I am taking a short break and will not post a case during the Christmas week. The next case will be posted on December 31st. In the meantime, I am presenting the chest radiographs of a 56-year-old man who came to the emergency room with chest pain and low-grade fever. He had a fracture of T-8 ten years ago.
1. Carcinoma of the lung
2. Pneumonia
3. Tuberculosis
4. None of the above
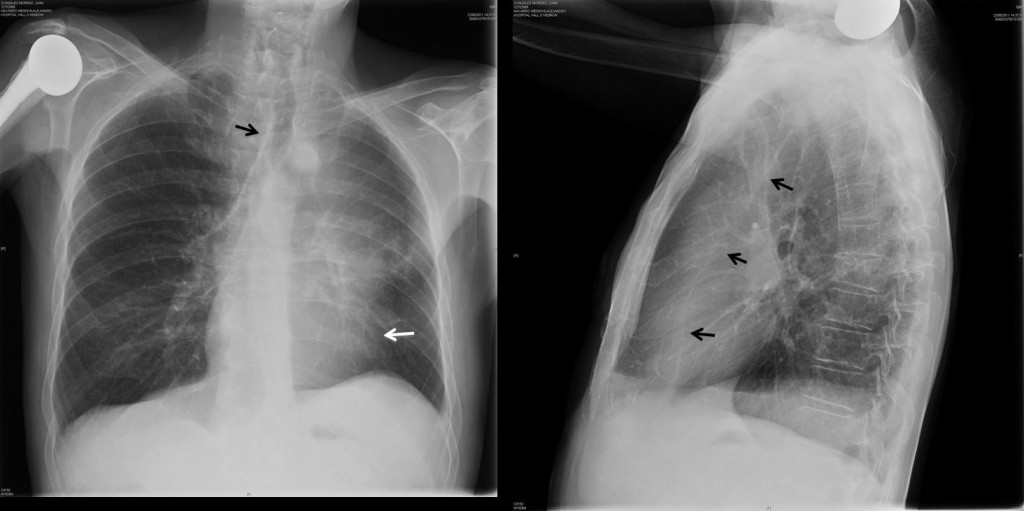
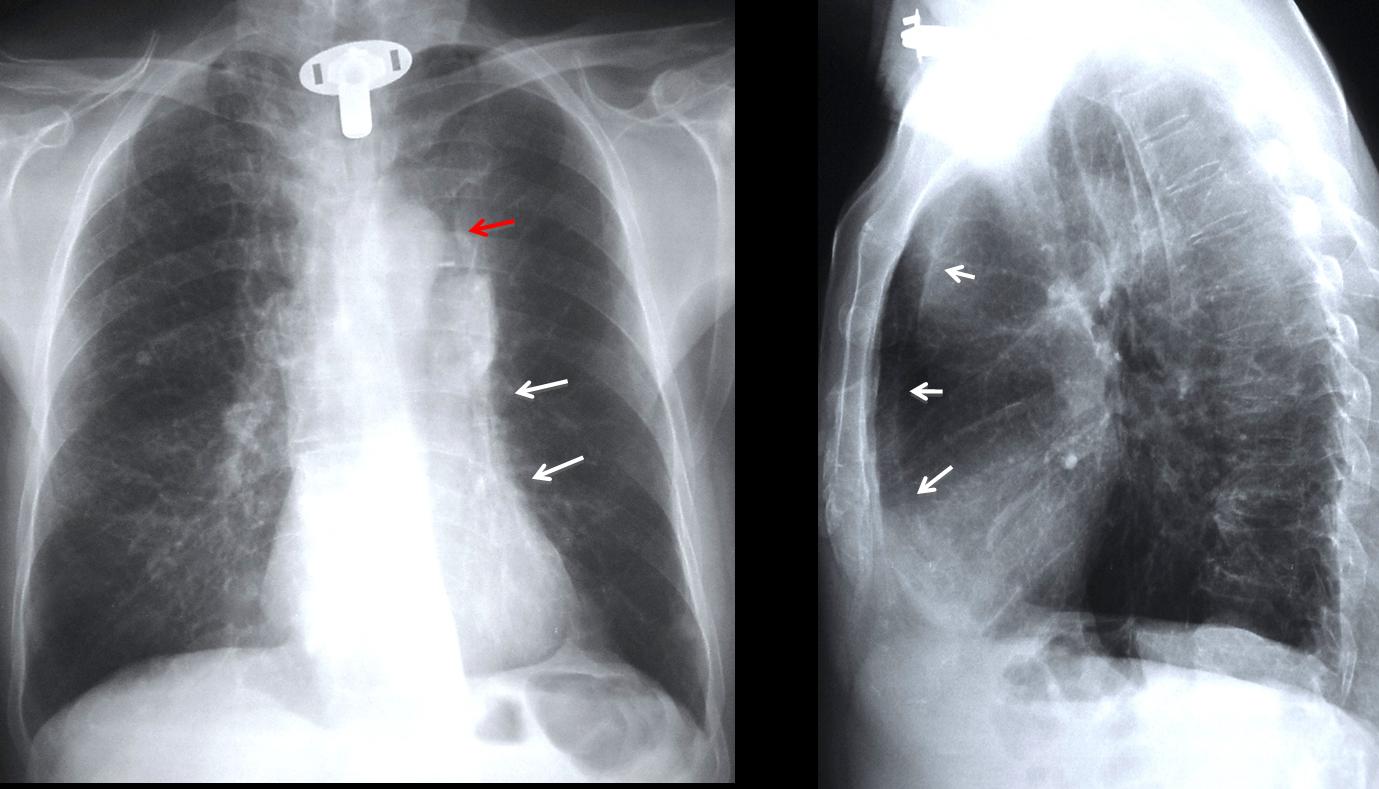
Fig. 3
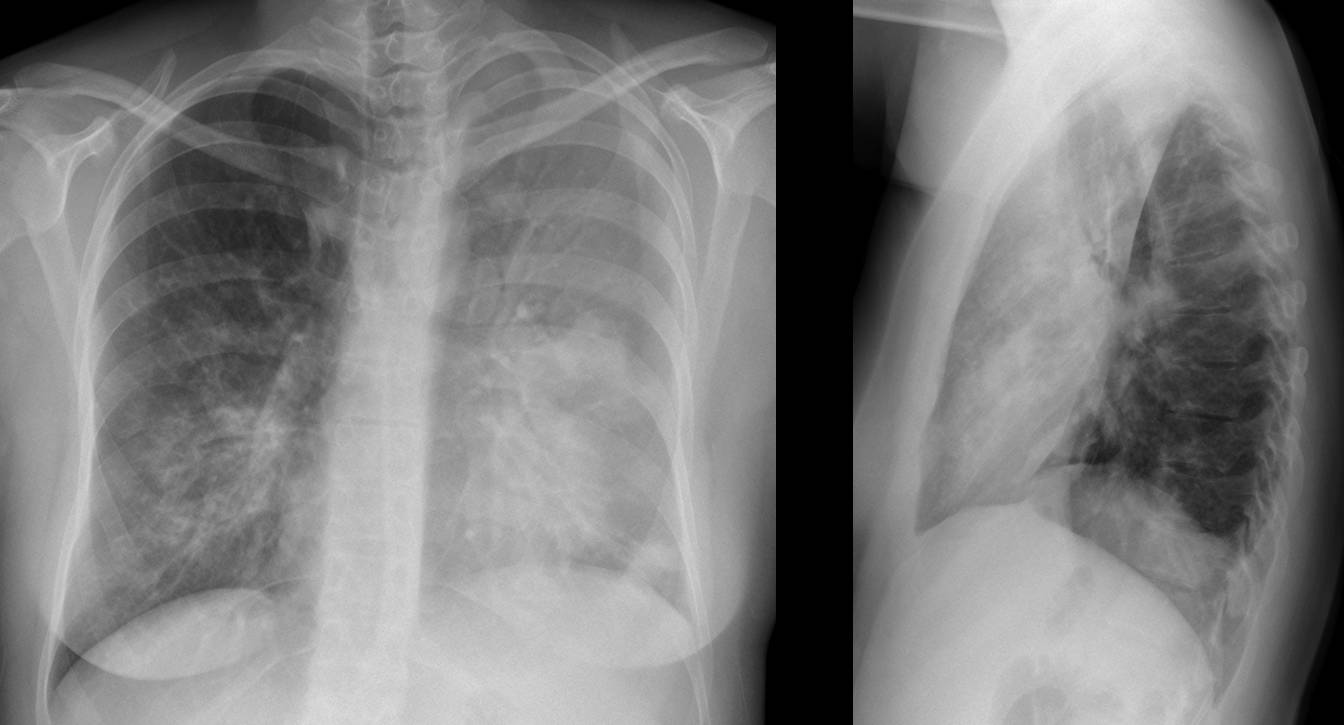
Findings: PA chest film shows a poorly-defined left lung opacity and hazy cardiac contour (white arrow). There is a loss of volume on the left side, as evidenced by displacement of the trachea (black arrow). Lateral view shows a retrosternal opacity that is well-limited posteriorly (arrows).
