Dr. Pepe’s Diploma Casebook: Case 53 – SOLVED!
Dear Friends,
Today I am presenting radiographs of a 36-year-old woman with shortness of breath increasing over the last three months. Examine the image below and leave me your thoughts and diagnosis in the comments. Come back on Friday for the answer.
Diagnosis:
1. Metastatic disease
2. Sarcoid
3. Interstitial pneumonia
4. None of the above

36-year-old woman with shortness of breath
Findings: chest radiographs show widespread involvement of the lung with numerous Kerley B lines in both lower lobes (Fig. 1 A, B arrows), confirmed with CT (Fig. 1 C, arrows). In the presence of widespread Kerley lines in a chronic setting, the first consideration should be lymphangitic metastasis to the lung. In this patient, endoscopy discovered an advanced carcinoma of the stomach.
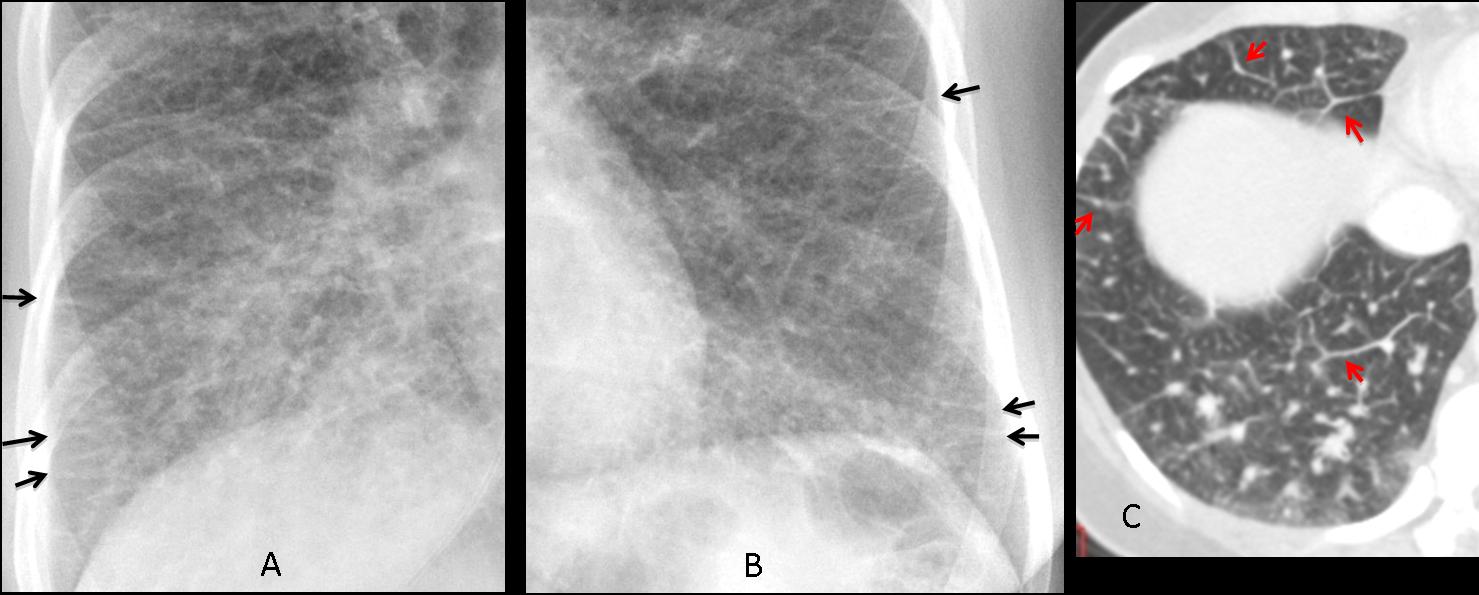
Fig. 1
Final diagnosis: carcinoma of the stomach with lymphangitic lung metastasis.
This case is presented to discuss Kerley lines. This finding is important because their discovery considerably narrows the differential diagnosis of pulmonary processes affecting the interstitium.
