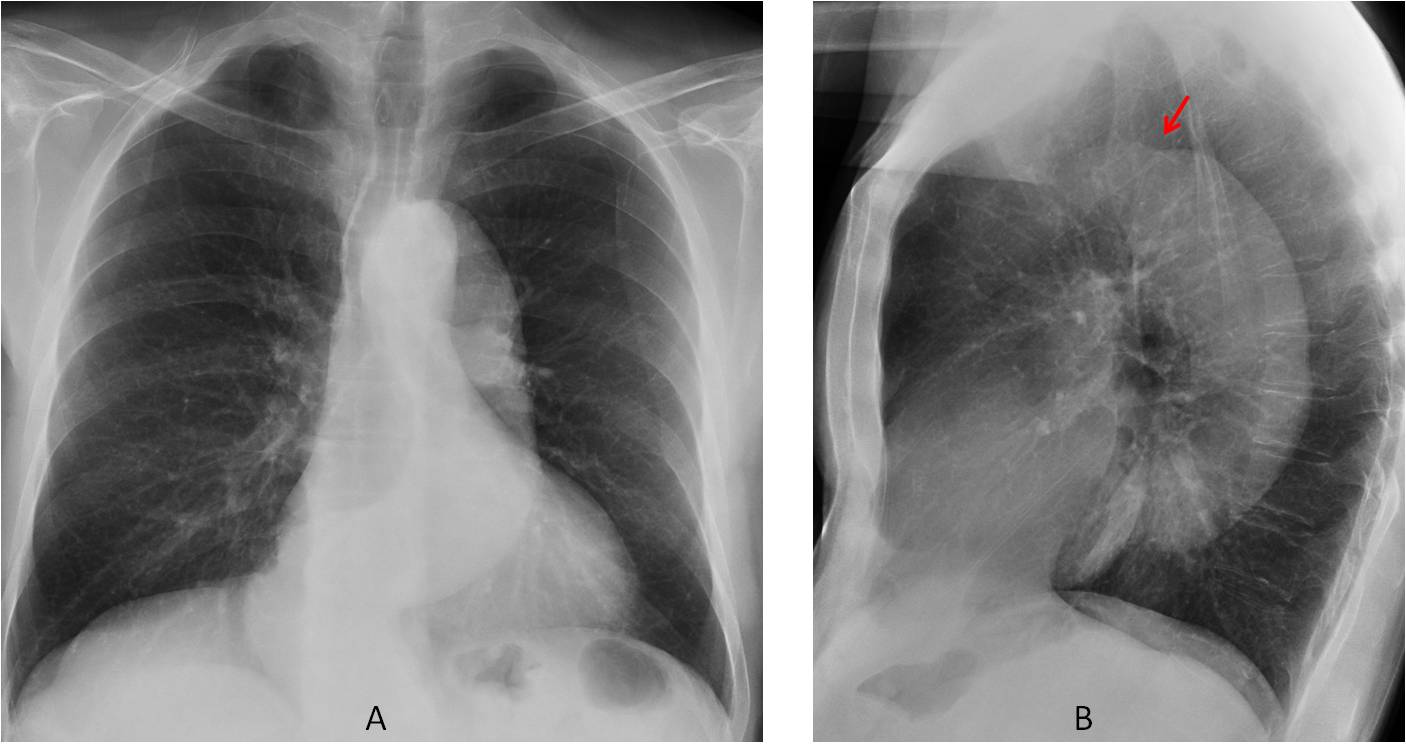
This week I’m continuing with another chapter of “To err is human”; and today I am presenting chest radiographs of a 64-year-old man. These images were taken one month after a myocardial infarction.
Check the images carefully, leave your thoughts in the comments and come back on Friday for the answer.
Diagnosis:
1. Aortic elongation
2. Aortic dissection
3. Aortic aneurysm
4. Any of the above


Findings: Chest radiographs show an elongated descending aorta, while the ascending aorta is not prominent at all, as evidenced in both views. A non-dilated ascending aorta goes against aortic elongation (the whole aorta should be prominent). In my experience, the combination of a non-dilated ascending aorta and dilated descending aorta is highly suggestive of type B dissection. The transition from normal to dilated aorta can be seen in the lateral view (B, red arrow).
Enhanced CT confirms the diagnosis of type B dissection (C and D, arrows). The dissection was discovered incidentally in a cardiac MRI performed to evaluate the heart after the myocardial infarction (insert, arrow).
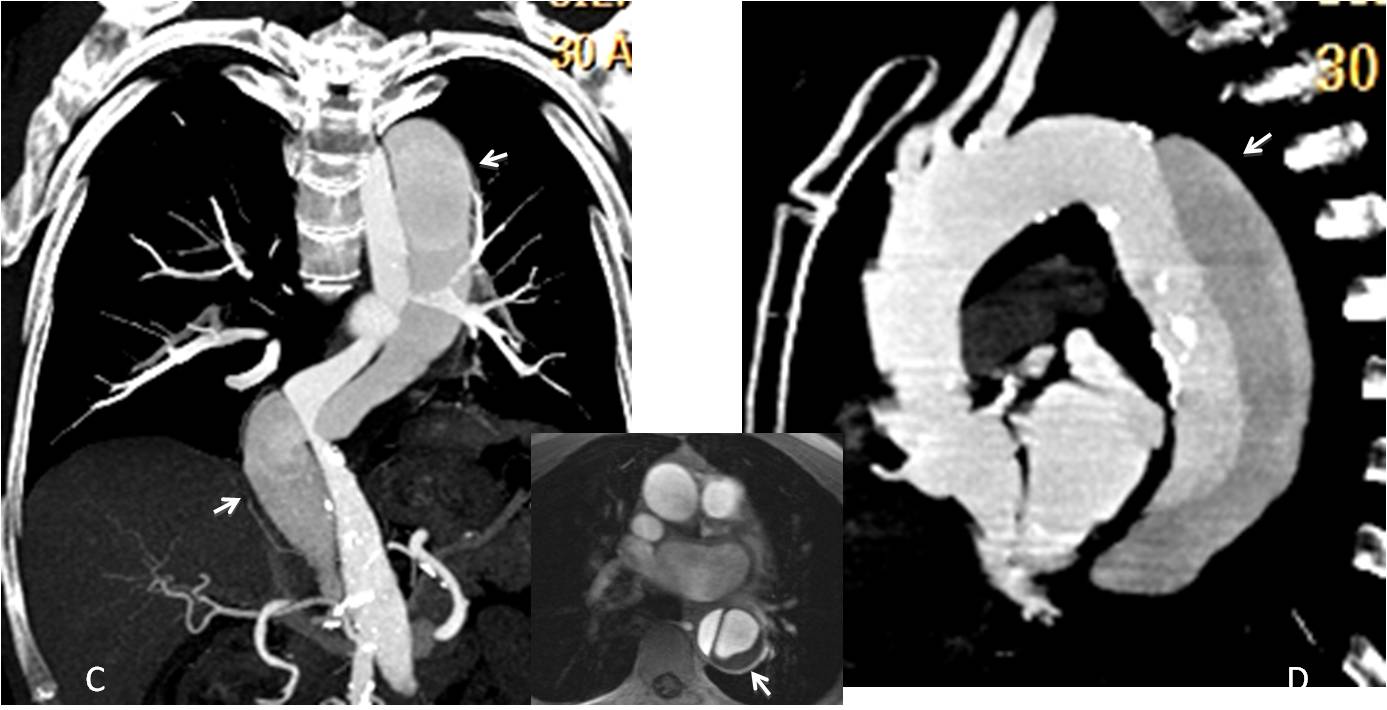
Final diagnosis: asymptomatic type B aortic dissection.