The radiographic appearance is typical of LUL collapse. Since malignant disease is the most common cause of collapsed LUL in adults, the likely diagnosis is carcinoma of the lung. Axial and coronal CT confirm the endobronchial tumour (arrows).

Fig. 4
Final diagnosis: squamous-cell carcinoma of left upper lobe bronchus
Collapsed lobes usually present a triangular appearance. The LUL collapses forward and flattens against the anterior chest wall, producing distinctive features that may be difficult to identify in some cases.
The imaging signs of LUL collapse are explained by the flattened lobe juxtaposed with the anterior chest wall, which produces blurring of the mediastinal and cardiac silhouette in the PA view (Fig. 2A). In about half the patients, compensatory expansion of the lower lobe outlines the aortic knob, rendering it more visible (luftsichel sign).
The findings are more evident in the lateral view, which shows the flattened lobe as a retrosternal opacity, sharply defined by the major fissure (Fig. 5B).
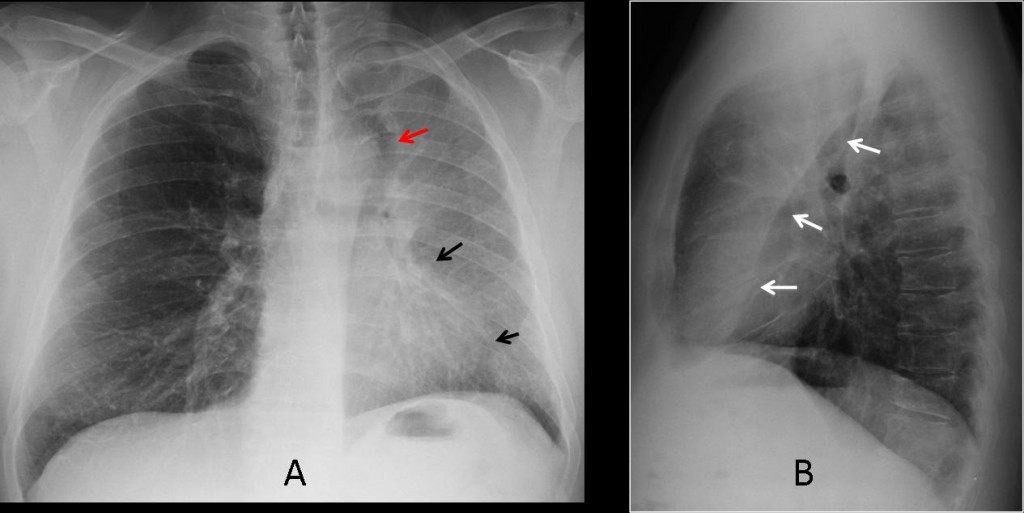
Fig. 5
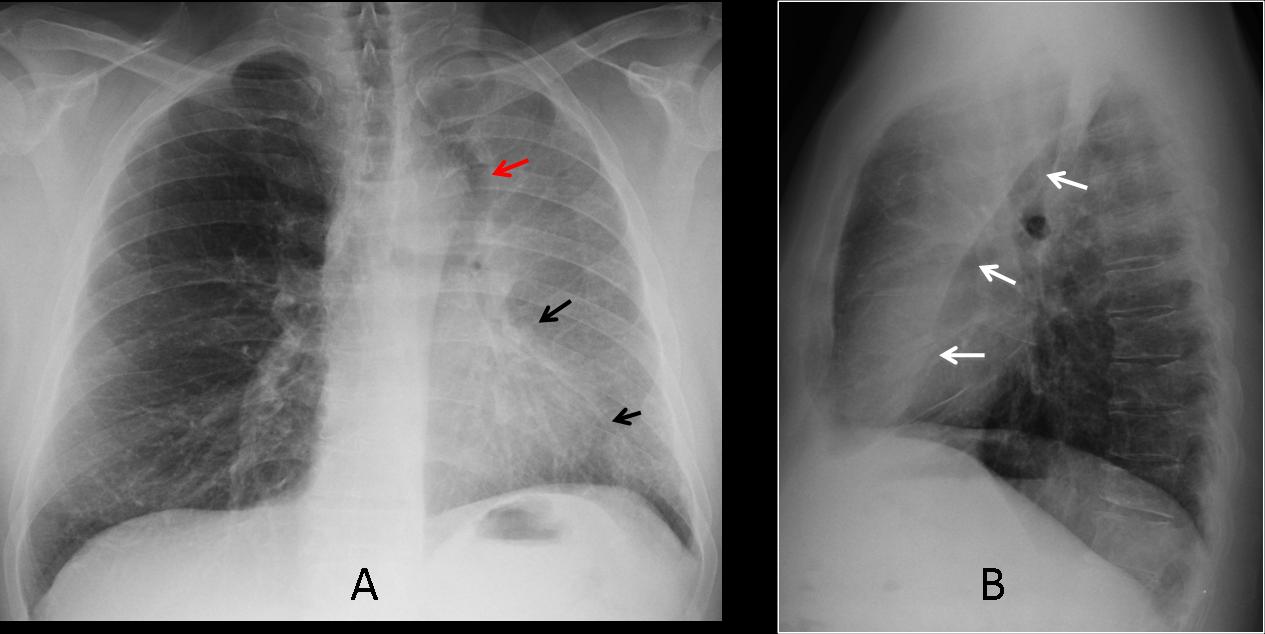
Fig 5 a&b (above): typical findings in LUL collapse in a patient with endobronchial carcinoma. PA chest film shows haziness of the left lung, with blurring of the mediastinum (arrows). Visible luftsichel sign (red arrow). Lateral view shows the typical sharply-defined retro-sternal opacity (arrows).
