Dr. Pepe’s Diploma Casebook: Case 109 – The Wisdom of Dr. Pepe (Chapter 2) – SOLVED!
Dear Friends,
To continue with the second chapter of The wisdom of Dr. Pepe, I am showing radiographs of a 75-year-old man with cough and haemoptysis.
What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.


Findings: chest radiographs show emphysematous lungs with chronic fibrotic changes in the RUL (A, arrow) and left middle lung. The most important finding is an irregular opacity projected over the descending aorta, visible only in the lateral view (B, arrow).
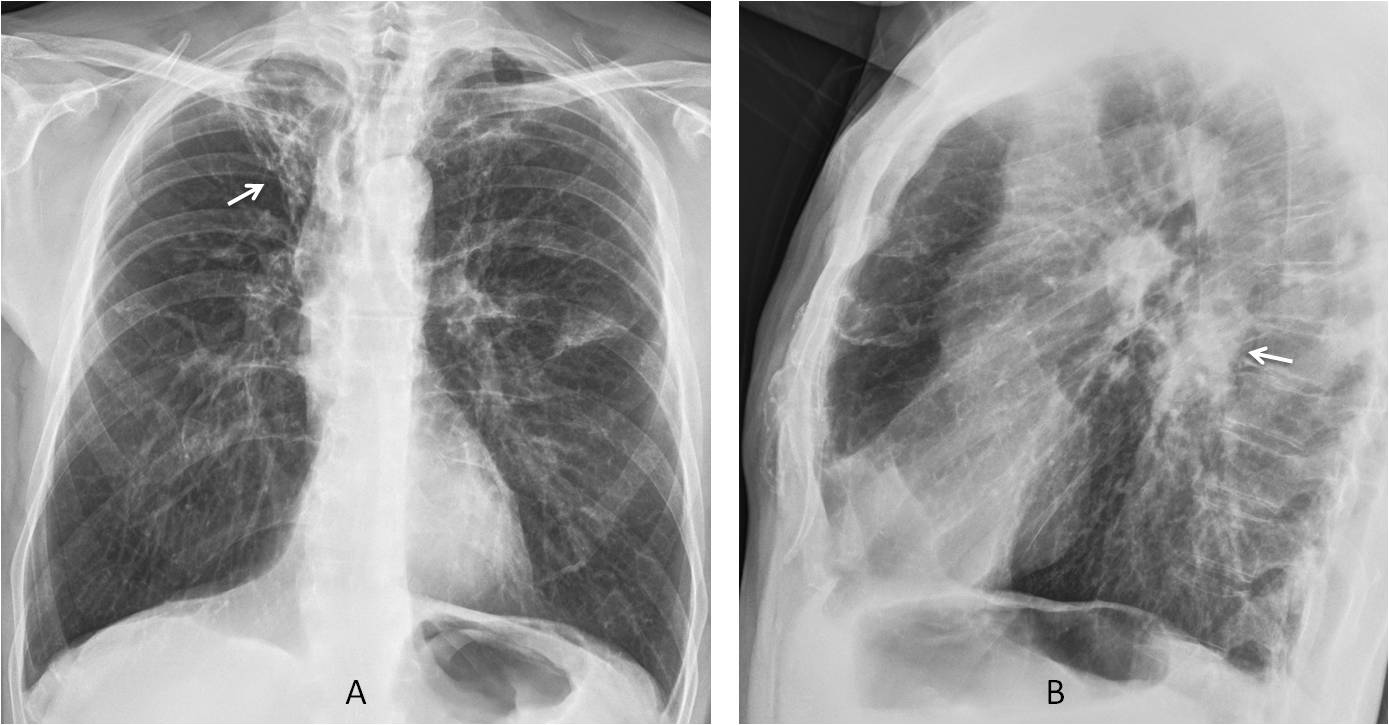
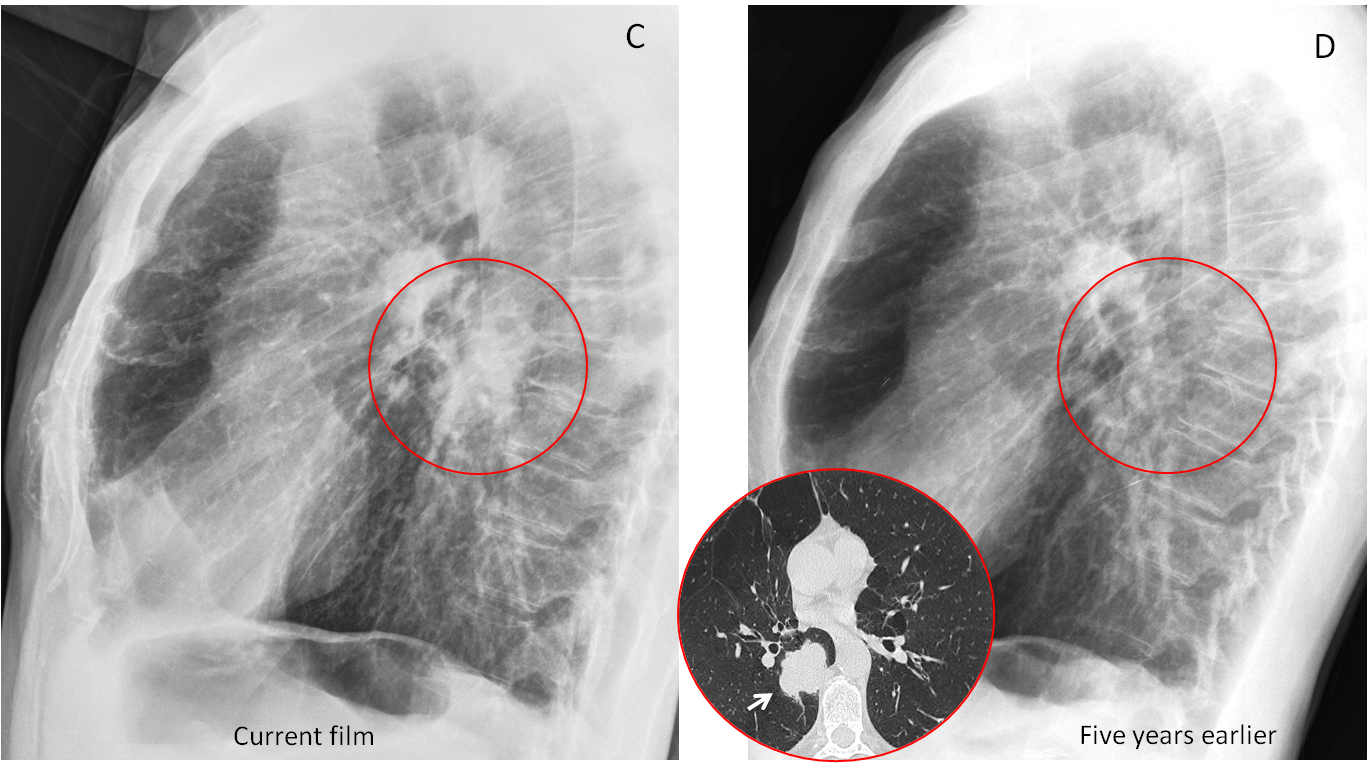
Comparison with a previous lateral film shows that the opacity was not present five years earlier (C and D, circles). Axial CT confirms an irregular mass hidden in the azygoesophageal recess (insert, arrow).
Final diagnosis: Carcinoma of the lung, hidden in the PA view
In the second chapter of The Wisdom of Dr. Pepe I intend to discuss the lateral view (lv), the second component of the equation:
D = (bc + lv + ps + chl) e
My purpose is to emphasise the importance of the lateral view in the detection of chest abnormalities. When examining other organs (skeleton, breast, etc.), it is mandatory to take two right-angle projections (Fig. 1). I see no reason why this practice should not also be applied to chest imaging.
