Dr. Pepe’s Diploma Casebook: Case 49 – SOLVED!
Dear Friends,
The first case of 2014 belongs to a 40-year-old male with a mild cough. What would you suspect?
1. Tuberculosis
2. Carcinoma
3. Enlarged left pulmonary artery
4. None of the above
Check out the images below and leave your thoughts and diagnosis in the comments section.


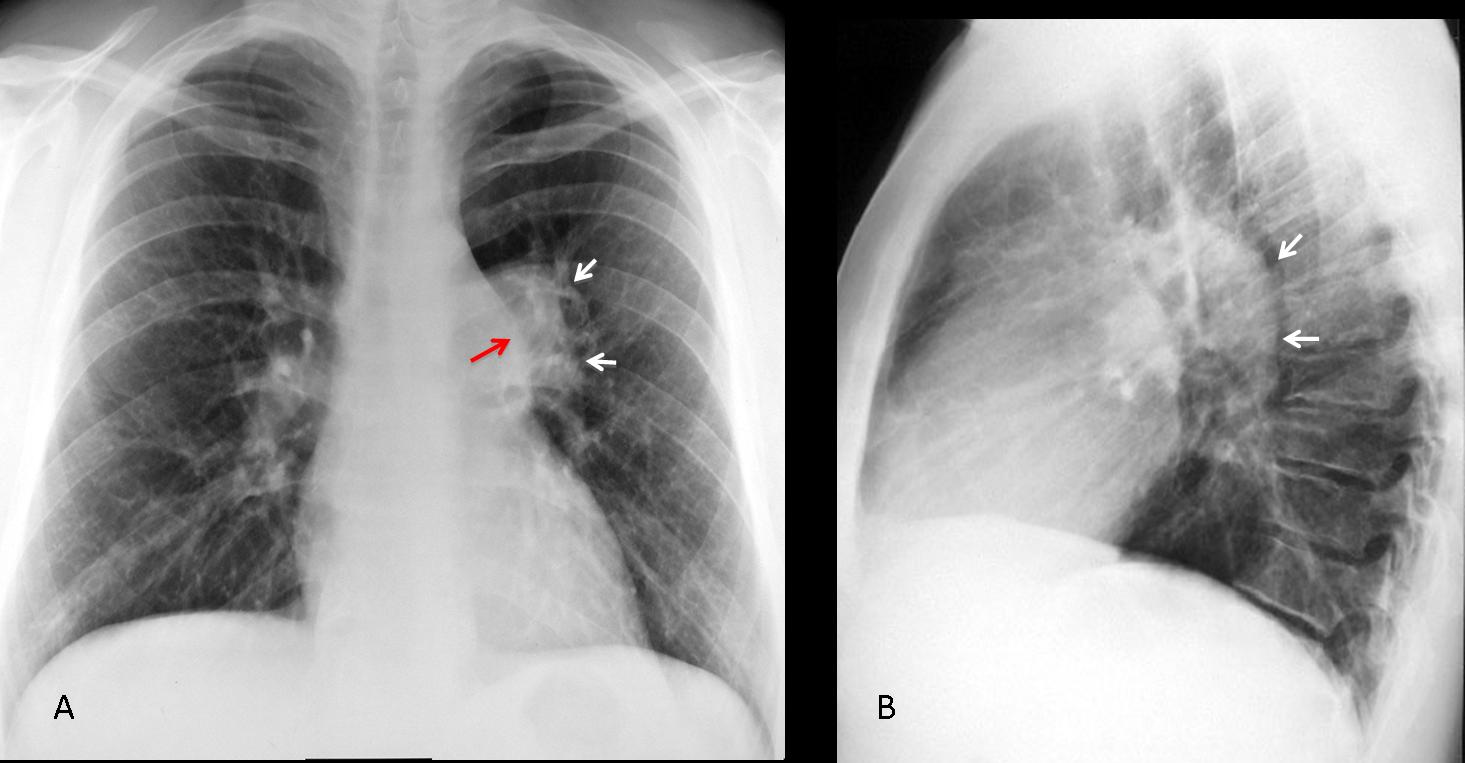
Fig. 1
Findings: the PA view shows that the left hilum is larger and more opaque than the right (A, white arrows). The pulmonary arch is prominent (A, red arrow). The lateral view show an increase in size of the left pulmonary artery (B, arrows). This combination of signs is highly suggestive of pulmonary valve stenosis in which the jet strikes the main pulmonary trunk and left pulmonary artery, enlarging both.
Enhanced CT confirms marked enlargement of the left pulmonary artery (C, arrows).

Fig. 2
Final diagnosis: congenital pulmonary valve stenosis, with secondary enlargement of the left pulmonary artery.
This case is presented to discuss unilateral hilar enlargement. This feature is easily recognisable by comparing the size and opacity of the two hila. In my experience, increased hilar opacity is more reliable than increased size.