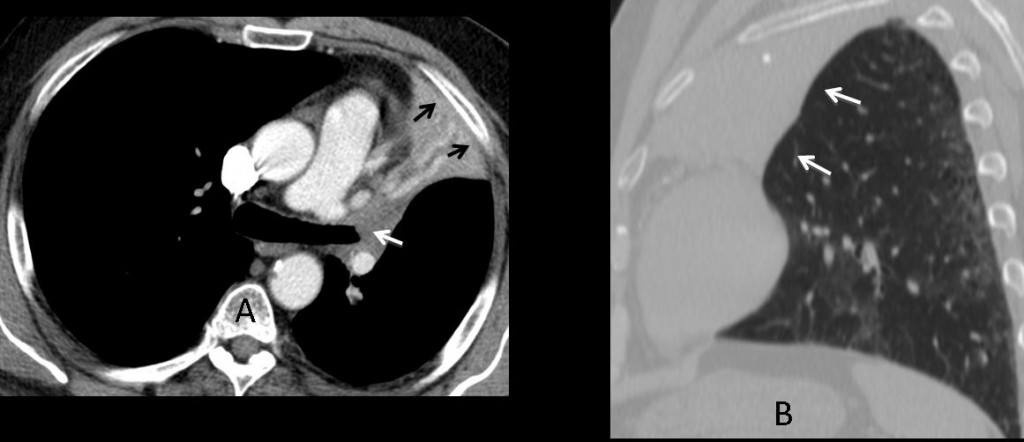
Fig. 6
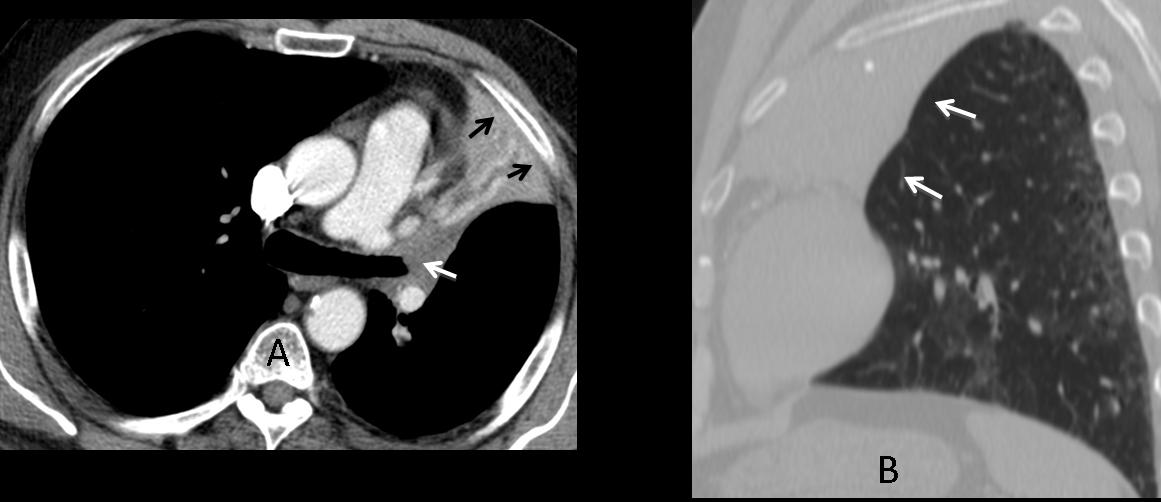
Fig 6 a&b (above): axial CT in the same patient shows the collapsed lobe in apposition to the anterior chest wall (a, arrows) and the endobronchial lesion (b, white arrow). Sagital reconstruction shows the anterior collapse of the lobe (b, arrows).