From a practical approach, Kerley lines can be classified as A and B. Kerley A lines are thin and non-branching, radiate from the hila, and are better seen in the middle lung areas in the PA view and in the anterior clear space in the lateral view (Fig. 2 A, arrows). Kerley B lines are short and horizontal, and are better seen in the periphery of the lung bases at the costophrenic angles (Fig. 2 B, arrows). A and B lines are equally significant, but B lines are easier to identify. A lines are nearly always accompanied by B lines.

Fig. 2
Fig. 2 (above): a 37-year-old woman with vasculitis. Prominent Kerley A lines are seen in the anterior clear space in the lateral view (A, arrows). PA view shows multiple Kerley B lines, particularly in the costophrenic angle (B, arrows).
Prominent lymphatic vessels and thickened interlobular septa are the anatomic substrata of Kerley lines. CT identifies them much better than plain radiographs (Fig. 3).
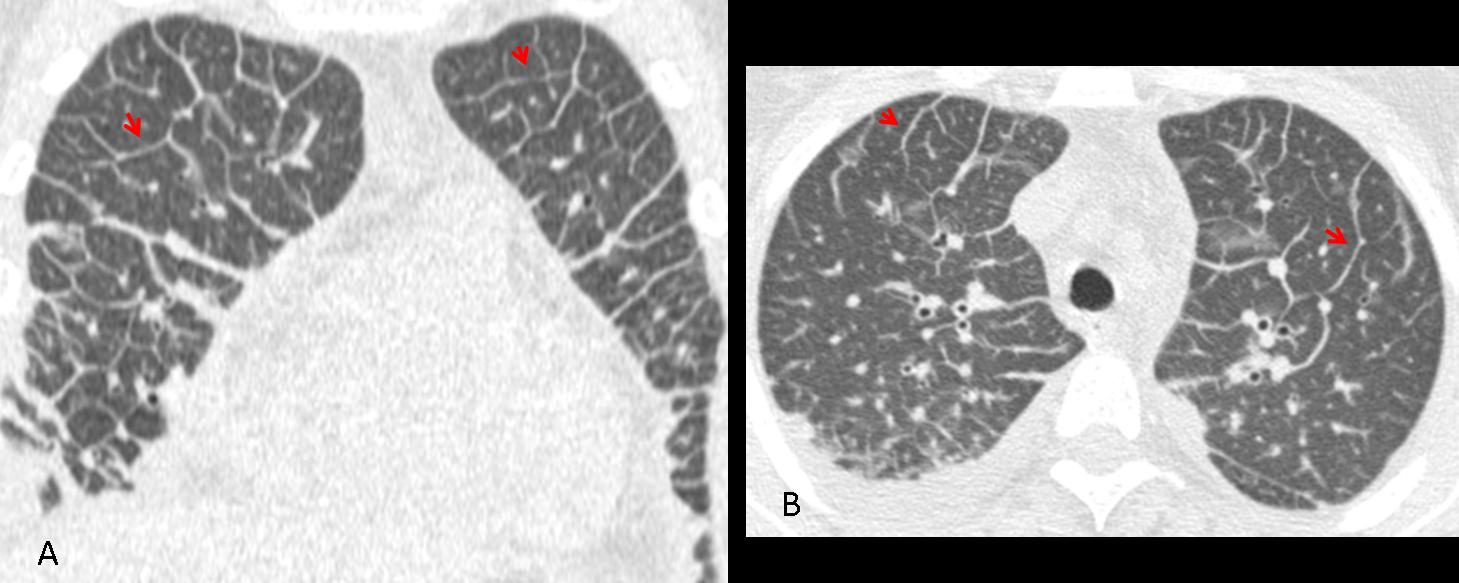
Fig. 3
Fig. 3 (above): CT images of the same patient show the prominent septa to better advantage (A,B, arrows).
From the diagnostic viewpoint, Kerley lines can be classified as transient or persistent. It is important to know that this distinction cannot be made with a single study. Follow-up films or clinical information (acute vs. chronic) are needed. The main characteristic of transient Kerley lines is that they disappear on follow-up studies (Fig. 4).

Fig, 4
Fig. 4 (above): a 47-year-old patient with heart failure. Initial film shows a prominent hilum and Kerley B lines (A, arrows). After treatment, the B lines are less conspicuous (B).