Up to now, I have shown several types of perceptual errors in which abnormalities are missed. In this presentation I plan to discuss cognitive (interpretive) errors. They occur when an abnormality is identified, but is incorrectly interpreted, resulting in a misdiagnosis.
Interpretive errors account for about 12% of all errors. They have three main causes:
– Over-reading
– Faulty reasoning
– Lack of knowledge
Over-reading occurs when an unimportant finding is attributed to a more serious cause. It accounts for about 1% of errors. Over-reading can be prevented by knowing, among other things, the most common normal variants (Figs. 1 and 2).
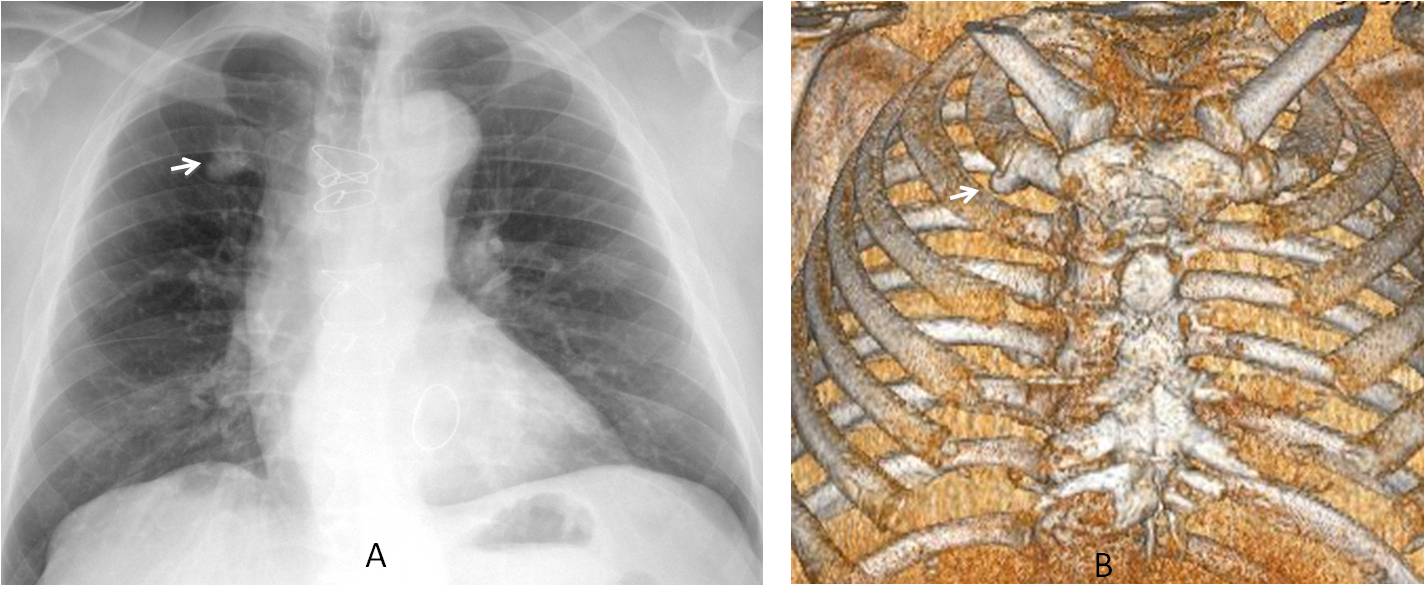
Fig. 1
Over-reading occurs when an unimportant finding is attributed to a more serious cause. It accounts for about 1% of errors. Over-reading can be prevented by knowing, among other things, the most common normal variants (Figs. 1 and 2).
Fig. 1: 56-year-old man who came to the ER with chest pain. A RUL nodule was diagnosed (A, arrow). CT shows that the nodule corresponds to calcified cartilage of the first rib (B, arrow).
This clear case of over-reading could have been prevented by being aware of the variant and, in case of doubt, by comparing with the previous film (D, below), which showed identical findings (C and D, arrows). Unnecessary CT could have been avoided.