Considering that the hila has 3 components ─ the pulmonary artery, bronchi, and minute lymph nodes ─ the possible causes of hilar enlargement are:
1. Enlarged pulmonary artery (A)
2. Bronchogenic carcinoma (B)
3. Lymphadenopathy (C)
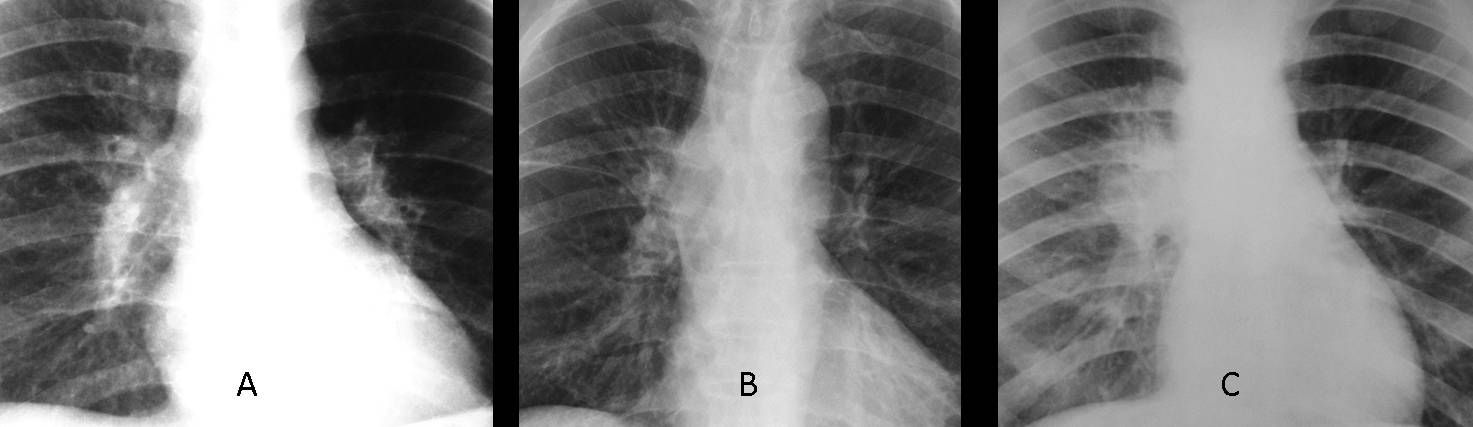
Fig. 3
Before discussing hilar pathology, we should review the normal hilar anatomy. In the PA view, the right and left pulmonary hila include the right and left main pulmonary arteries, respectively.

Fig. 4
In the lateral view, the right main pulmonary artery appears as a nodular shadow (Fig. 4 A,B, white arrow) in front of the trachea (T), whereas the left main pulmonary artery has the shape of a comma behind the posterior tracheal wall (Fig. 4 A,B, red arrow). Thus, an enlarged artery is easily recognisable in the lateral film, as in the initial case presented. When a solid mass is present, the hilar components are ill-defined (Fig. 4 C, arrows).
A word of caution: if the lateral view is not straight, normal hilar anatomy may not be recognisable. In case of doubt, always perform an enhanced CT.
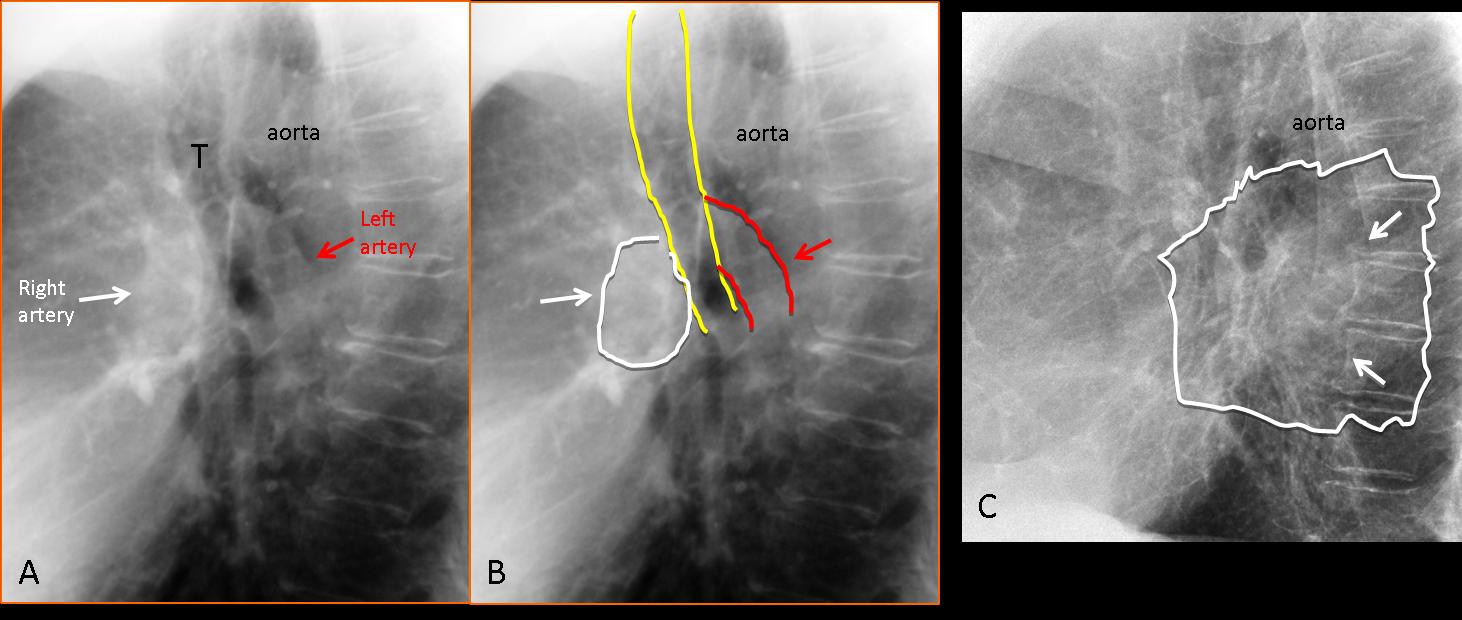
Fig. 5
TIP: the enlarged/dense hilum is identified in the PA view. The lateral view is useful to determine if the cause is an enlarged artery or a mass.
Congenital pulmonary valve stenosis is an unusual cause of hilar enlargement and affects only the left hilum. Another cause of vascular hilar enlargement is central pulmonary embolism. The embolus lodged in the central artery causes an increase in size and opacity of the hilum and may affect either one (Fig. 6).