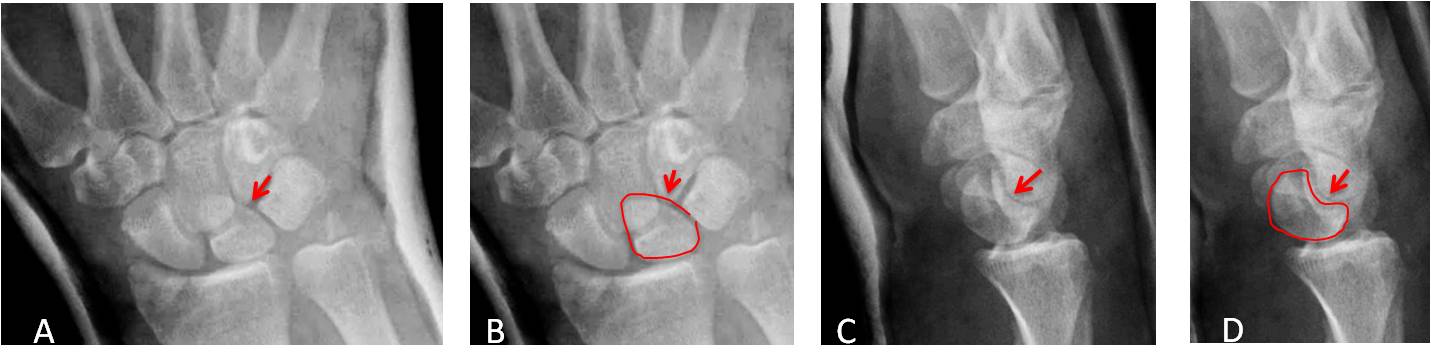
Fig. 1
Fig. 1. Traumatic lunate dislocation. The PA view shows that the lunate has a triangular shape, a sign of possible dislocation (A and B, arrows). Lateral projection confirms the lunate dislocation (C and D, arrows).
The main reasons to obtain a lateral view of the chest are:
To visualise blind areas in the PA view
To clarify lesions that are poorly depicted in the PA view
As I’ve already mentioned, around 25% of the lung surface is hidden in the PA radiograph by other structures (blind areas). These areas may be better visualised in the lateral film, which serves as an aid to detect abnormalities that might be missed otherwise. The blind areas are sketched in Fig. 2, including the thoracic spine, which is poorly seen in the PA view.
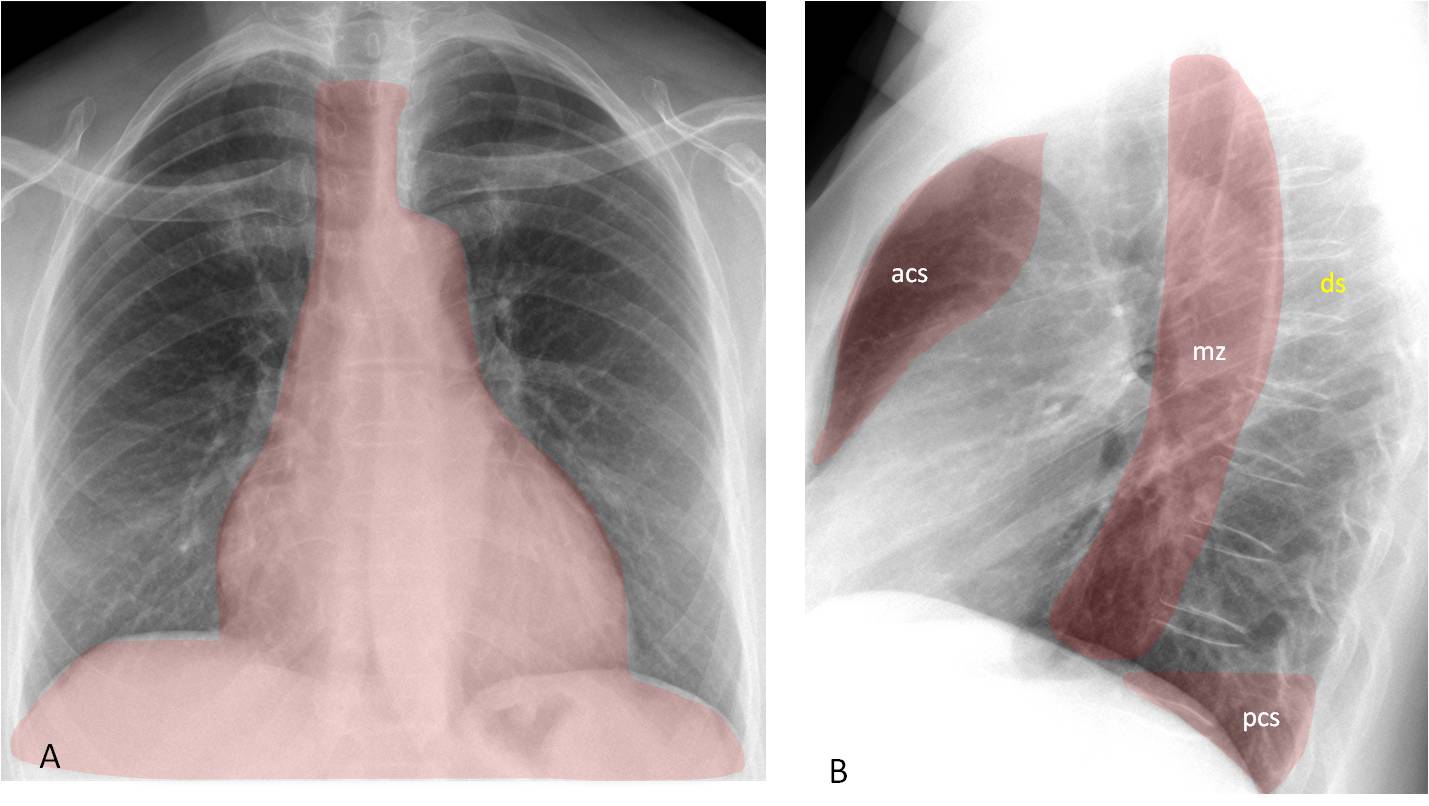
Fig. 2
Fig. 2. The shaded area (A) depicts the blind areas in the PA view. They are visible in the lateral view (B) as the anterior clear space (acs), middle zone (mz), and posterior clear space (pcs). The dorsal spine (ds) is also included.
Blind areas were discussed in Diploma cases 100 and 101 and I don’t think it is necessary to review the subject again. As a reminder, I’m showing an example of disease detected in the lateral radiograph, not visible in the PA view (Fig. 3).
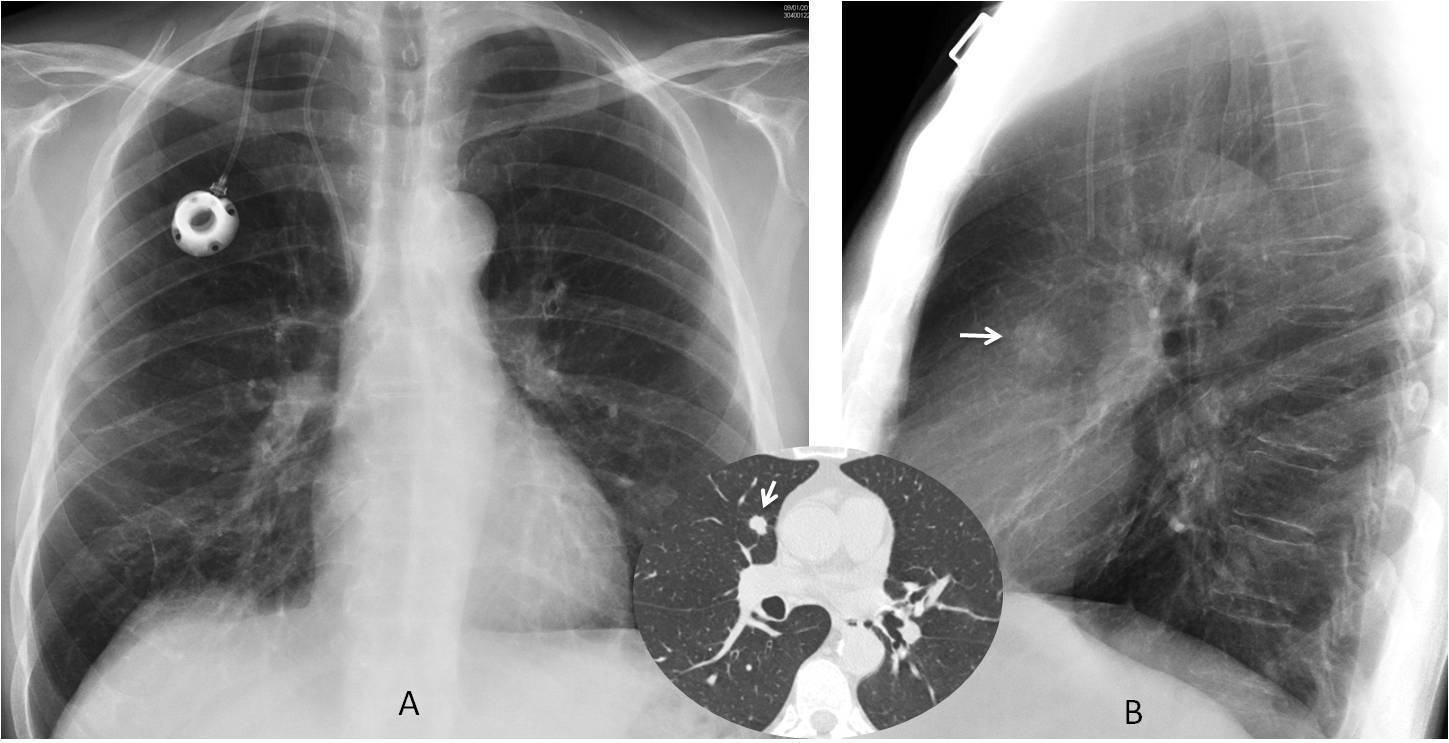
Fig. 3
Fig. 3. 54-year-old man with colon carcinoma. Lateral view shows a nodule in the anterior clear space (B, arrow), hidden behind the right hilum in the PA view (A). CT confirms the nodule (insert, arrow). Surgically proven metastasis.