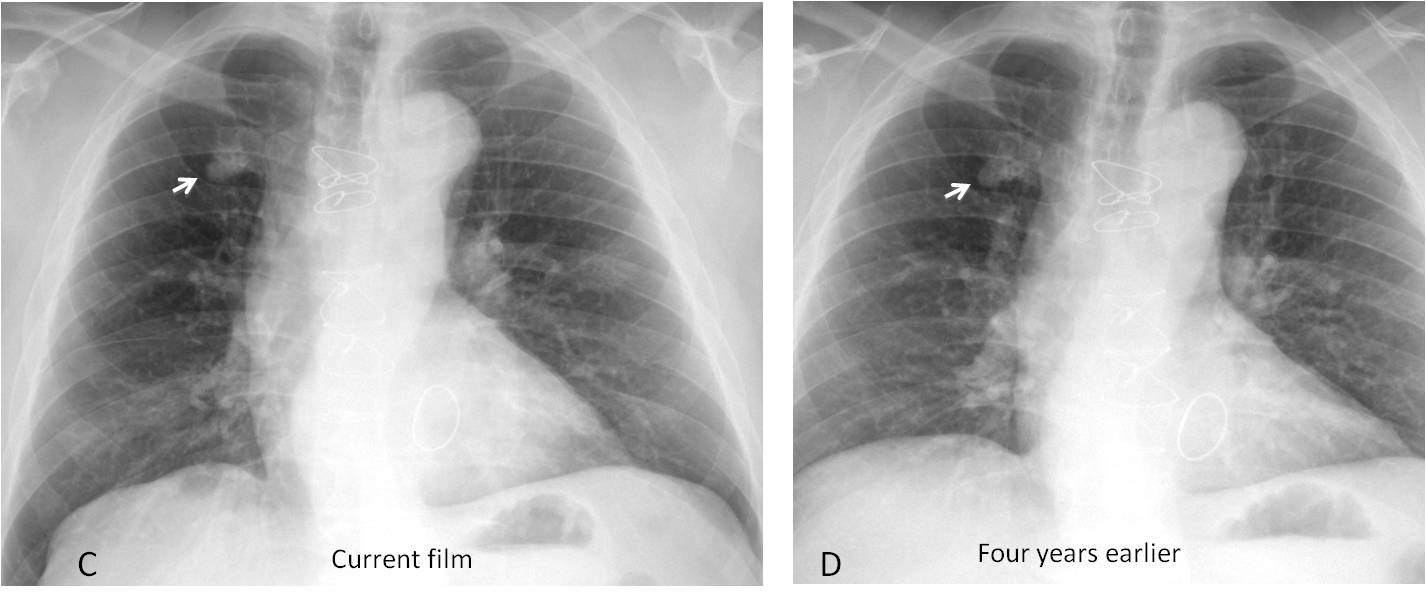
Fig. 1
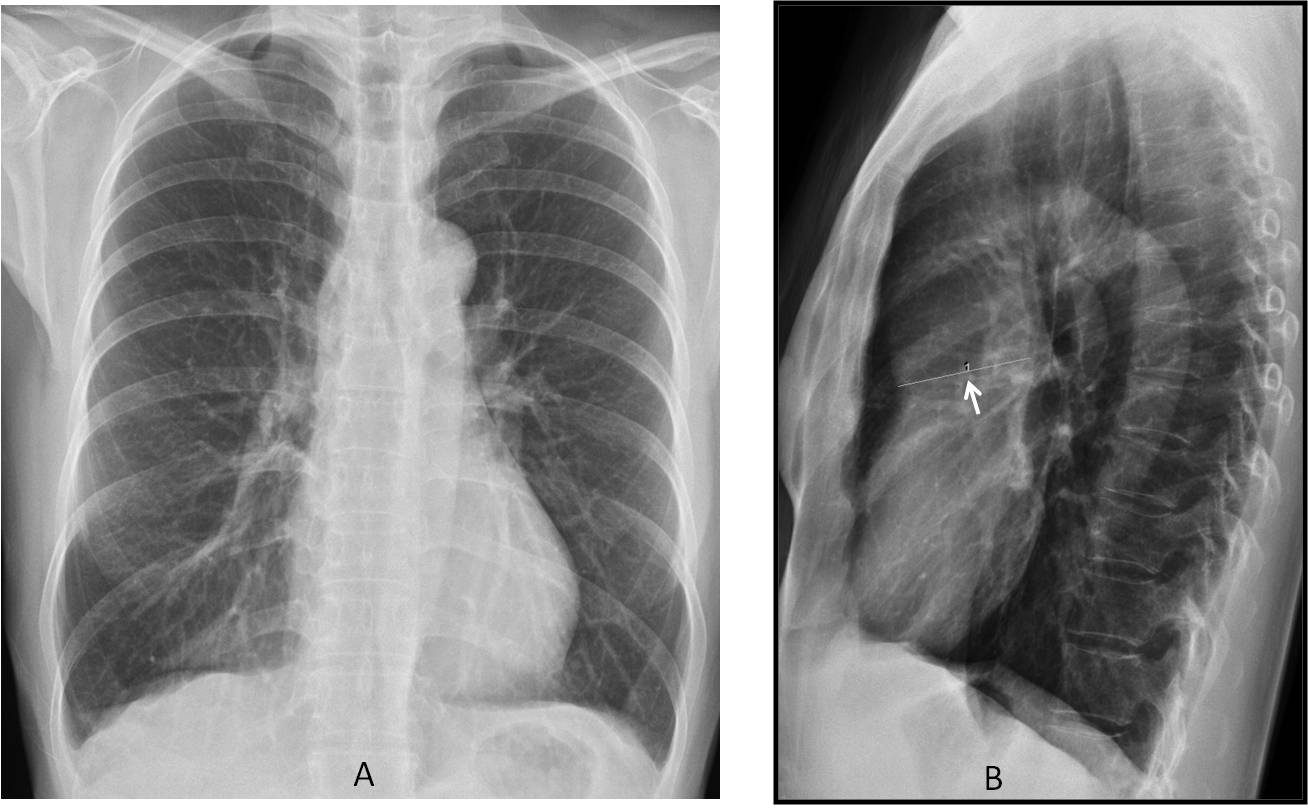
Fig. 2
Fig. 2: this asymptomatic 35-year-old woman was diagnosed with dilatation of the ascending aorta (B, arrow), and aortic dissection was suspected. MRI (not available) showed a normal aorta. An over-reading error had occurred: the measurement in the lateral view is erroneous because the posterior wall of the ascending aorta is not outlined by lung air and therefore, cannot be seen. Whoever traced the line was wrong. The apparent enlargement of the ascending aorta is due to the narrow A-P diameter of the chest.