The most common cause of LUL collapse is a malignant endobronchial lesion, with lung carcinoma as the first possibility. LUL collapse can also be caused by an acute inflammatory disease (Fig. 7), although this etiology is uncommon. Chronic forms of LUL collapse are usually secondary to previous TB (Fig. 8).
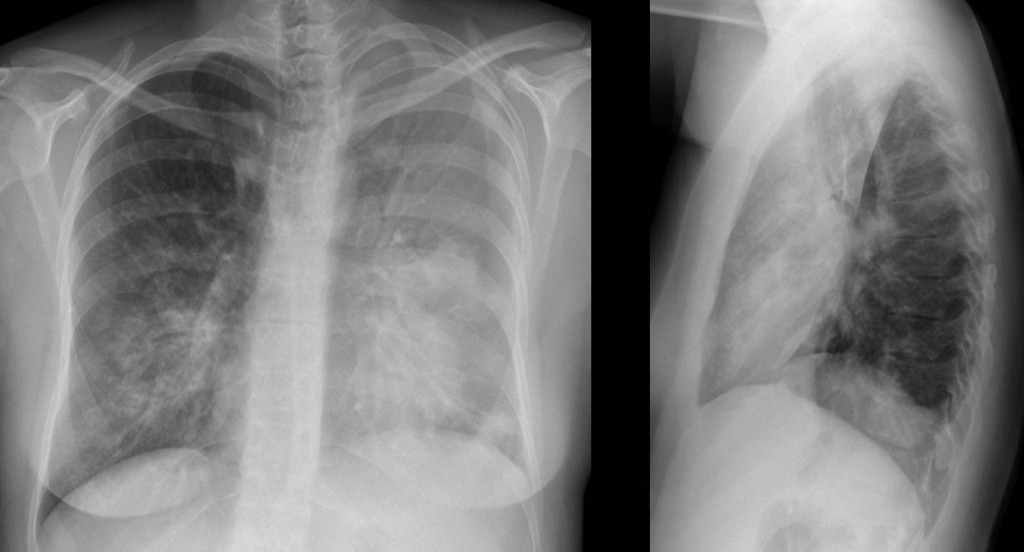
Fig. 7
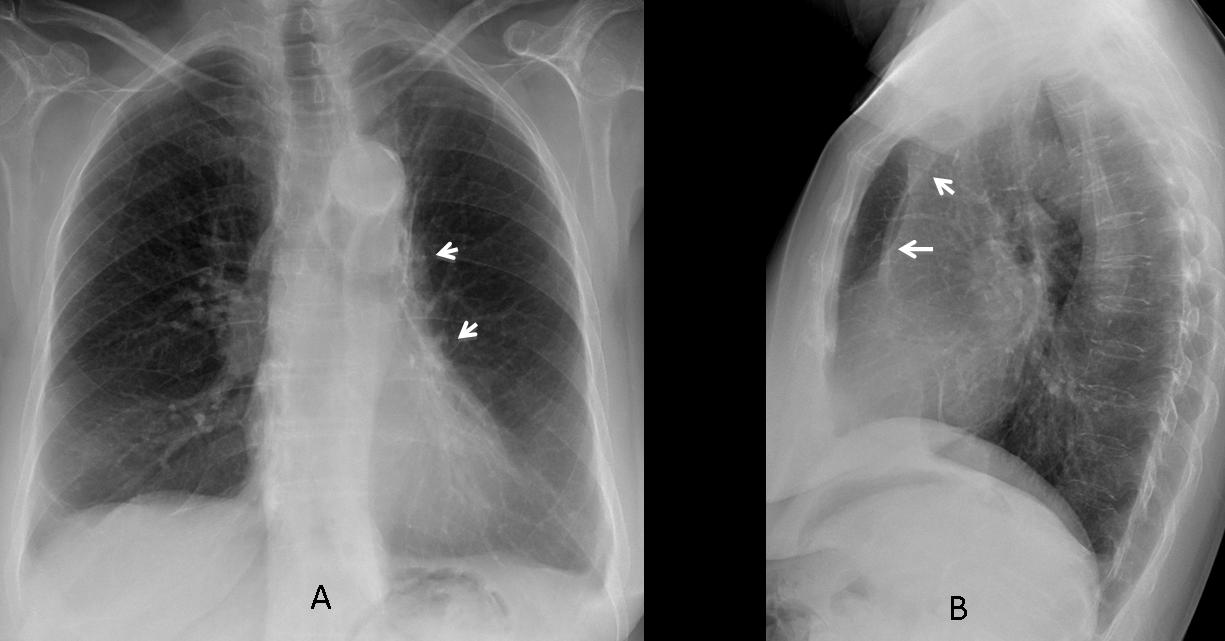
Fig. 7 (above) 47-year-old woman with LUL pneumonia. Findings are very similar to LUL collapse, with haziness of mediastinal and cardiac borders and retrosternal opacity. In cases such as these, an endobronchial lesion should be excluded with CT or bronchoscopy.