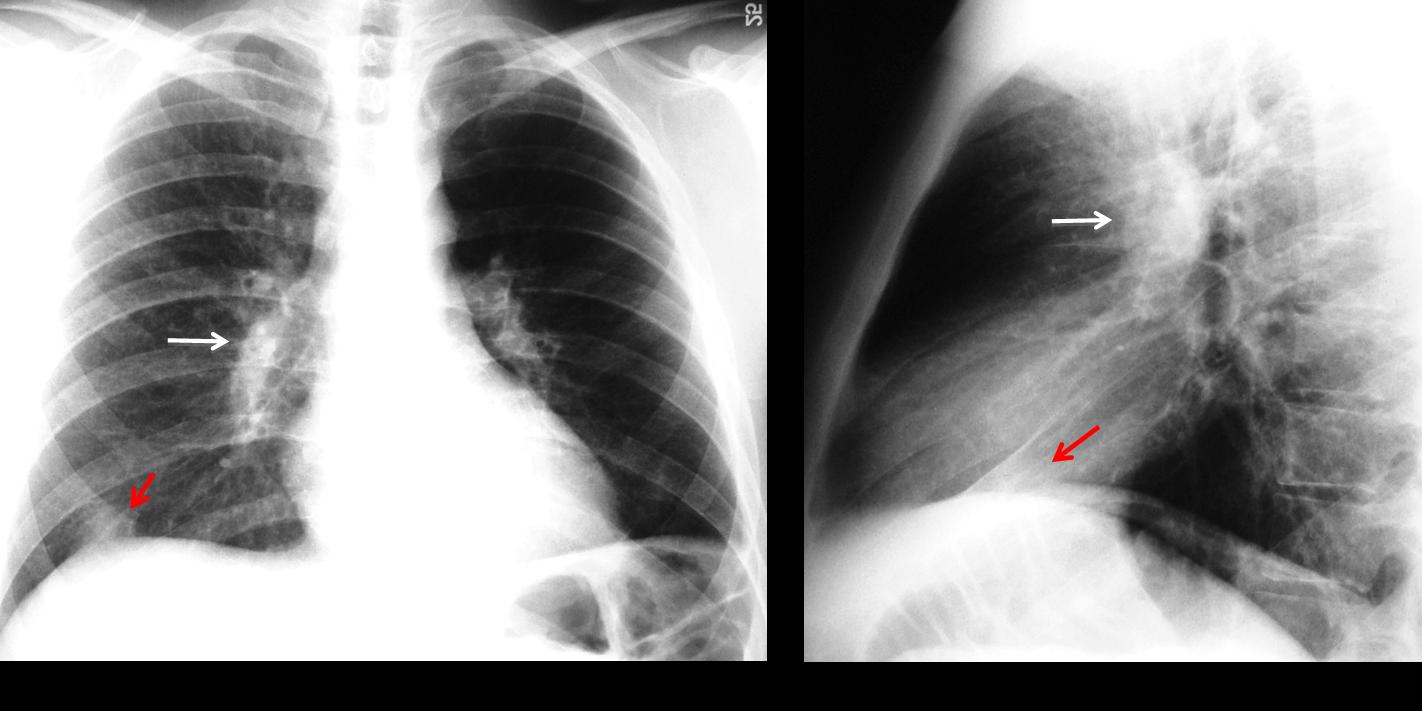
Fig. 6
Fig. 6 (above): 23-year-old diabetic man with pulmonary embolism. Note the enlarged right hilum in the PA and lateral view (white arrows). Pleural-based opacity at the right lung base (red arrows) typical of a Hampton hump.
In pulmonary embolism, when the anatomic contour of the hilum is not well defined, enhanced CT is needed to differentiate embolism from a hilar mass (Fig. 7).

Fig. 7
Fig. 7 (above): 47-year-old male with hypernephroma and abnormal right hilum (A, arrow). Metastases were suspected. Standard enhanced CT shows a central embolus in the right pulmonary artery (B, arrow).
Solid lesions, such as bronchogenic carcinoma or lymphadenopathy, are by far the most common cause of unilateral hilar enlargement. It is difficult to differentiate between these conditions, and enhanced CT should always be performed (Figs. 8 and 9).

Fig. 8
Fig. 8 (above): increased opacity of a normal-sized left hilum (A, arrow). Lateral view shows a normal left pulmonary artery (B, white arrow) and an anterior, rounded mass (B, red arrow). CT confirms a lung mass in the left hilum (C, arrow). Diagnosis: bronchogenic carcinoma.
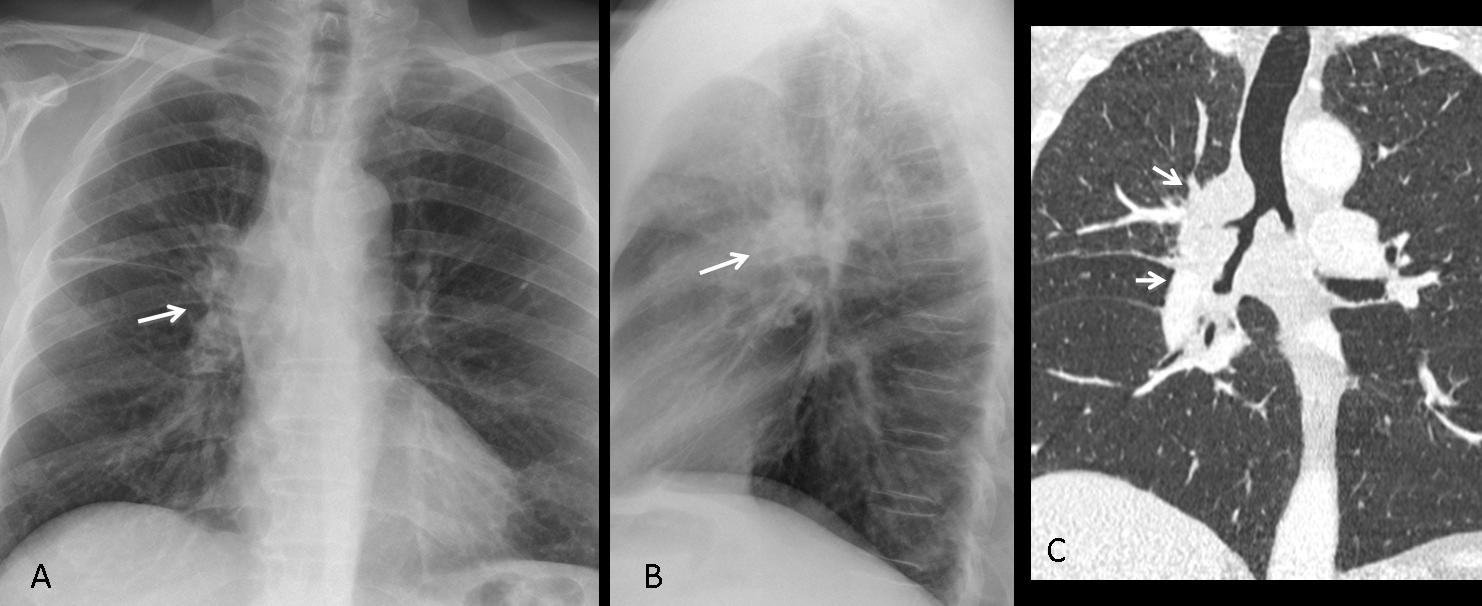
Fig. 9
Fig. 9 (above): abnormal right hilum, which is enlarged and increased in opacity compared to the left one (A, B, arrows). Coronal CT shows a large hilar mass narrowing the bronchi (C, arrows). Diagnosis: central bronchogenic carcinoma.