In faulty reasoning, the finding is seen and considered abnormal, but it is attributed to the wrong cause. Faulty reasoning is the most common interpretive error, accounting for around 9% of all errors. It can be prevented by considering a list of differential diagnoses (Figs. 3 and 4).
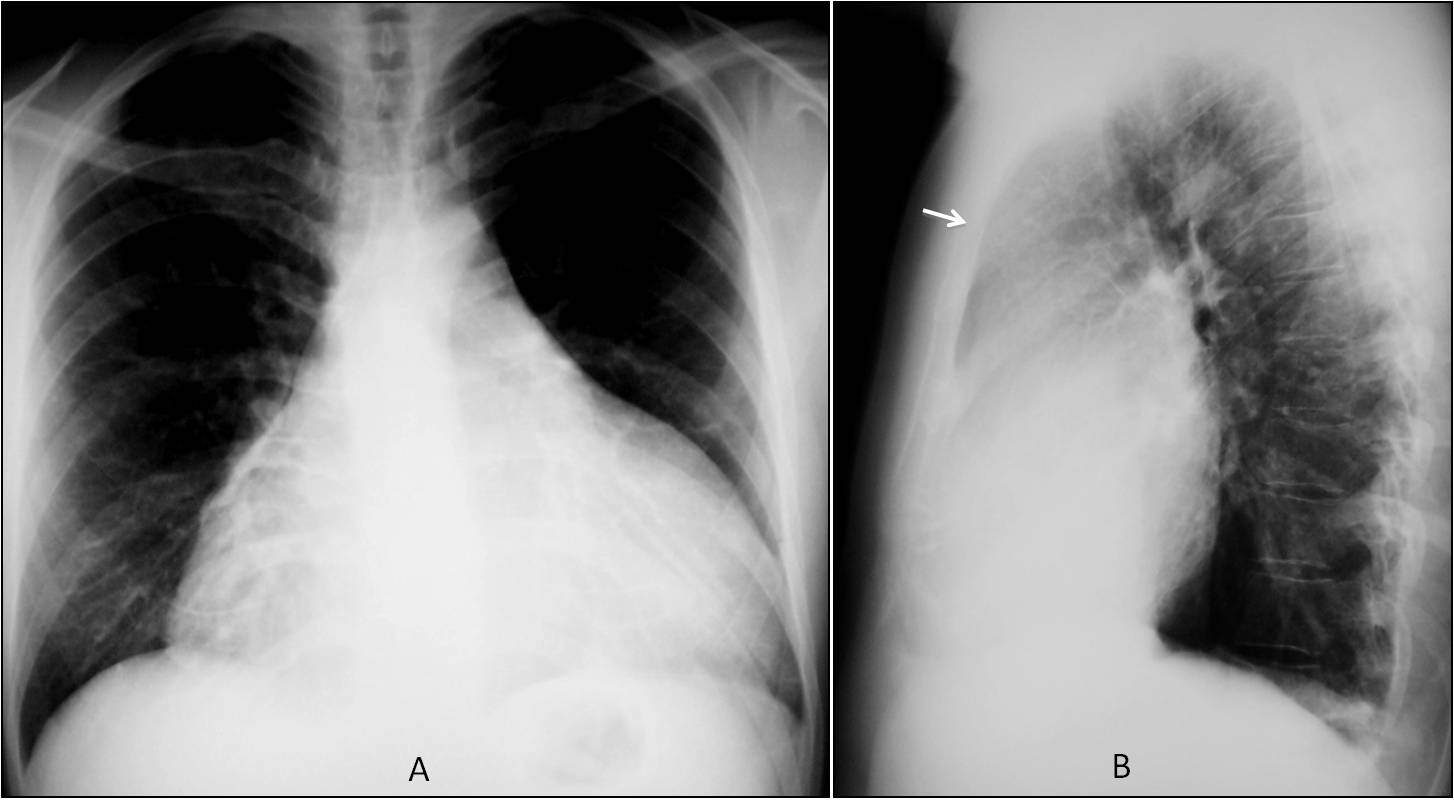
Fig. 3
Fig. 3: 29-year-old man diagnosed with pericarditis based on the large cardiac silhouette and low vascularisation of the lungs. The radiologist failed to see the occupation of the anterior space in the lateral view (B, arrow) and the lack of posterior displacement of the cardiac shadow. These findings are suggestive of a mediastinal mass, and this, together with dilated cardiomyopathy and pericarditis are the main differential diagnoses of enlarged cardiac shadow.
Enhanced axial CT (below) shows a large, fatty, anterior mediastinal mass wrapped around the heart and mediastinal structures (C and D, arrows). Final diagnosis: thymolipoma.