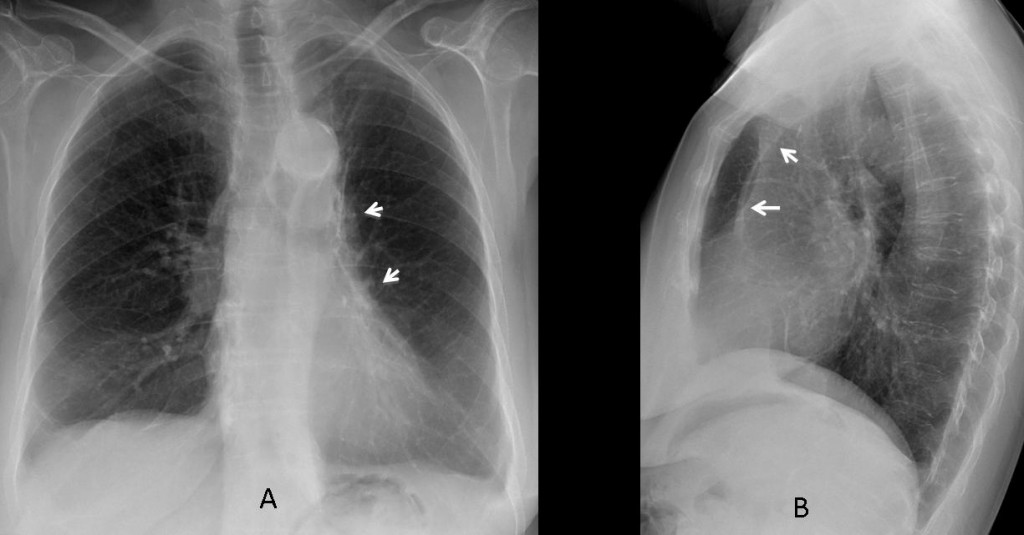
Fig. 8
Fig. 8 a&b. Patient with collapsed LUL secondary to old TB. There is slight tracheal deviation and haziness of the mediastinum in the PA film (arrows). Lateral view shows the retrosternal line (arrows). Air in front of this line is due to anterior herniation of the right lung.
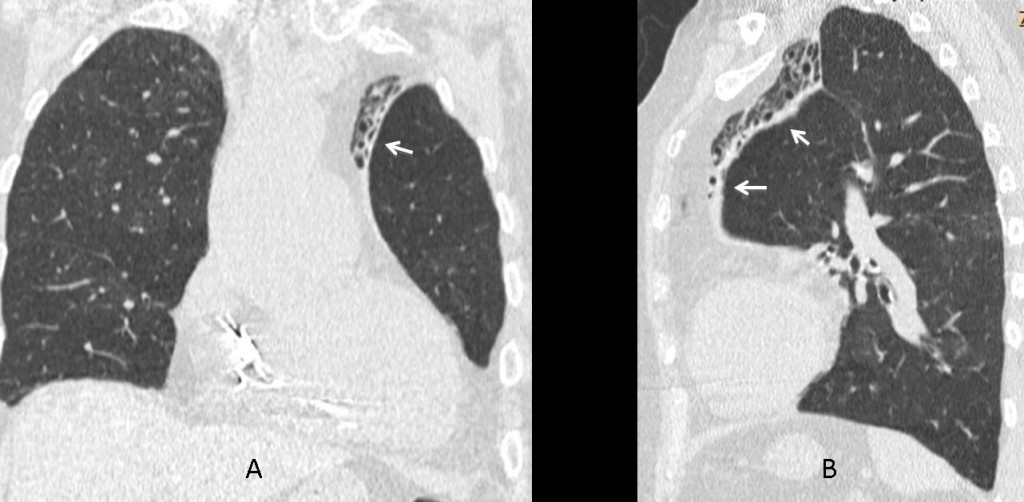
Fig. 9
Fig. 9 a&b (above): coronal and sagittal CT confirm the marked LUL collapse, with good visibility of the retrosternal line in the lateral view (arrows).