Lymphadenopathy is another cause of unilateral enlarged hilum. The most common origin is metastasis from bronchogenic carcinoma (Fig. 10), with tuberculosis as a distant second (Figs. 11 and 12).
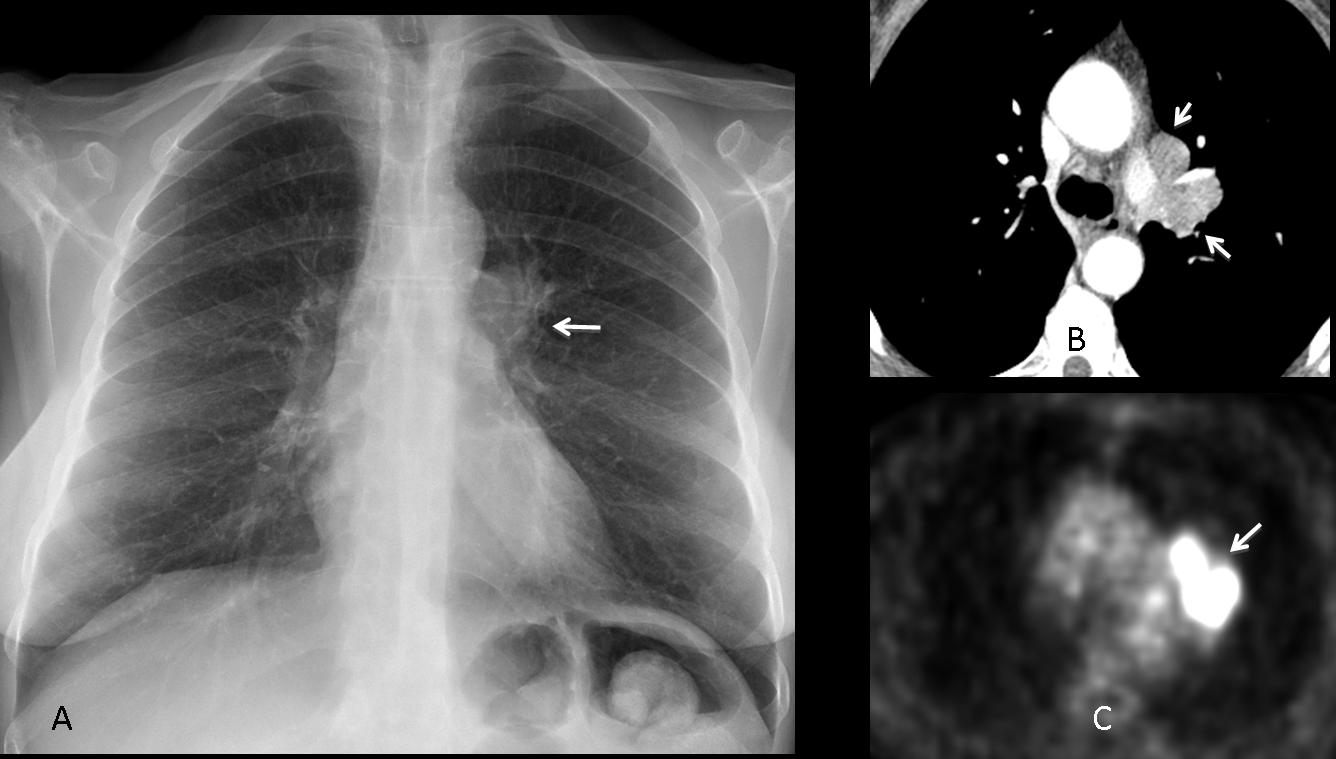
Fig. 10
Fig. 10 (above): 61-year-old woman with prominent left hilum (A, arrow). Axial CT shows enlarged lymph nodes (B, arrows) with high metabolic rate on PET (C, arrow): Small-cell carcinoma.