Aside from depicting the blind areas, the lateral view also contributes to interpreting abnormalities that may have a confusing appearance in the PA view and are more clearly seen in the lateral radiograph. To confirm this, examine the images below (Fig. 4, A and B) and try to determine what objects they represent.
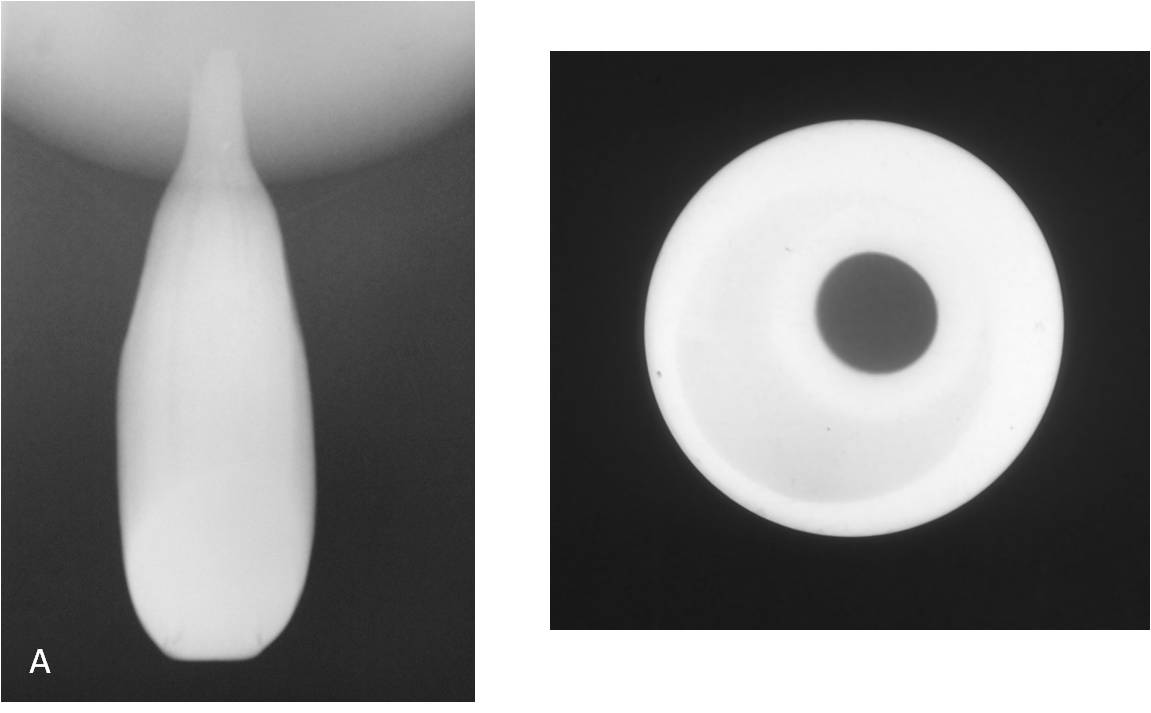
Fig. 4
Fig. 4. Radiographs (A and B) of two familiar objects.
The right-angle view shows that the first image corresponds to a banana (C) and the second to a bottle (D). This is an example of the usefulness of the right-angle view (ie, lateral view) to clarify inconclusive images seen in a single projection.
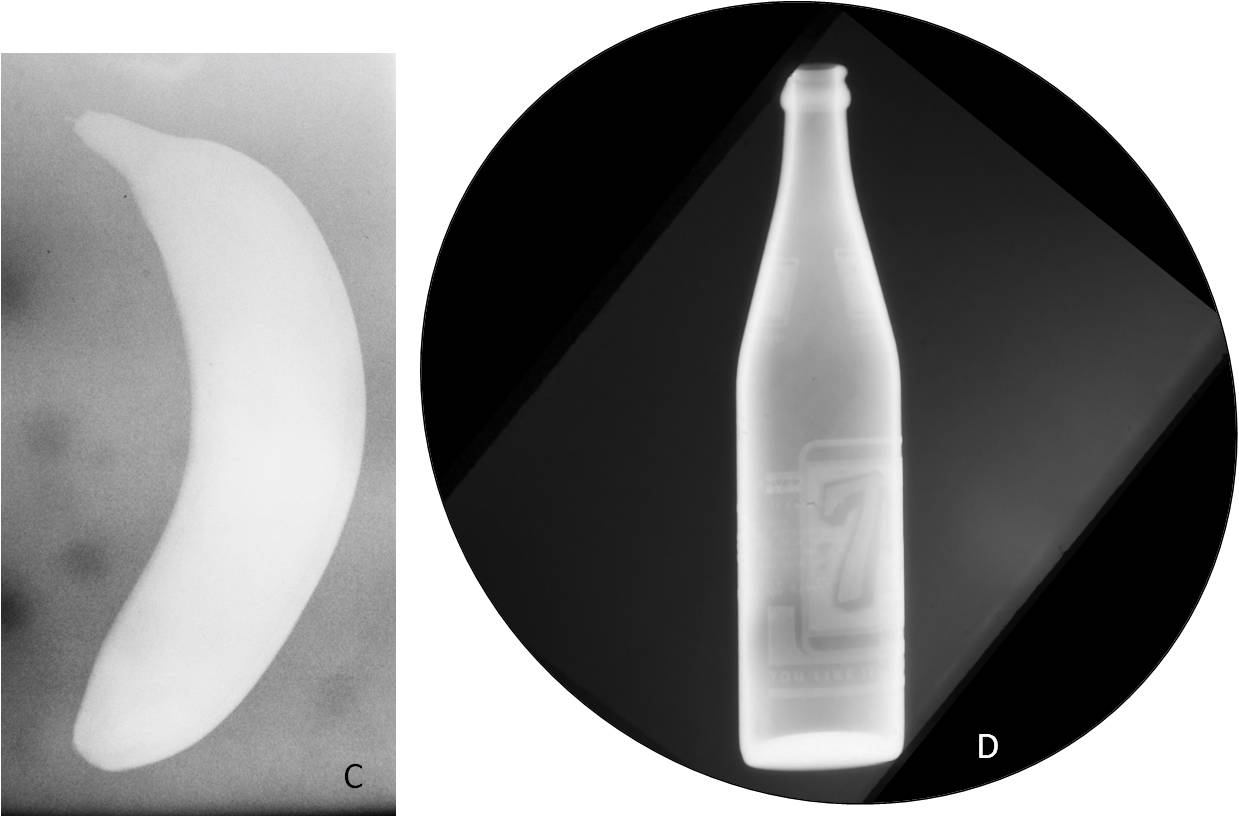
Fig. 4
It is difficult to determine which abnormalities may be better visualized in the lateral view, but I’ll do my best. In my opinion, the conditions that most benefit from a lateral view are:
1. Hilar abnormalities
2. Some types of lobar collapse
3. Abnormalities in the major fissures
4. Abnormalities of the pleura/chest wall
Hilar abnormalities are important because more often than not they are related to malignant disease. The lateral view helps to differentiate true hilar pathology from lesions in front of or behind the hilum that simulate hilar pathology in the PA view (Figs. 5 and 6).