Since malignancy is the first cause of LUL collapse, it is important to carefully seek its signs, especially in extreme cases, to avoid a delay in the diagnosis. In marked LUL collapse, the lateral view is very useful, depicting subtle findings that should not be overlooked (Fig. 10).
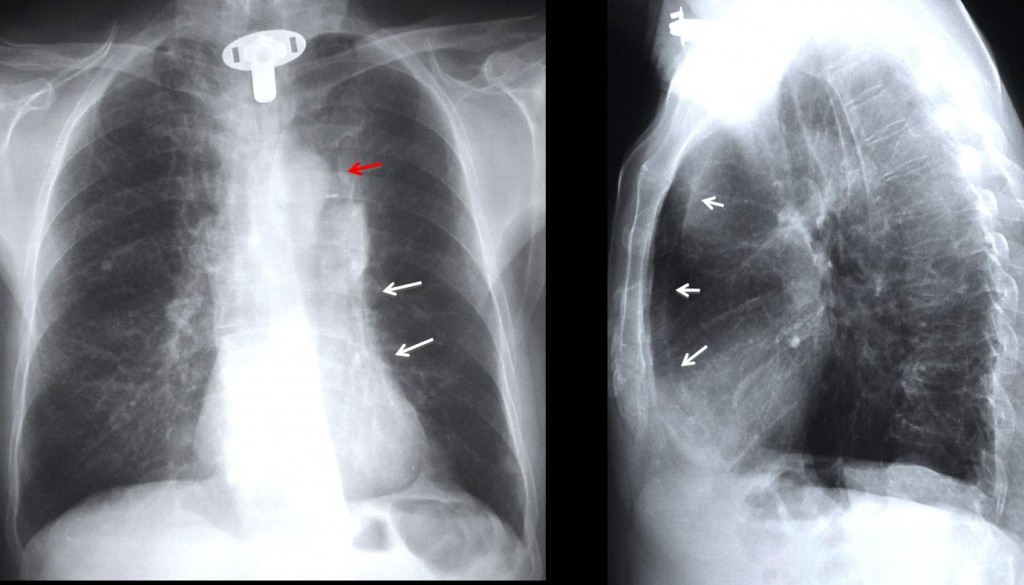
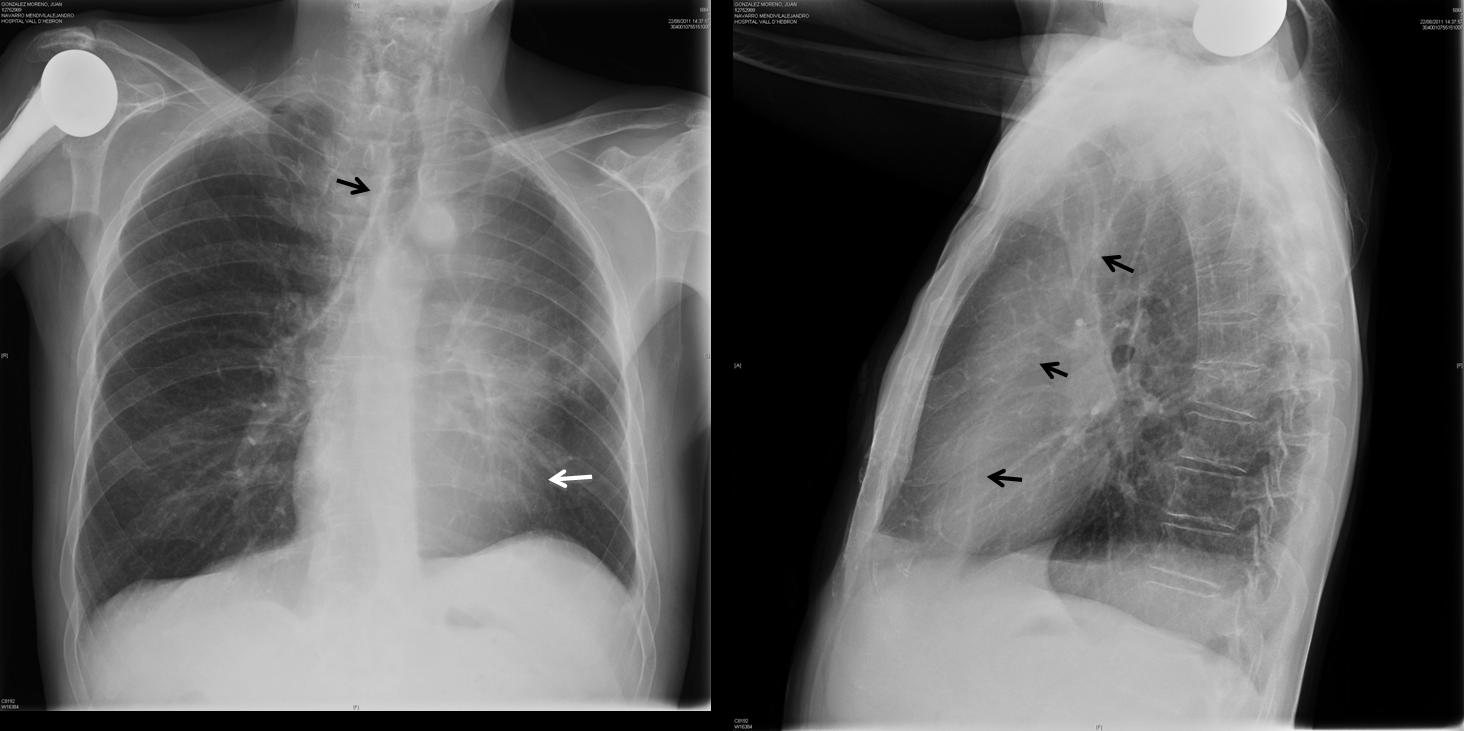
Fig. 10
Fig. 10: subtle findings of extreme LUL collapse in a patient who had undergone surgery 10 years before for carcinoma of the larynx. PA film shows blurring of the mediastinum (arrows) and luftsichel sign (red arrow). The retrosternal line is visible in the lateral view (arrows). Bronchoscopy confirmed the diagnosis of bronchogenic carcinoma.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- In the PA chest film, LUL collapse causes diffuse increased opacity of the left lung, with blurring of the mediastinum and heart border.
- The lateral view is more revealing, showing a sharply defined retrosternal opacity.
- The most common cause of LUL collapse is bronchogenic carcinoma.
Suggested reading: Lobar collapse, basic concepts. European Journal of Radiology 23: 9-22, 1996
Case prepared by Dr. Pepe






left ul atelectasis highly suspicious of carcinoma until proven otherwise
Perdita di volume dell’emitorace sx, ipoespanso, con riduzione degli spai intercostali, attrazione omolaterale dell’ombra cardio-mediastinica, opacità a banda retrosternale, pinzettamento pleurico basale , il tutto come da atetelettasia del bronco lobare superiore sx. Regola KISS : ipotesi piu’ probabile , CR bronchiale.
LUL collapse (atelectasis).
Dense nodular opacity on left paratracheal stripe(left pilmonary artery with left bronchus in upper position?)
Pleural calcification in left (and Right apex) and calcfication also in left middle field.
Bronchial TB(i.e. Broncholithiasis).
it’s a good idea?