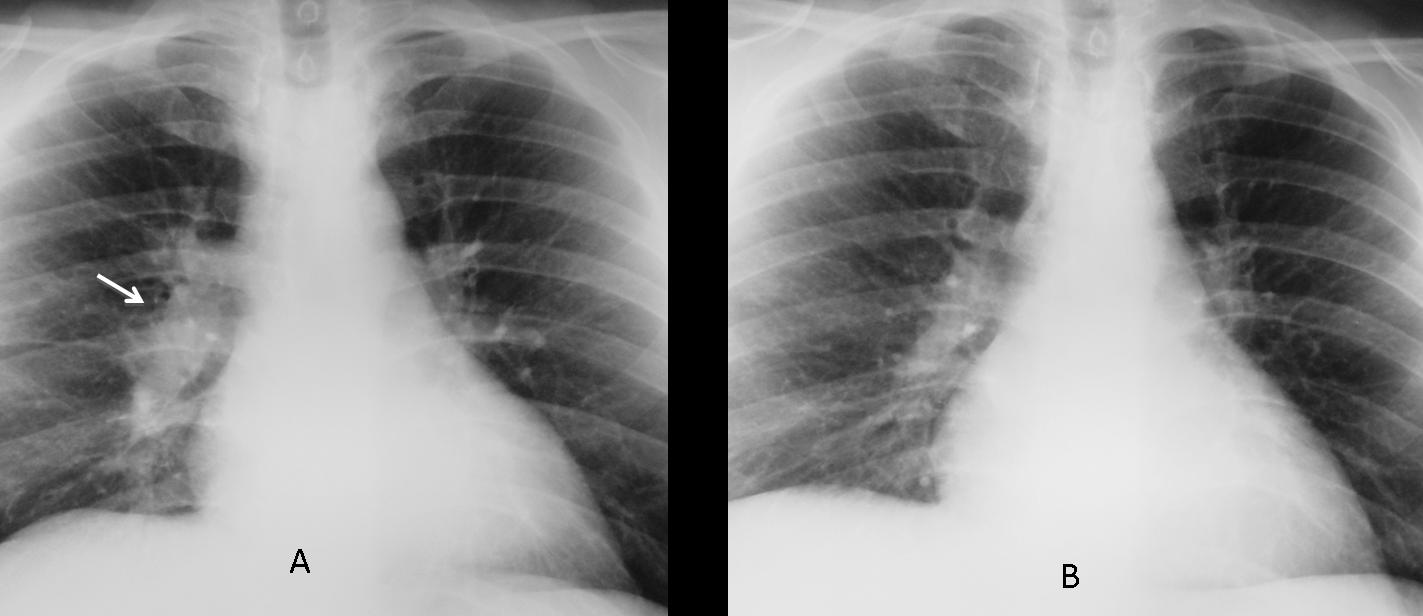
Fig. 11
Fig. 11 (above): 35-year-old man with unilateral enlargement of right hilum secondary to tuberculous lymphadenopathy (A, arrow). Radiograph after treatment (B) shows decreased size and density of the right hilum.
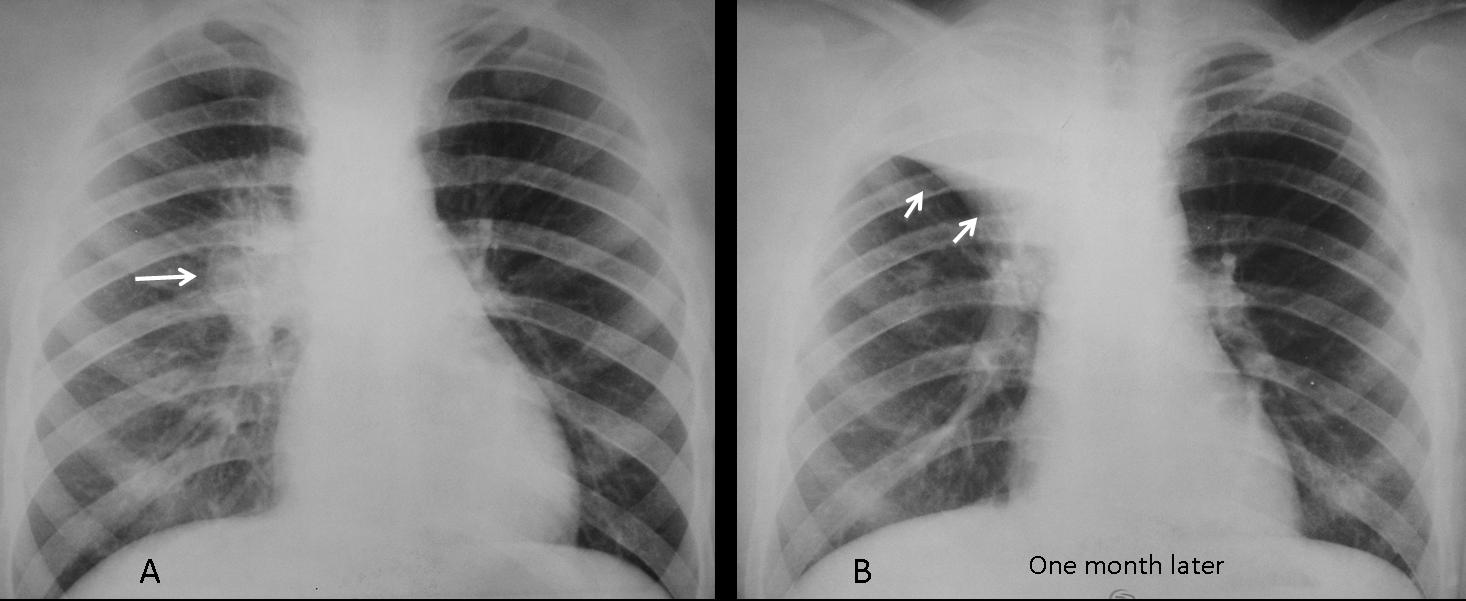
Fig. 12
Fig. 12 (above): 16-year-old male with tuberculous lymphadenopathy of the right hilum (A, arrow). One month later, the enlarged lymph nodes have caused RUL collapse (B, arrows).