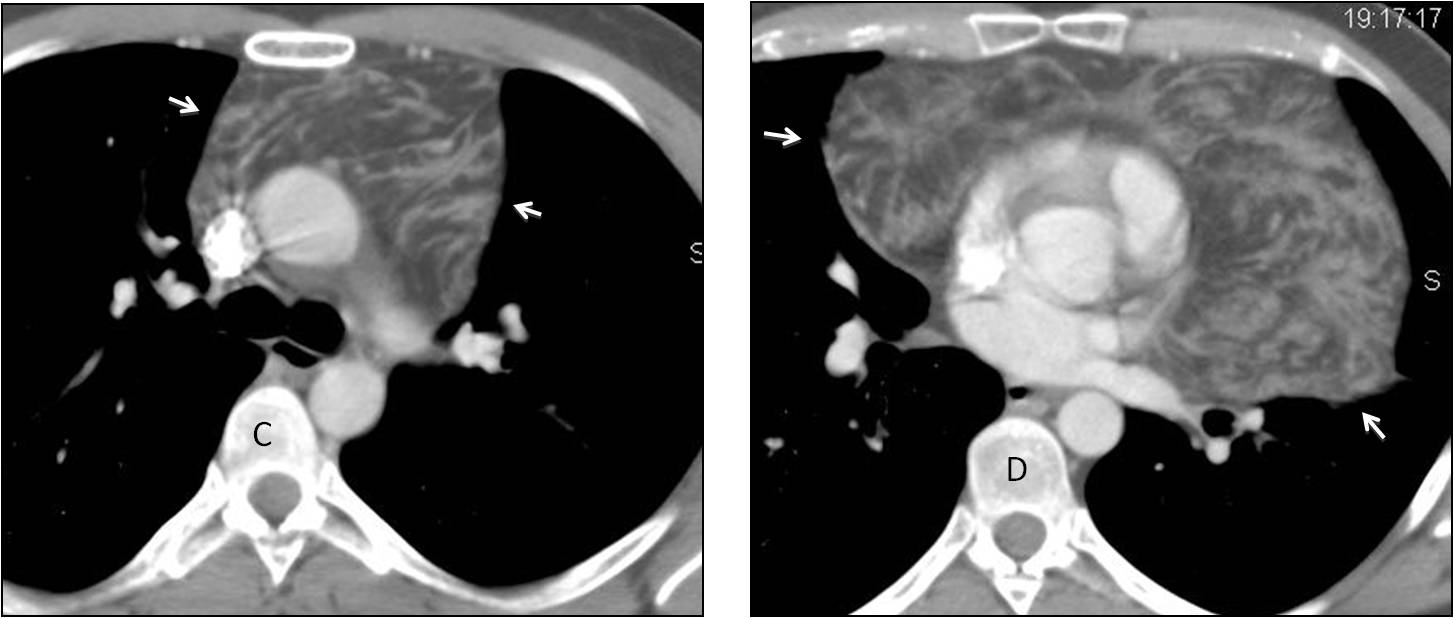
Fig. 3
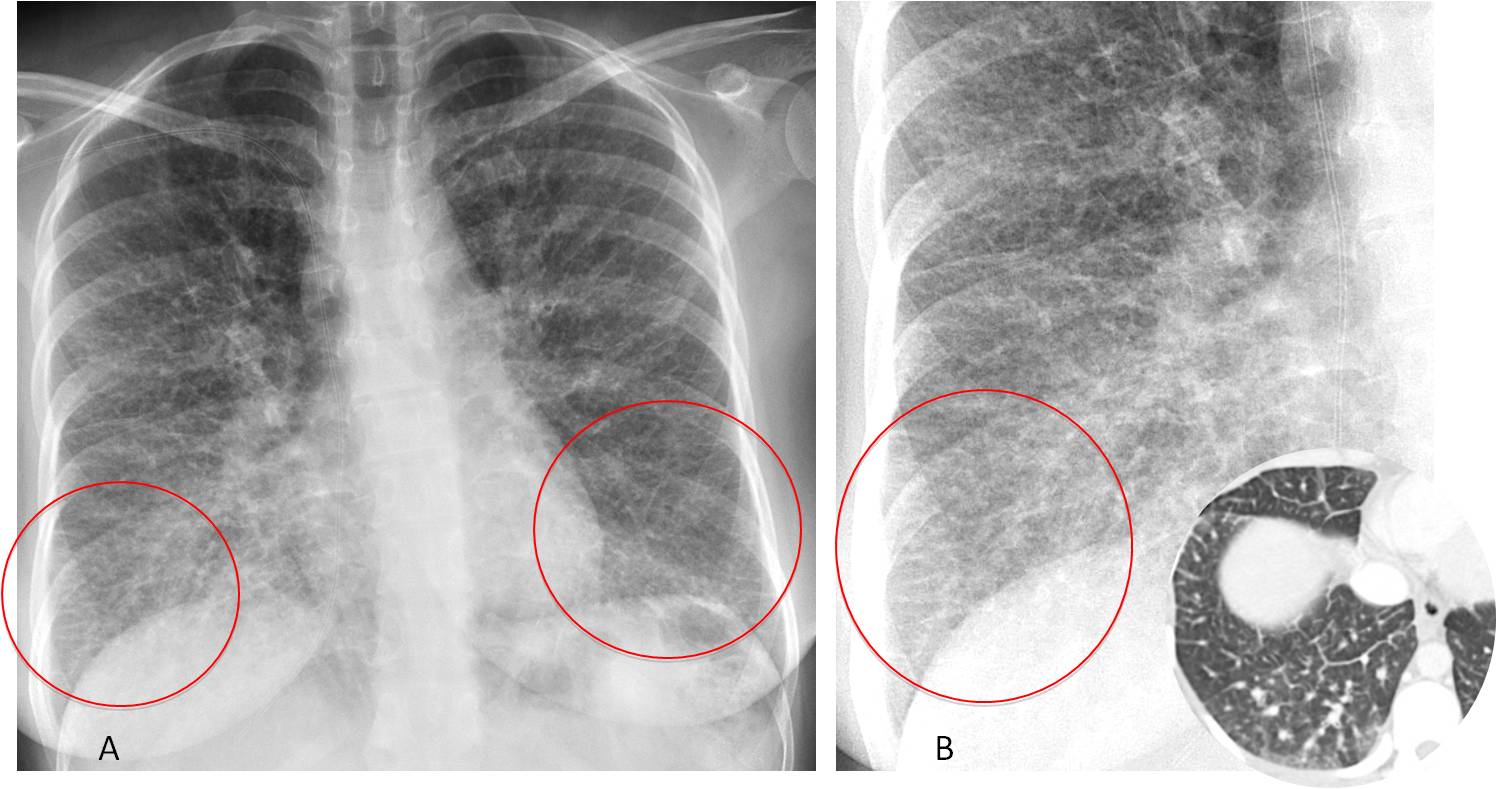
Fig. 4
Fig 4: 34-year-old hairdresser with gastric carcinoma. Preoperative PA chest film shows multiple Kerley lines in both lungs (A and B, circles), confirmed on CT (insert). This case was presented at the blog and the answers were divided between extrinsic alveolitis and lymphangitic carcinomatosis. In my experience, when you see multiple Kerley lines, lymphangitic spread of carcinoma is by far the best option. Diagnosis confirmed by biopsy.