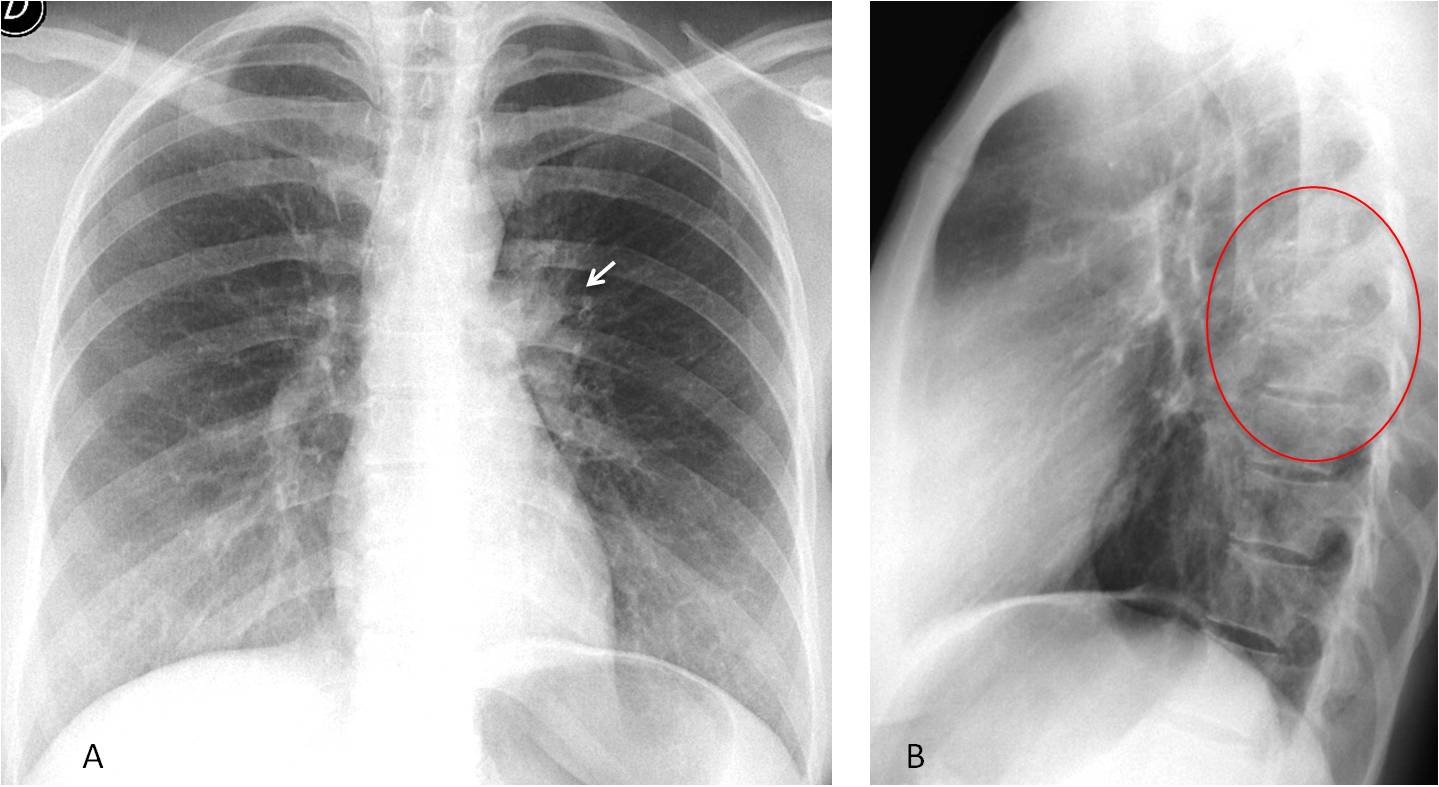
Fig. 5
Fig. 5: 28-year-old man with cough and fever. PA radiograph shows an apparently abnormal left hilum (A, arrow). Lateral view depicts a posterior pulmonary infiltrate (B, circle), simulating an abnormal left hilum in the PA view.
Follow-up films two weeks later show that the hilum has a normal appearance (C and D, arrows) and the infiltrate has disappeared (E and F, circle). Diagnosis: acute pneumonia.
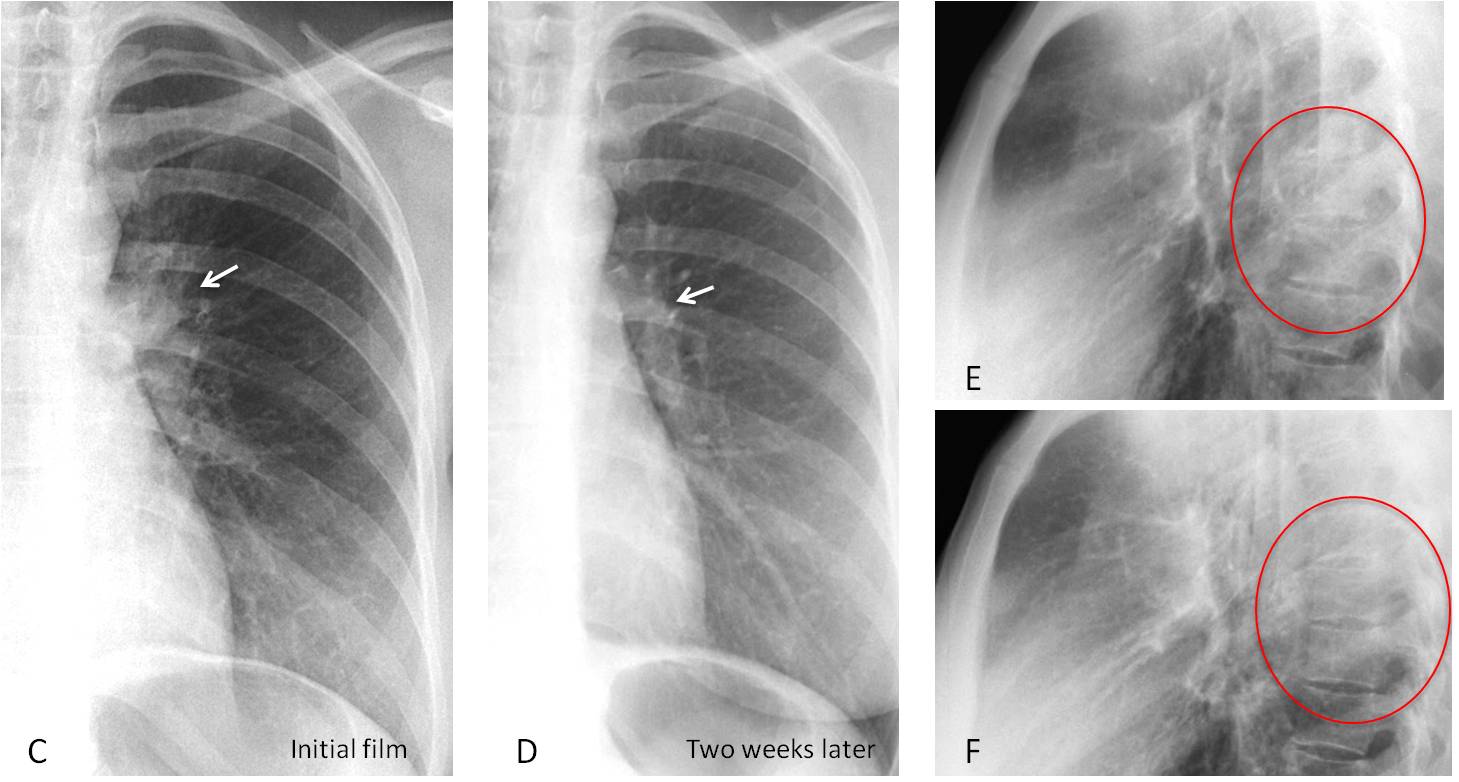
Fig. 5
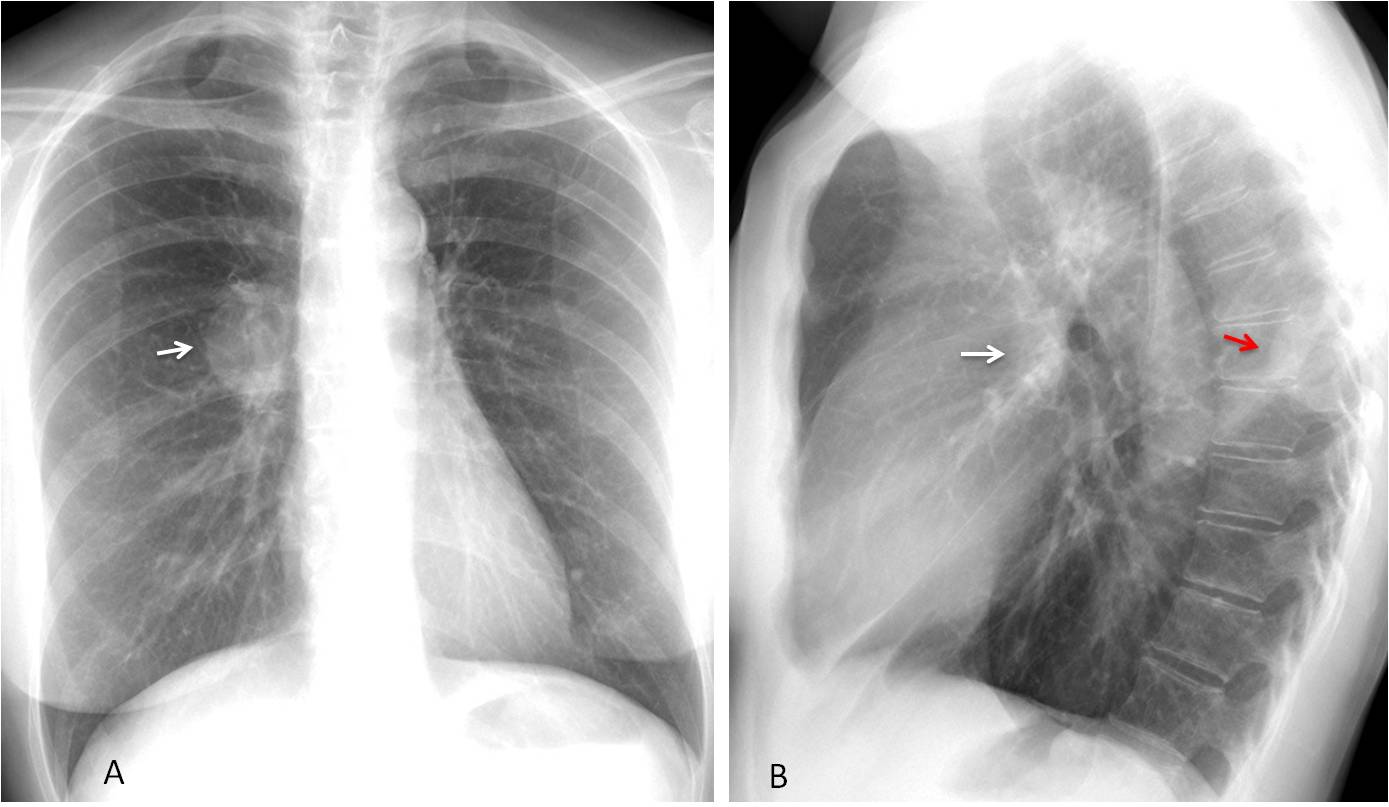
Fig. 6
Fig. 6. Neurogenic tumour projected over the right hilum in the PA view, simulating a hilar mass (A, arrow). Lateral radiograph shows that the right hilum is normal (B, white arrow). The tumour is visible as an extrapulmonary lesion in the posterior mediastinum (B, red arrow).