Time for a test. The radiographs below are of a 49-year-old male, smoker, with fever. Diagnosis:
1. Carcinoma
2. TB
3. Lymphadenopathy
4. None of the above
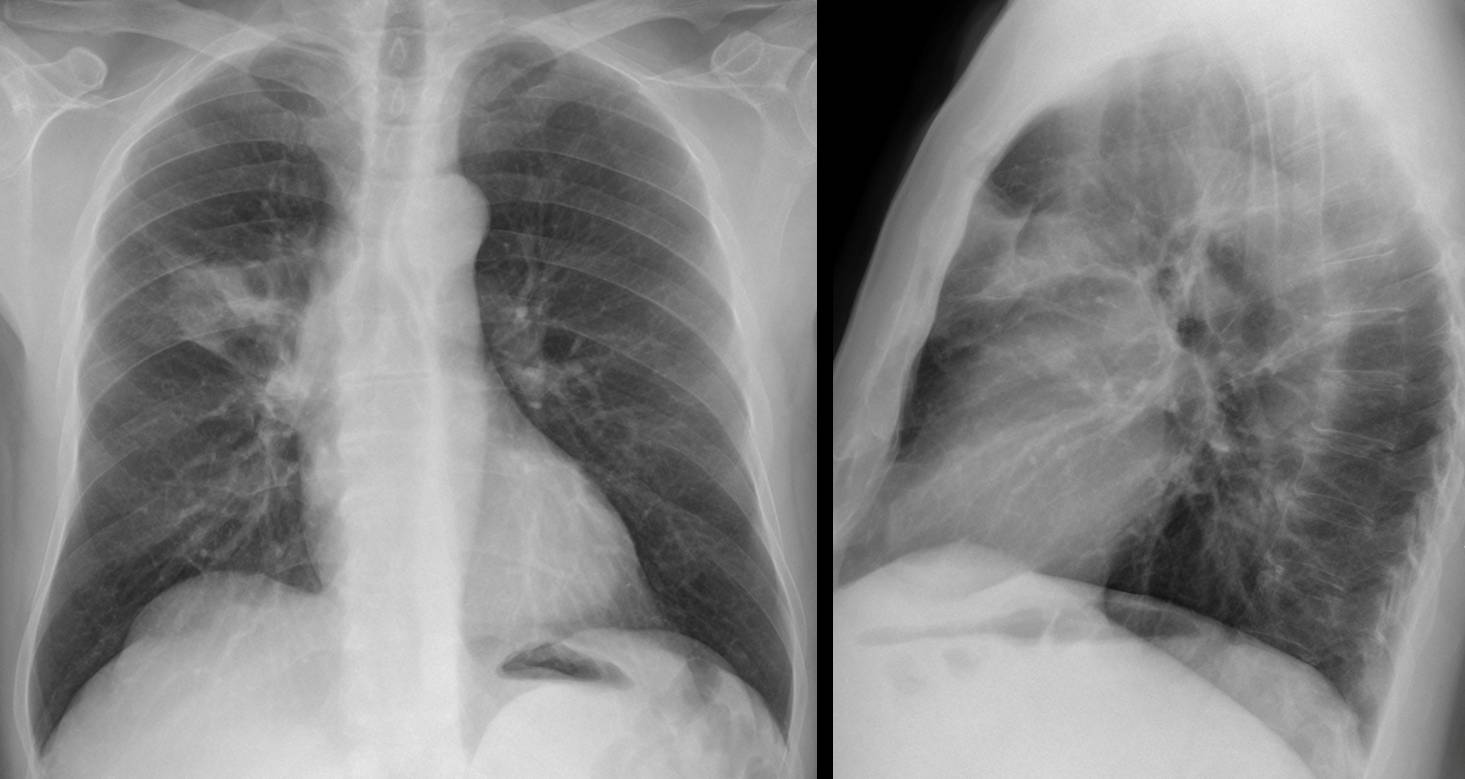
Fig. 13
Aside from the already mentioned causes of enlarged hilum, there is a spurious one caused by superimposition of a pulmonary lesion. Any process in front of or behind the hilum (tumor, infection, etc.) may simulate a dense hilum. In this particular case there is a pneumonic infiltrate in the anterior RUL, simulating a dense right hilum (Fig. 14 A, arrows). The lateral view shows the anterior pneumonia (B, white arrow) and the intact hilum (B, red arrow).
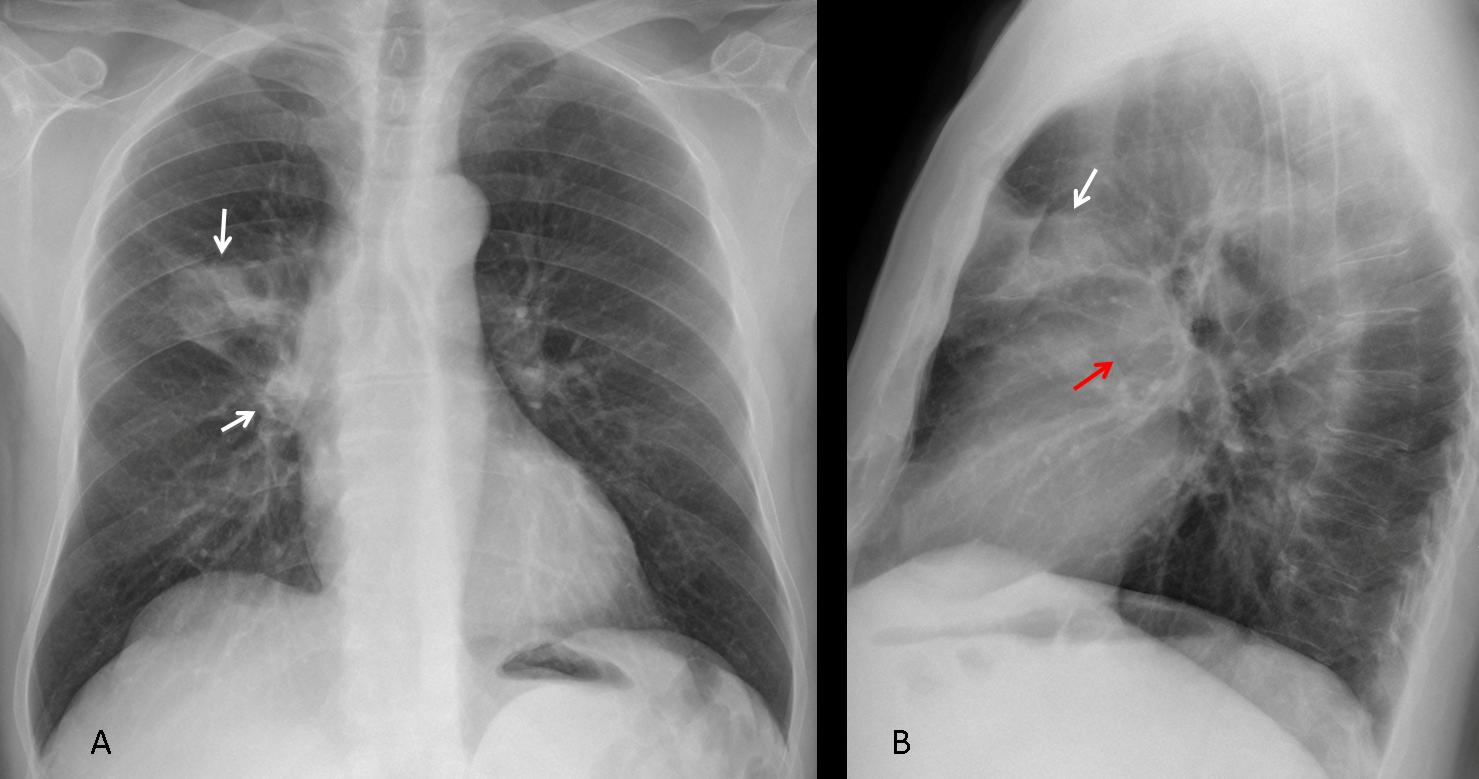
Fig. 14