Lack of knowledge accounts for about 3% of interpretive errors. In these cases the finding is detected, but its diagnostic importance is missed because of the reader’s lack of expertise. To decrease these errors, radiologists must actively update their knowledge through the literature and continuing medical education.
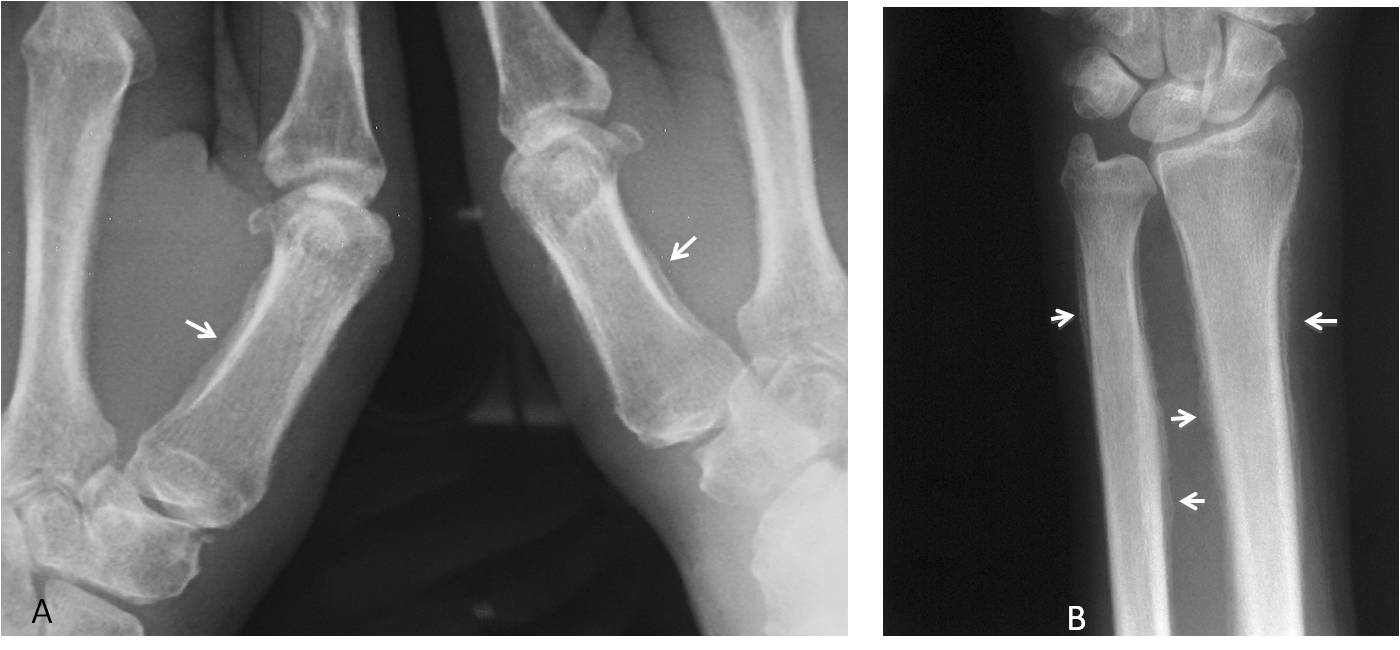
Fig. 5
Fig 5: cone down radiographs of both hands and the left wrist of a 59-year-old man with hand pain. There is periostitis in the first metacarpals (A, arrows) and extensive periostitis in the bones of the forearm (B, arrows). This case was shown in the blog. Thyroid acropachy psoriasis, and hyperparathyroidism were mentioned. Most responders forgot to mention hypertrophic pulmonary osteoarthropathy, which should be considered in an adult.