It is important not to overlook lobar collapse because it is a common presentation of lung carcinoma. Collapse of three of the lobes (RUL, RLL, and LLL) is easily diagnosed in the PA view. However, the last two (RML and LUL) may offer a confusing appearance in the PA radiograph and are better identified in the lateral view (Figs. 7 and 8)
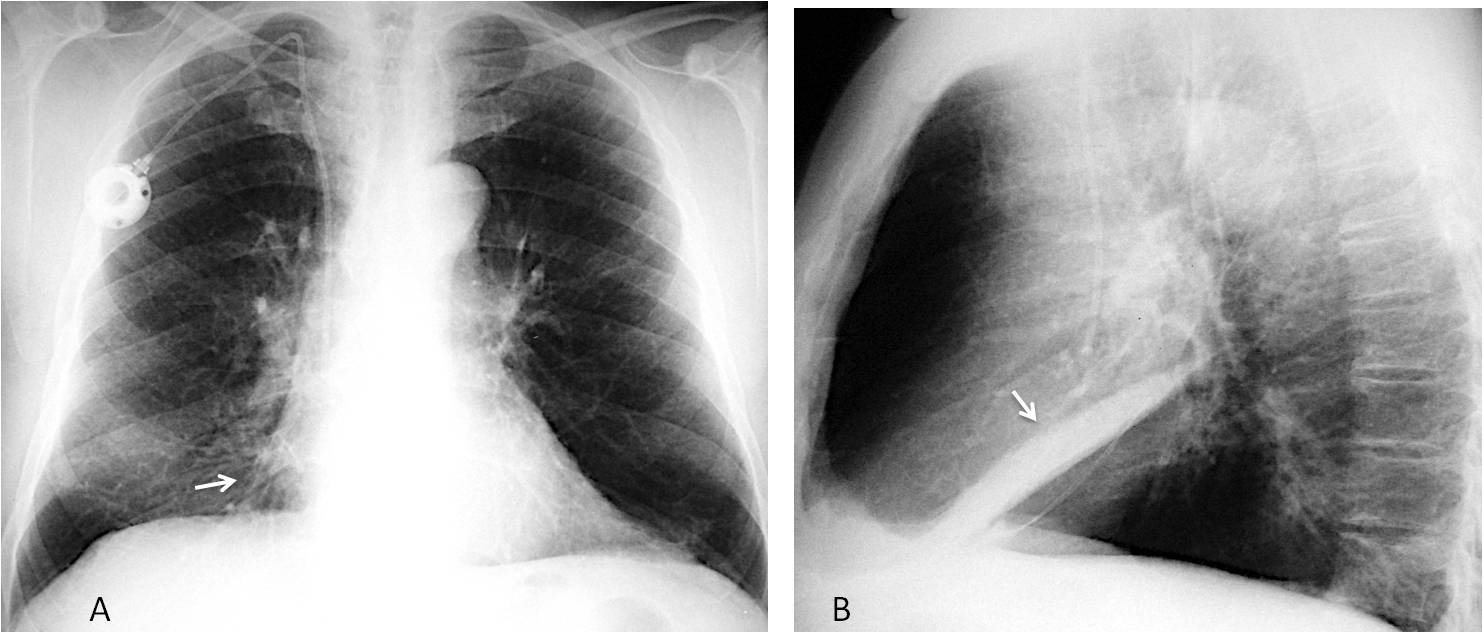
Fig. 7
Fig. 7. Chronic RML collapse. The only indication in the PA view is slight blurring of the right heart border (A, arrow). The lateral view clearly identifies RML collapse (B, arrow).
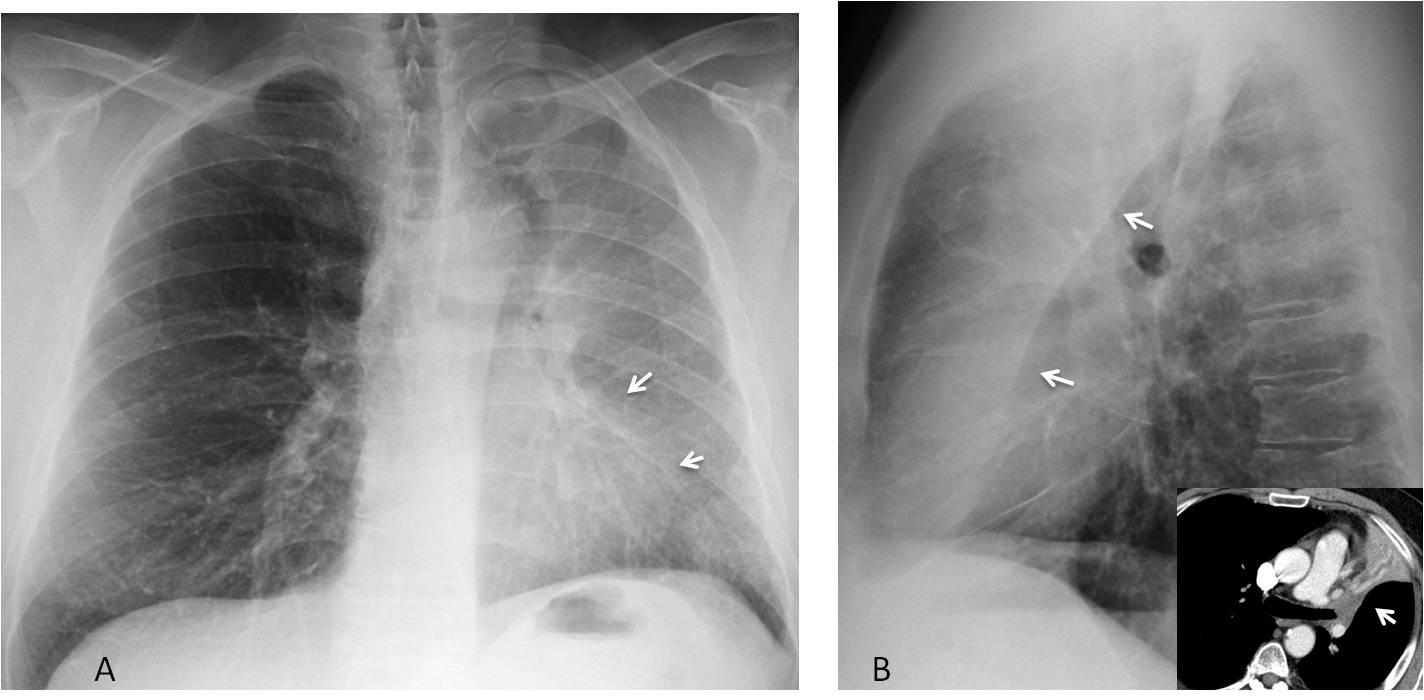
Fig. 8
Fig. 8. LUL collapse in a patient with endobronchial carcinoma. PA radiograph shows haziness of the left lung, with blurring of the left heart border (A, arrows). Lateral view shows the typical sharply-defined retrosternal opacity, which corresponds to the collapsed lobe limited by the left major fissure (B, arrows). Axial CT confirms the endobronchial obstruction and the collapsed lobe (insert, arrow).