Another example, in which a peripheral nodule in the apical segment of the LLL simulates a dense left hilum (Fig. 15). This case emphasises the importance of obtaining a lateral radiograph to better evaluate possible hilar disease.
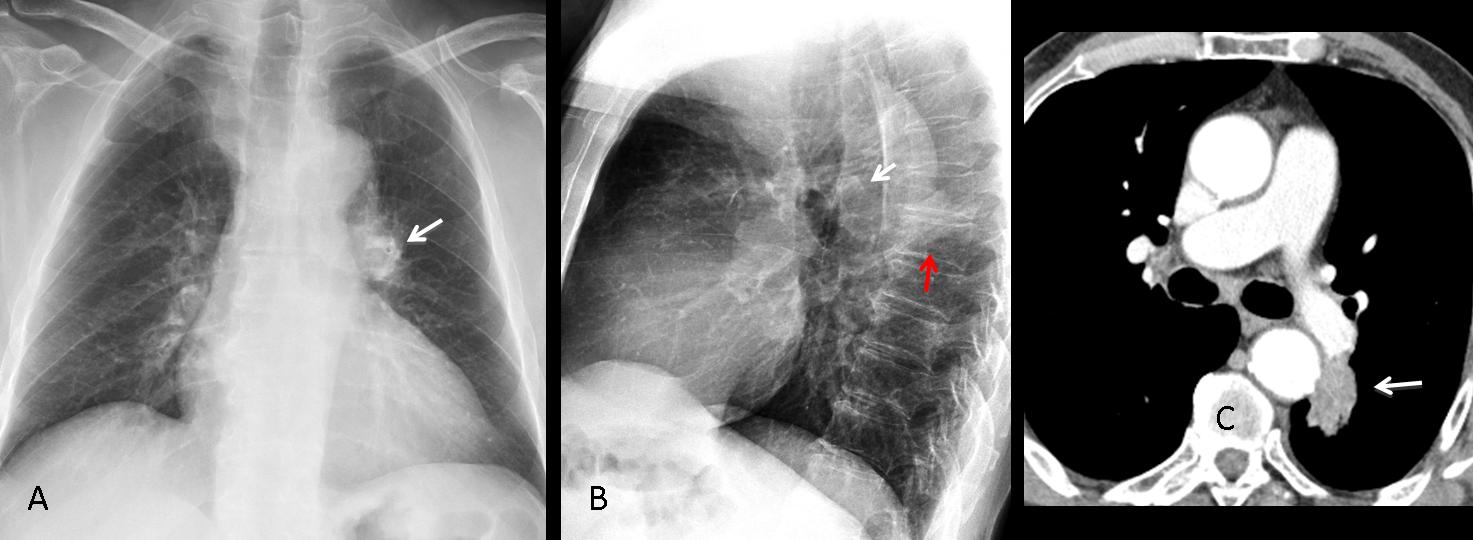
Fig. 15
Fig. 15. PA chest film shows an apparently dense left hilum (A, arrow). Lateral view shows a normal left hilum (B, white arrow) and a pulmonary nodule projected over the spine (B, red arrow). CT confirms the absence of hilar disease and the pulmonary nodule (C, arrow): bronchogenic carcinoma.
For completeness’ sake, I should mention increased density of the left hilum by a superimposed elongated aorta (Fig. 16, arrow). This is a common mistake of first-year residents.