Chest radiography showed a nodular opacity in the right lung, confirmed with CT (C and D, arrows). Diagnosis: carcinoma of the lung with hypertrophic osteoarthropathy.
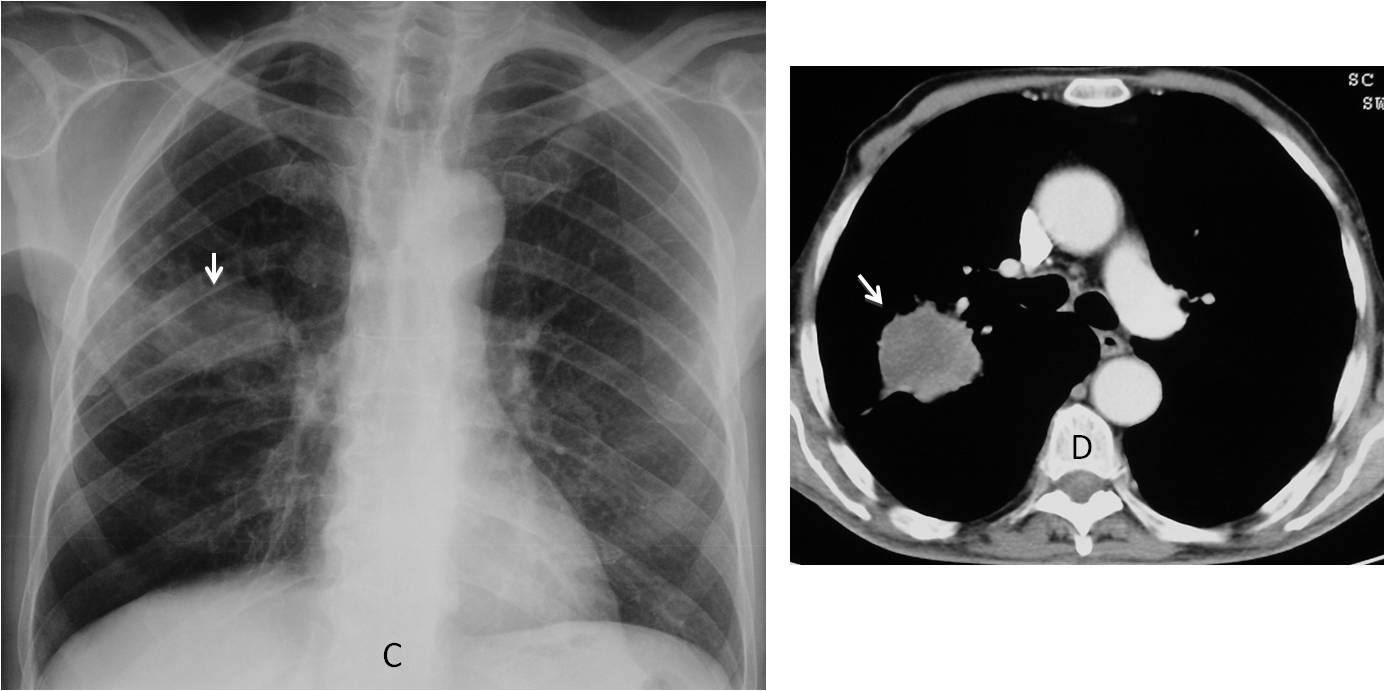
Fig. 5
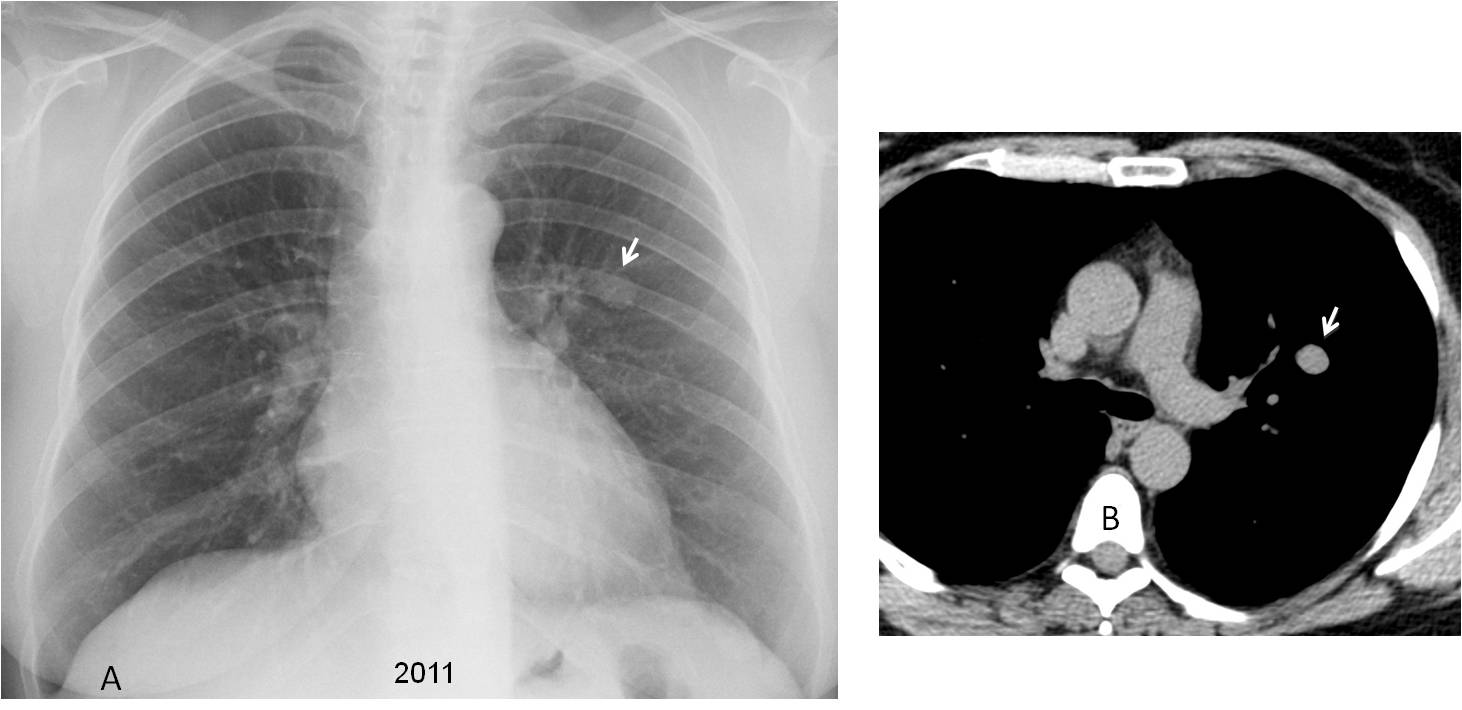
Fig. 6
Fig. 6. Preoperative chest radiograph in a 42-year-old woman. A nodule was discovered and a CT taken (A and B, arrows). Surprisingly, the CT was read as “16 mm benign nodule consistent with granuloma”. In this case we can change the phrase lack of knowledge to plain ignorance, because the nodule has an indeterminate appearance, and there is no reason at all to call it a granuloma.
A second chest radiograph five years later shows discrete enlargement of the nodule (C and D, arrows), confirmed with unenhanced CT (E and F, arrows). Surgical diagnosis: hamartoma.