Fluid and tumours within a fissure have a typical ovoid shape with tapering ends. When located in the major fissure, they have a deceiving appearance in the PA view because the fissure offers an oblique face to the X-ray beam. The lateral view clearly depicts the typical appearance (Figs. 9 and 10).
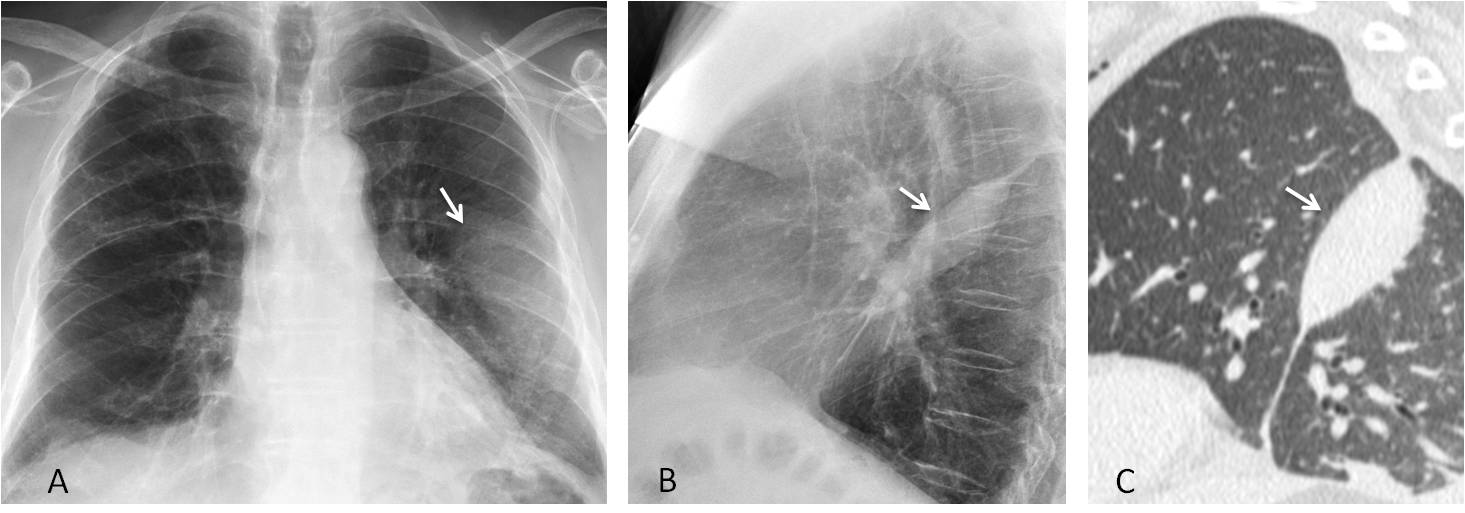
Fig. 9
Fig. 9. 59-year-old man with loculated fluid in the left major fissure. PA film shows a nondescript opacity in the left middle lung (A, arrow). Lateral view depicts the typical appearance of an intrafissural lesion (B, arrow). Sagittal CT confirms the findings (C, arrow). The most common etiology of a fissure mass is heart failure, in which pleural fluid may collect within the fissures.
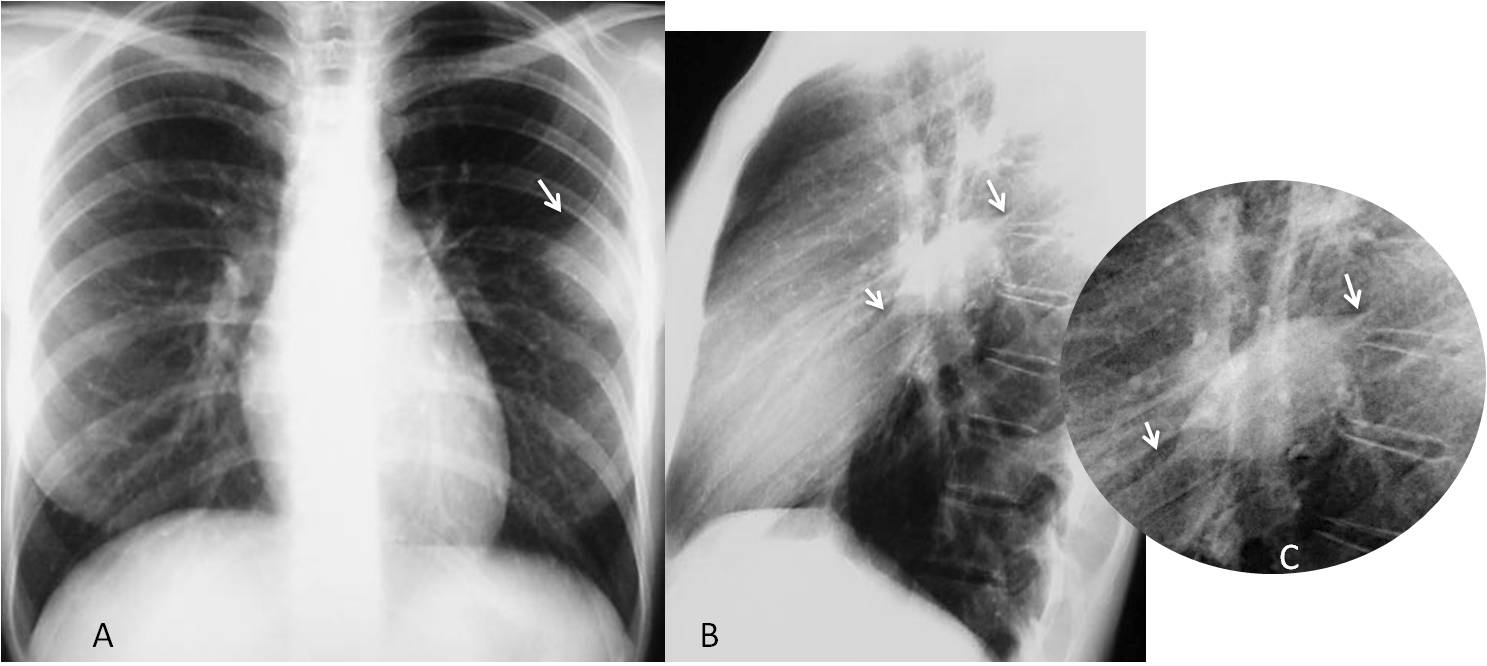
Fig. 10
Fig. 10. 35-year-old woman with a fibrous tumour in the left major fissure. PA radiograph shows a poorly defined peripheral opacity (A, arrow) that simulates a lung tumour. Lateral view demonstrates the typical ovoid shape and tapering edges, better seen in the cone-down view (B and C, arrows).
Disease of the pleura/chest wall may offer a blurred appearance in the PA view when seen en face. The extrapulmonary location is easily recognizable in the lateral projection (Figs. 11 and 12).