Apply the KISS method. It is safer.
I believe this is a case of malignancy that have been left untreated . That fracture ten years ago was pathologic and now there is blured anterior border of T10 vertebra and increased intensity at the left axilliary region, which maybe has to do with the non visualization of the medial part of left scapula. So i will go with thoracic wall malignancy. the finding in the lungs are secondary perhaps due to meta.
Fracture of T-8 was traumatic, with fracture of right humerus as well. It would be unusual for a bone malignancy to last for ten years. I mentioned the previous fracture of T-8 to avoid misleading the readers.
Try again.
elevation of the diaphragm, nodular opacity ..I would go with the TB but CT is needed..
Lung ca
Shift of mediastinum towards left , left hilum enlargement and a pulmonary nodule that maybe have cavity . Reactivation of TB?
There is volume loss on the left as evidenced by loss of the left cardiac border, mediastinal shift to the left, crowding of the left lower ribs and elevation of the left hemi-diaphragm. There is air-space shadowing in the lingula. A calcified lymph node is seen at the level of the carina, which is adjacent to and causing compression of the left main bronchus.
There is loss of height of the T8 vertebral body in keeping with the known old fracture.
I think this is reactivation TB with left bronchial stenosis and mucoid impaction leading to left lung collapse
Caro dr Pepe, il Professor Caceres è più generoso un elogi di te: dimmi che sono stato bravo, anche se il caso era semplice! Con affetto dal Sud Italia.
Yes I believe you are doing very well, both in the diploma and Caceres’ corner. Thinking of giving away T-shirts with Dr. Pepe’s picture to the best achievers. That’s much better than a compliment!
Hello! What’s the KISS method about? 🙂 thank you!