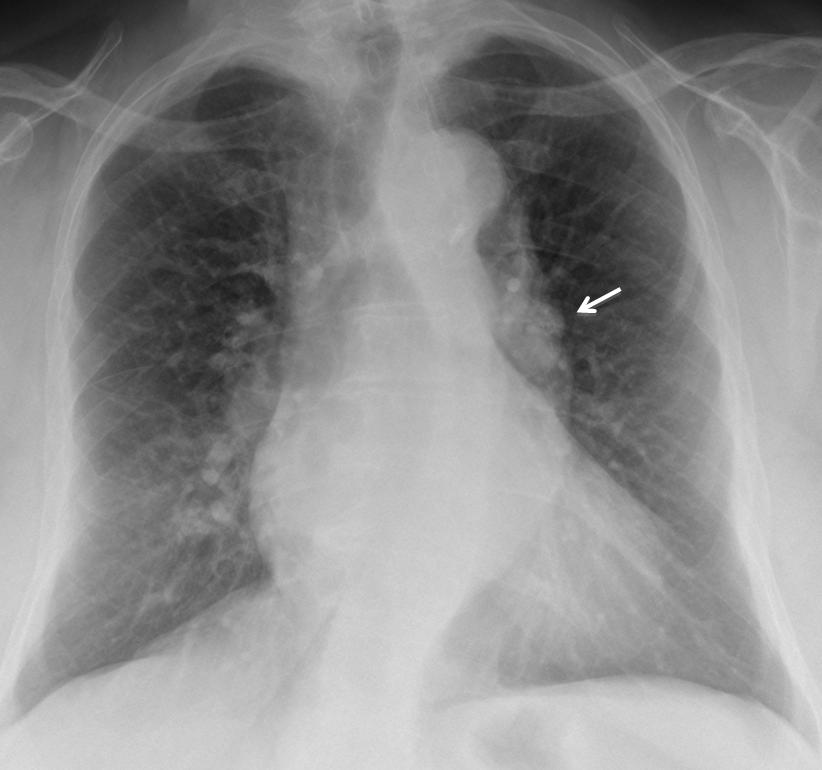
Fig. 16

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Bonchogenic carcinoma is the most common cause of unilateral enlarged hilum
- Occasionally it may be due to TB lymph nodes or an enlarged pulmonary artery
- The lateral view helps to identify enlarged pulmonary arteries
- The lateral view identifies superimposed lung processes that simulate an enlarged hilum in the PA view


There is an unilateral left-sided mass in a hillum. In the differential diagnosis sign is characteristic for carcinoma. It’s margine is rather ill-defined which excludes left pulmonary artery enlargement. Upper zones billaterally and right paratracheal region seems to be unaffected which excludes TB.
Left side hilar ill-defined irregular mass. DDx includes malignant lesion vs lymphadenopathy.
And?
None of the above
Carcinoma
there is mass in the left hilum – carcinoma?
There`s a heterogenous mass in the left hilum with ill defineg borders and border calcifications – in lateral image looks like it`s in the posterior mediastinum. The upper segments of LUL are translucent which indicates the dmimisied vascularization. I`d vote for enlarged left pulmonary artery and because of calcifications I`d think about aneurysm. Or maby if the clinical signs are acute we should exclude pulmonar emboli?
Nice discussion. Sorry, no calcium was present. And symptoms were minimal.
Still, you are close.
A left hilar homogenous opacity of irregular outlines, shows some areas of marginal spiculation and definitely attenuates the lumen of the main left upper lobe bronchus (( bronchogenic carcinoma )) is highly considered
No trachea or intralobular fissure participation, so carcinoma is excluded. lymph node enlarged vs left pulm.art.dilatation. None of the above though
Is it too much to ask for a ct scan :]
Patient’s age, symptoms and x-rays are not characteristic.
I would consider ans. 3, although carcinoma (or metastatic lymph node) can’t be excluded.
Who would state a diagnosis in this case, based on x-ray, without a ct?
I don’t expect anyone, including me, to make a diagnosis based only in plain radiographs. But a correct interpretation of the findings helps. In this particular case, the enlargement of the left pulmonary artery on the lateral view excludes carcinoma and TB.
i am not sure if that we see is carcinoma.
i can see prominent pulmonary outflow tract on frontal view and enlarged both pulmonary arteries on the lateral view. The peripheral pulmonary arteries are normal in size.
i can’t se well the aortic knob.
Patent ductus arteriosus ?
no!
descending aortic arch saccular aneurism.
It’s a hilar mass and it kind of reminds of an enlarged vessel on the lateral xray. Proposed ddx : pulmonary artery aneurysm, lymphadenopathy, ca.
the aorta is rather small. must be some sort of a congenital vascular malformation.
poststenotic dilatation of the left pulmonary artery after chronic pulmonary embolism?
There are other causes of dilatation of left pulmonary artery. Look them up.
1. Can bronchoscope
2. Lymphadenopathy
3. Duplication / bronchgenic cyst
Advise:CECT Chest
….la “massa” sembra di “natura” vascolare, presentando delle diramazioni vascolari sul suo contorno.Non puo’ essere TBC perché la TBC è post-primaria in età adulto e dunque dovrebbe presentare un quadro di interessamento parenchimale.Non può essere un tumore ilare perché l’aspetto dei margini è abbastanza regolare e non vi sono turbe di ventilazione polmonare.Resta l’ipotesi di una natura vascolare unilaterale, si esclude pertanto l’ipertensione polmonare, primitiva e-o secondaria.Rimane una ectasia aneurismatica probabilmente esito vasculitico(Becet?).Dirimente ovviamente l’angio-tc con le varie ricostruzioni.
i vote for enlargement of left pulmonary artery because on profile image the main bronchus is well expanded (no retraction or obstruction). But i guess there is a valvular mechanism of air entrapment more peripherally. Arteritis could be the cause.
I agree with you, although the interpretation is simpler: the left artery is enlarged in the lateral view.
CT on Friday.
Would like to congratulate all of you that made the diagnosis of enlarged left pulmonary artery. Answer and discussion tomorrow.
Have a nice weekend!
…..grazie dott. Pepe….avevo pensato ANCHE ad una patologia congenita vascolare, ma l’età del paziente e la mancanza di segni cardiologici per esempio alla semplice AUSCULTAZIONE, del cuore mi avevano fatto propendere per una origine “acquisita” di tale patologia.Grazie ancora per la lezione!
Grazie, dottore
Nice case
My discussion is different, do we need to do lateral chest on such patients? No matter your interpretation is is the referring doctor always wants CT chest to confirm the lesions, are going back to lateral CXR’s era again? Once you offer a lateral CXR , the referring doctors particularly junior doctors will request lateral CXR on all patients– increased workload and increased radiation!!