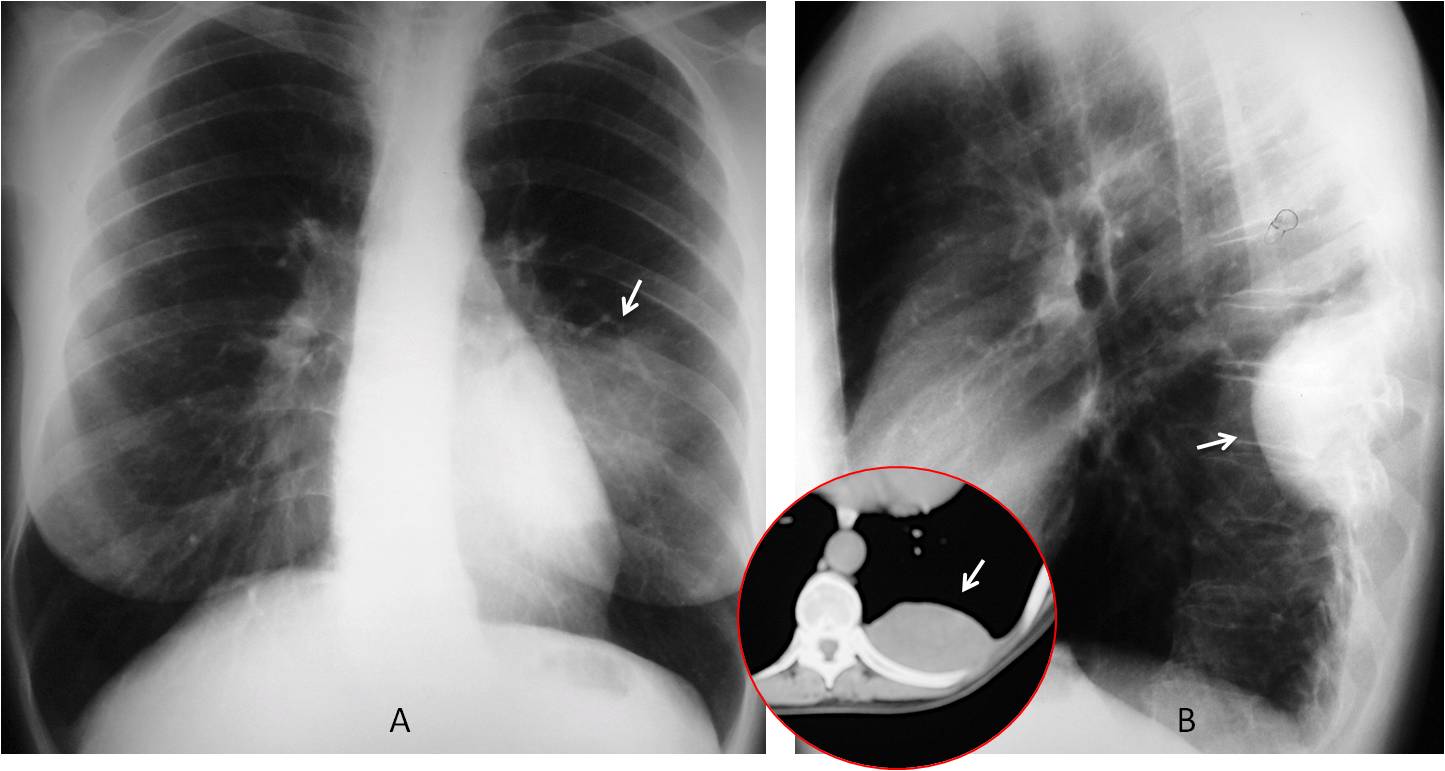
Fig. 11
Fig. 11. 47-year-old woman with chest pain. PA radiograph depicts a poorly defined opacity, apparently located in the left lung (A, arrow). Lateral view shows that the lesion is clearly extrapulmonary (B, arrow), confirmed with CT (insert, arrow). Fibrous tumour of pleura.
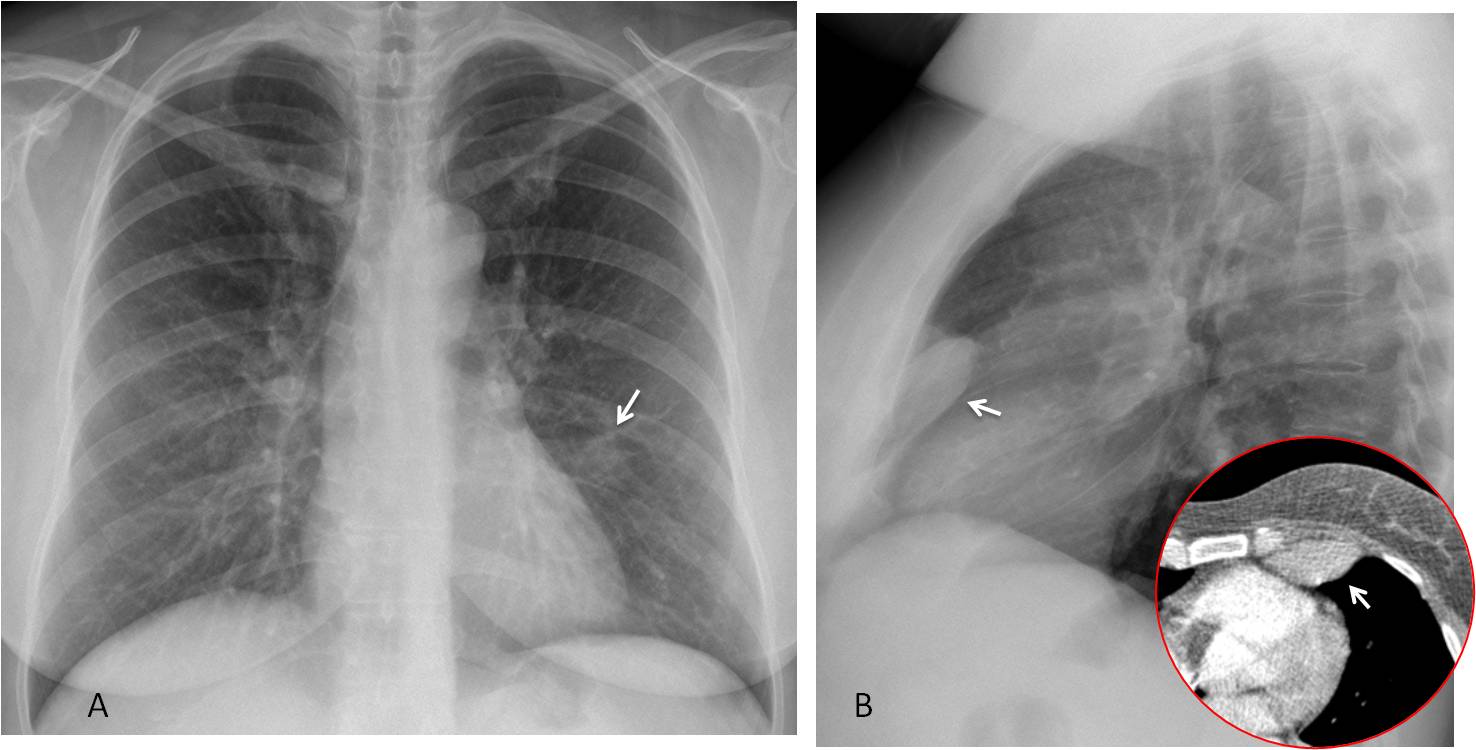
Fig. 12
Fig. 12. 39-year-old woman with breast carcinoma. PA radiographs depict a poorly defined opacity in the left lung (A, arrow). Lateral view shows an extrepulmonary anterior lesion (B, arrow). CT confirms the location of the lesion (insert, arrow). Diagnosis: fibrous tumour of pleura.
In single calcified pleural plaques, high KV techniques tend to “burn” the calcium. When seen en face, they may simulate a pulmonary infiltrate. Seen in profile they appear as a calcified line (Fig. 14) and the diagnosis is then apparent.
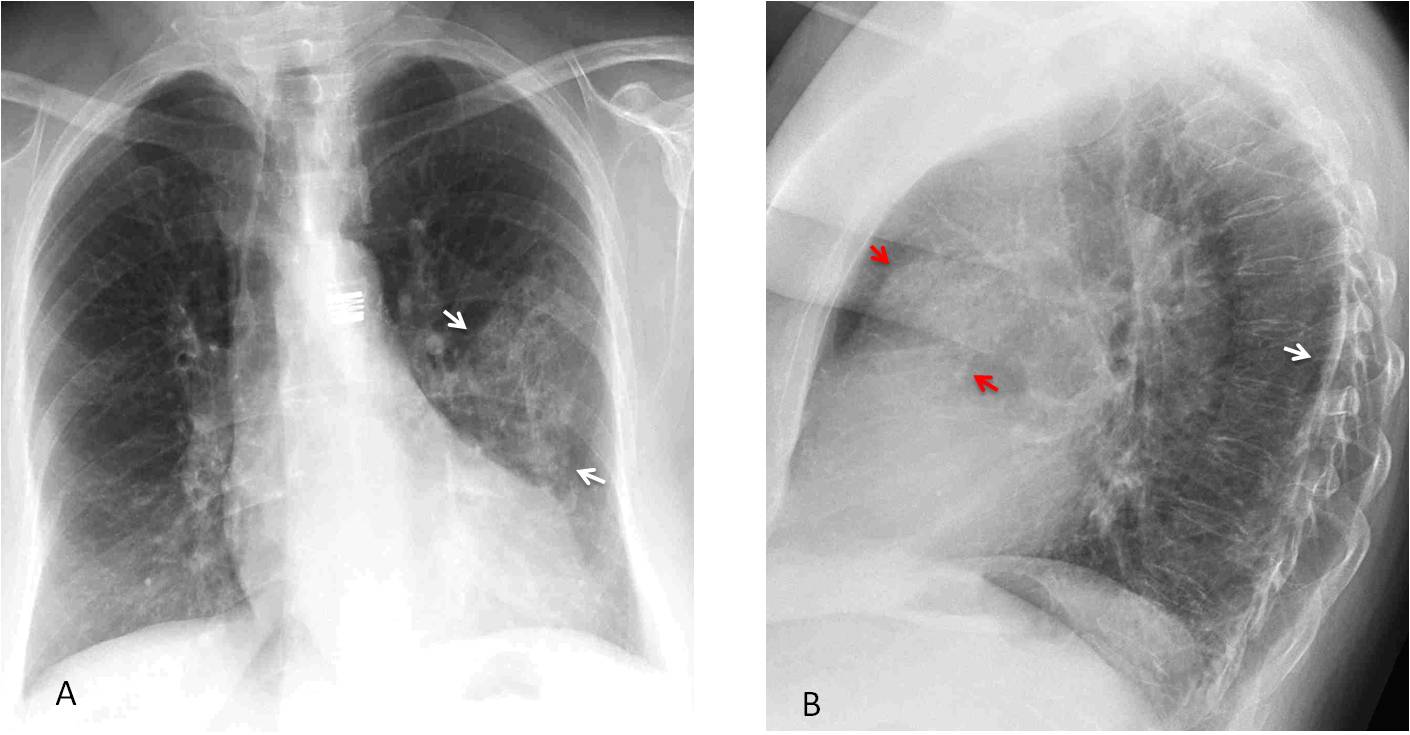
Fig. 14
Fig. 14. 52-year-old woman with two pleural plaques. The PA radiograph shows the plaques en face, simulating a pulmonary infiltrate (A, arrows). In the lateral view, the posterior plaque is depicted as a calcified line (B, white arrow), whereas the anterior one is more oblique and simulates a rounded opacity (B, red arrows).