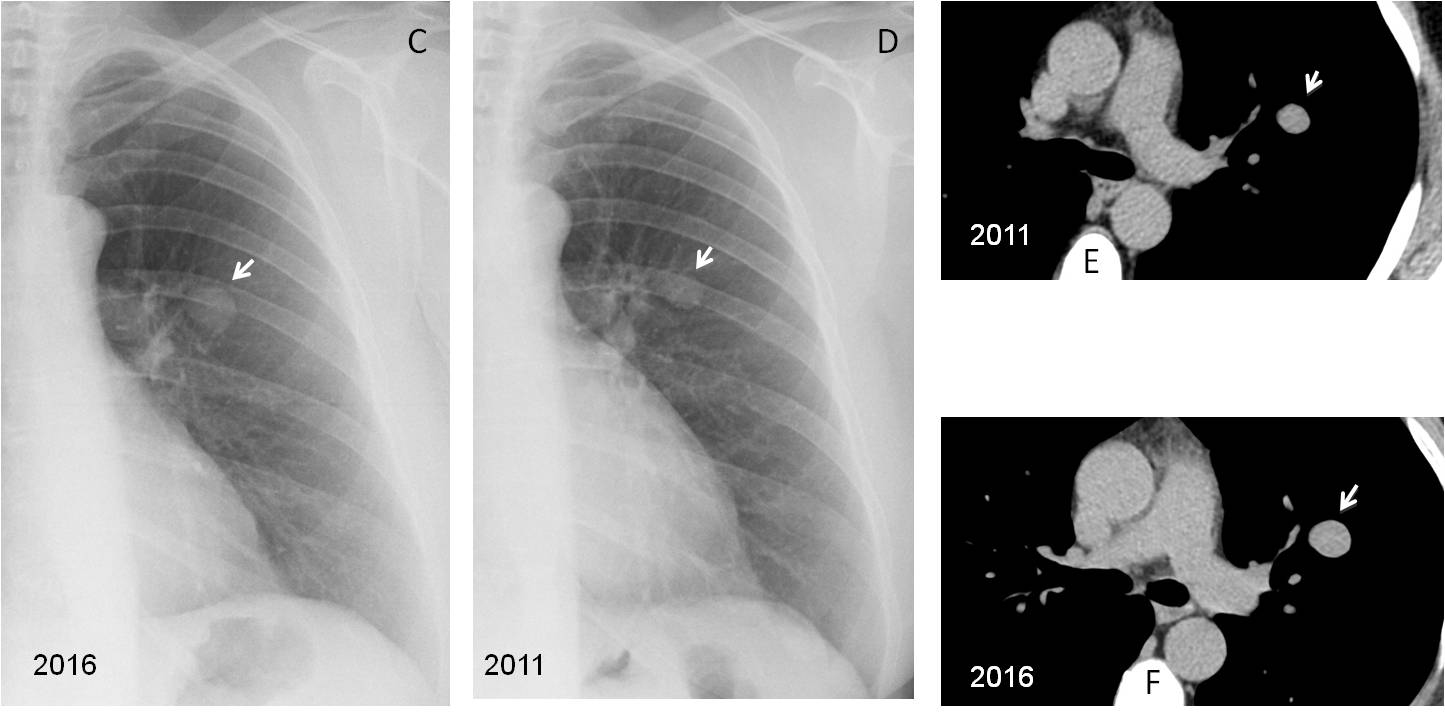
Fig. 6

Follow Dr. Pepe’s advice:
1. Interpretive errors account for 12% of all reading errors.
2. The most common interpretive error results from faulty reasoning.
3. Being familiar with normal variants, handling differential diagnoses, and keeping up with related knowledge are the best ways to avoid interpretive errors.


Hello,
there is an evident elongation of the descending aorta with an increased size (aneurysm dilatatation of the aorta), but with the Rx I can´t excluded a dissection.
The left hilum is increased in size and density, perhaphs because of an increased pulmonary artery.
When the left hilum is overlapped by the aorta it seems increased in opacity. It is a common error. Do you think the left hilum is enlarged in the lateral view?
No, in the lateral view it´s normal.
Thanks!!!
There is an obliteration of the retrocardial space!!
Due to the elongated descending aorta
4. Any of the above.
The descending aorta is definitely elongated and widened. Chest pain is usually present with dissection, but it cannot be ruled-out based on this radiograph.
….professore…..la risposta dovrebbe essere la 4: …con la radiografie standard osserviamo l’allungamento “sigmoide” di tutta l’aorta,,,la sua evidente dilatazione nel tratto discendente( confronto con l’aorta ascendente) …ma in tutta onestà non riesco a fare dd tra l’aneurisma, la dissezione o l’ematoma intramurale…..ci sarebbe tutta una clinica, di emergenza nel caso di dissezione…oltre naturalmente a segni di insufficienza del ventricolo sx, con scompenso del piccolo circolo e versamento pleurico….però siamo qui per imparare ed aspettiamo che il “galactico” ci illumini….
Elongation of descendent aorta with appearance serpiginous.
Aortic Aneurysm in proximal descendent aorta.
It seems to me that there is a change of caliber in the distal thoracic aorta, but it may be because of the tortuosity.
Left Ventricle rounded outline, apex sligth up.
Diffuse osteopenia.
This is aortic elongation due to the old age.
Welcome back!
Why the ascending aorta is not elongated?
because of its normal anatomy. ascending aorta is the part of aorta between the aortic valve and arch of aorta, it is short and limited by these anatomic structures. that is why here she could be mainly widened but not elongated
and also can not be aortic dissection excluded
Any of the above
1+2+3 😀
+ trachea shifted to the right
Elongated thoracal aortic with probable ektatic/aneurysmatic aortic descendens (seems to more than 3,5cm in diameter). Slight shift of the trachea to the right. There is kinking of the aorta in the thoraco-abdominal junction. Aortic aneurysm cannot be rouled out by this chest x-ray as already mentioned. Both hila and lungs are normal.
So for me any of the above is the correct answer.
Perhaps we have a semantic problem: to
me, an elongated aorta is tortuous but has a normal caliber. In this patient, as you rightly say, the descending aorta is dilated. According to my criteria (not universal, of course), the correct answer cannot be any of the above.
Thank you for this advice. I have to admit that until now I used the term elongated to describe the aortal appearance not keeping in mind the caliber, which could be normal or ectatic/aneurysmatic.
Therefore, three: aortic aneurysm.
Actually, you are right calling the aorta elongated, because most of the times the inner wall is not visible and it cannot be determined whether or not there is dilatation. The case presented is the rare one in which you can see both walls and determine that there is dilatation.
Elongated aorta, which also shows an increased diameter, consistent with aortic aneurysm.
Shift of the trachea to the right.
I believe an aortic disection cannot be excluded with this XRay and the patient’s symptoms should be considered.
As I mentioned in the clinical history, the patient is asymptomatic.
…carissimo professore…..ti pongo una domanda e ti faccio una osservazione….la brusca differenza di calibro tra aorta ascendente e discendente poteva sospettare anche un esteso ematoma intramurale?…..di fronte all’ rx , anomalo, la diagnosi di certezza poteva essere fatta solo con la Tc, nella dd tra queste due patologie?…..ti seguo sempre con interesse e penso che i 2 punti di distacco possano sempre essere recuperati!