Sagittal CT clearly shows the anterior (C, arrow) and posterior (D, arrow) plaques .
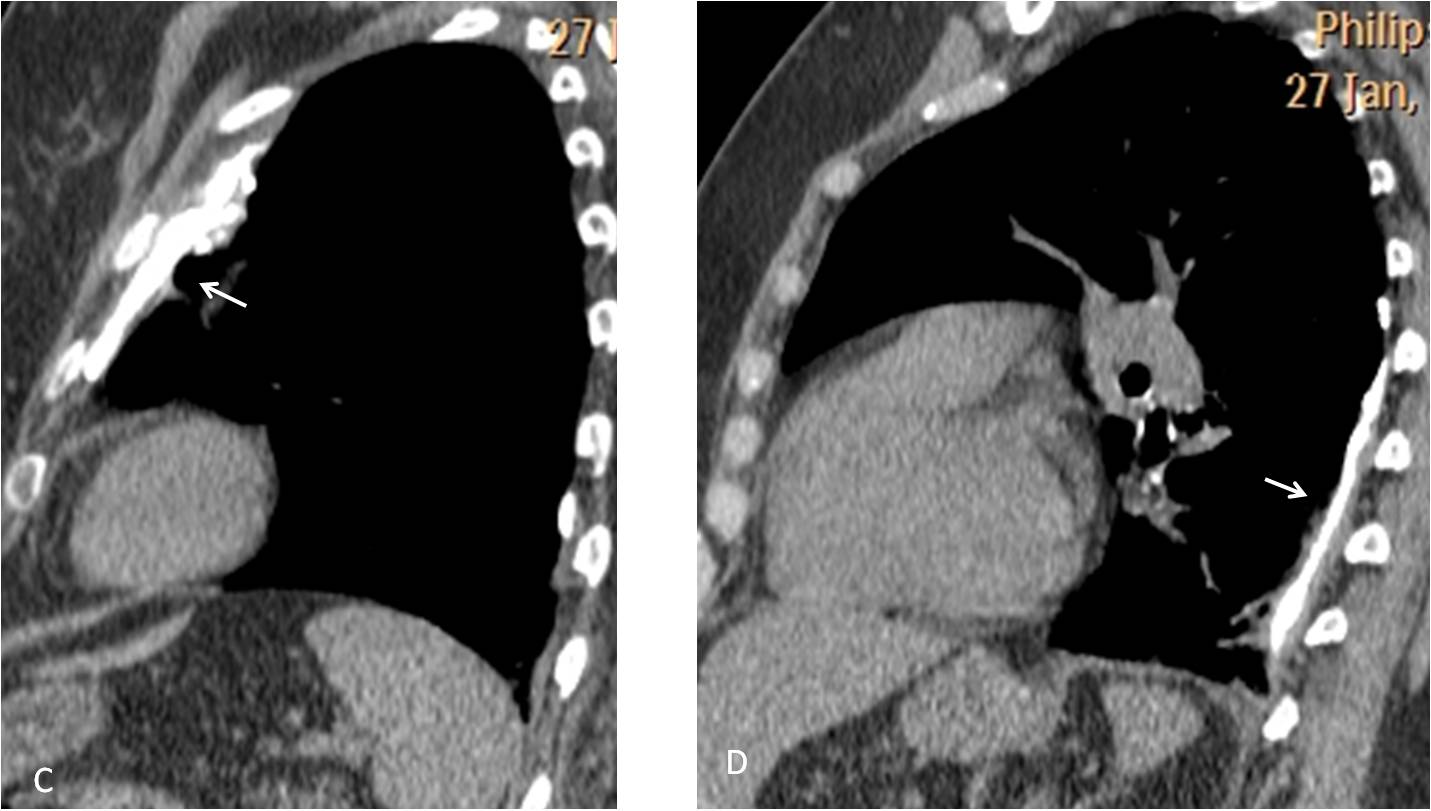
Fig. 14
Dr. Pepe’s second commandment:
Thou shalt always take a lateral view:
- To examine the blind areas in the PA view
- To clarify findings in the PA radiograph


Good morning!
Emphysematous thorax with bilateral apical tracts, more evidente in the right region where I can see an apical cap and a nodular lesion in the paratracheal margin and bronchiectatis (perhaps fibrotic changes because of a chronic pathology or a new lesion growing over them).
In the lateral view the hila are enlarged with high density, and there is an alveolar opacity in the LLL (like in the PA view).
So haemoptysis because of chronic changes or a neoplasm.
Hello!
– Emphysematous thorax.
– Bilateral apical fibroreticular opacities + bronchiectasis, with upward retraction of the hila.
– Tracheal displacement (apical retraction vs goiter)
– Posterior LLL nodular opacities.
-Bilateral apical fibrosis and cavitation
-Patchy pleural thickening /calcifications
-Tracheal narrowing
-Peripheral tree in bud pattern
mostly Tuberculosis
Emphysematous thorax
bilateral apical pleural caps right more than left. Fibrotic changes in the right apical region in the form of tracheal deviation and broncciectasis.
a nodular lesion in the right apical region.
an opacity in left mid zone could represent a lung nodule however could be due to the indentation by the costochondral junctions.
In the lateral view nodular opacity is seen in the hila.may represent lymph nodes.
So haemoptysis because of bronchiectatic changes or a neoplasm.
Corect reading
…carissimo Prof……la trachea in AP e LL è improntata e ristretta , da una opacità di massa….
Where is the right atrium of the heart?
Extensive emphysematous and fibrotic changes. Hilar lymphadenopathy. There is a nodule in the periphery of the left lung with peripheral clearing. This may be an aspergilloma.
First to note the underlying chronic pathology:
1. Emphysematous changes (hyperinflated lungs, increased retrosternal clear space…)
2. Old TBC (fibrotic changes in the apical zones, especially on the right, where some small cavitations are present, upward traction of hila, pleural caps…).
There is also an ill defined nodule in the middle left zone, which on LL seems to be placed posteriorly, possibly also scaring from TBC.
However, I see other abnormalities:
– Although both hila are elevated, right hilum is higher then the left one, indicating volume loss.
– There also appears to be hillar mass on the right.
– Trachea is narrow in the middle part and deviates to the right, as if being pushed by the paratracheal mass on the left, and not because of aortic knob, which is below the deviation.
– On the lateral view trachea is not vertical, but is displaced posteriorly in it’s lower part by a mass at the level of right pulmonary artery.
– There is also soft tissue structure anterior to the trachea.
Everything said could be due to reactivated TBC with lymphadenopathy, but neoplasm can’t be excluded, so I think this patient warrants a CT exam.
Detailed and accurate discussion
Emphysema, probable tb sequelae (pleural caps, bronchiectasis, scarring predominant in the upper lobes, which determine hilar elevatio and right tracheal dislocation).
Middle lobe atelectasis also looking residual.
Narrowing of trachea – could it be the cause of synptoms? (looks saber sheath like in the profile).
Bilateral nodular opacities more numerous on the LLL – tb? Mets? Angioinvasive aspergilosis?
Nice case, dr pepe! Looking forward to your insight!
Sorry I could not make any comment this week. Case was presented to emphasize the importance of the lateral view, in which the left hilum is abnormal and irregular. As many of you mentioned, CT should be done.
Thanks to you all for participating