Pulmonary oedema of any etiology (Fig. 5) is the most common cause of transient Kerley lines. Less common ones are vasculitis, allergic reactions, and initial stages of viral pneumonia (Fig. 6).
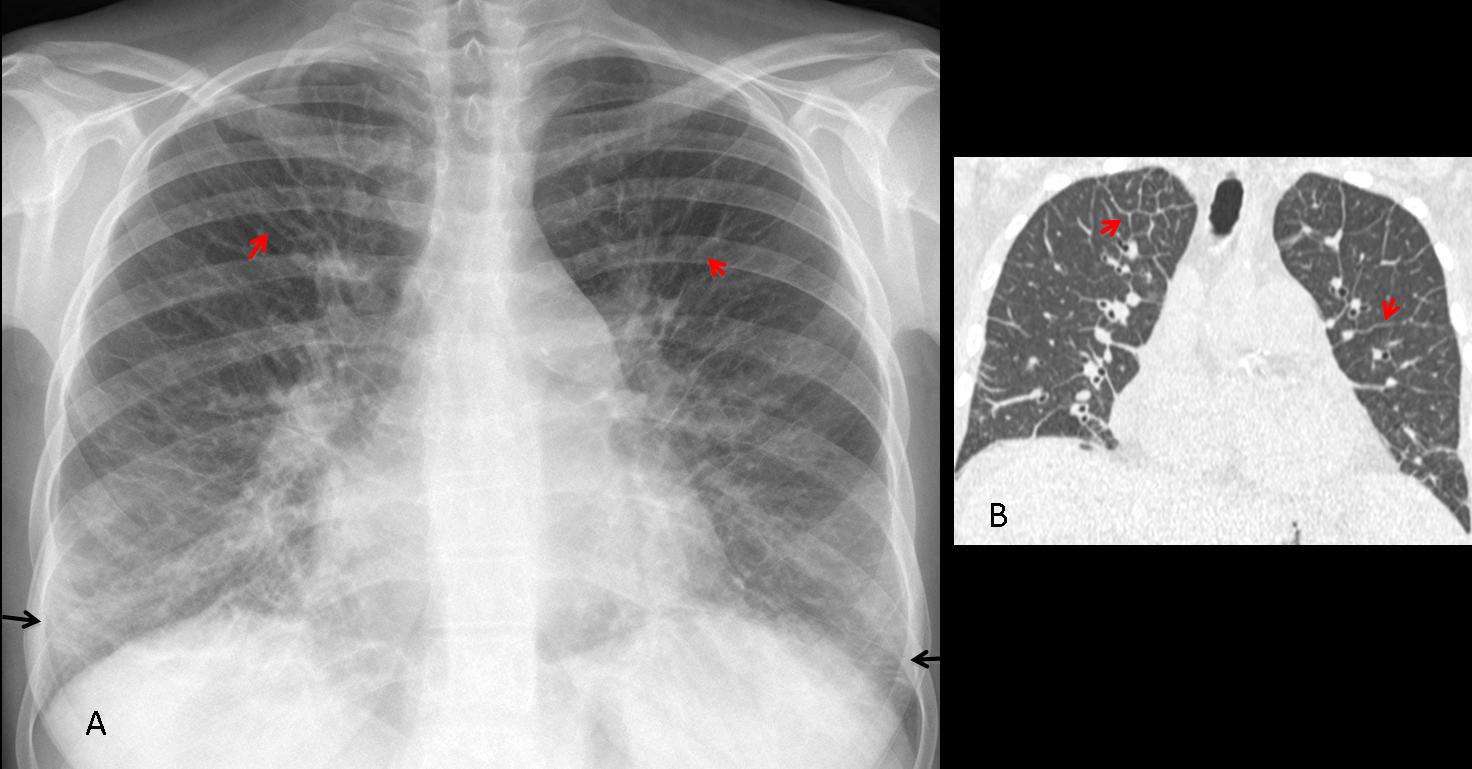
Fig. 5
Fig. 5 (above): 58-year-old man with cardiac pulmonary oedema. PA chest film (A) shows numerous A lines (red arrows) and B lines (black arrows), confirmed with CT (B, arrows). Compare with the initial case of lymphagitic carcinomatosis and notice that the appearance is identical. To differentiate between them we need clinical information or serial films.
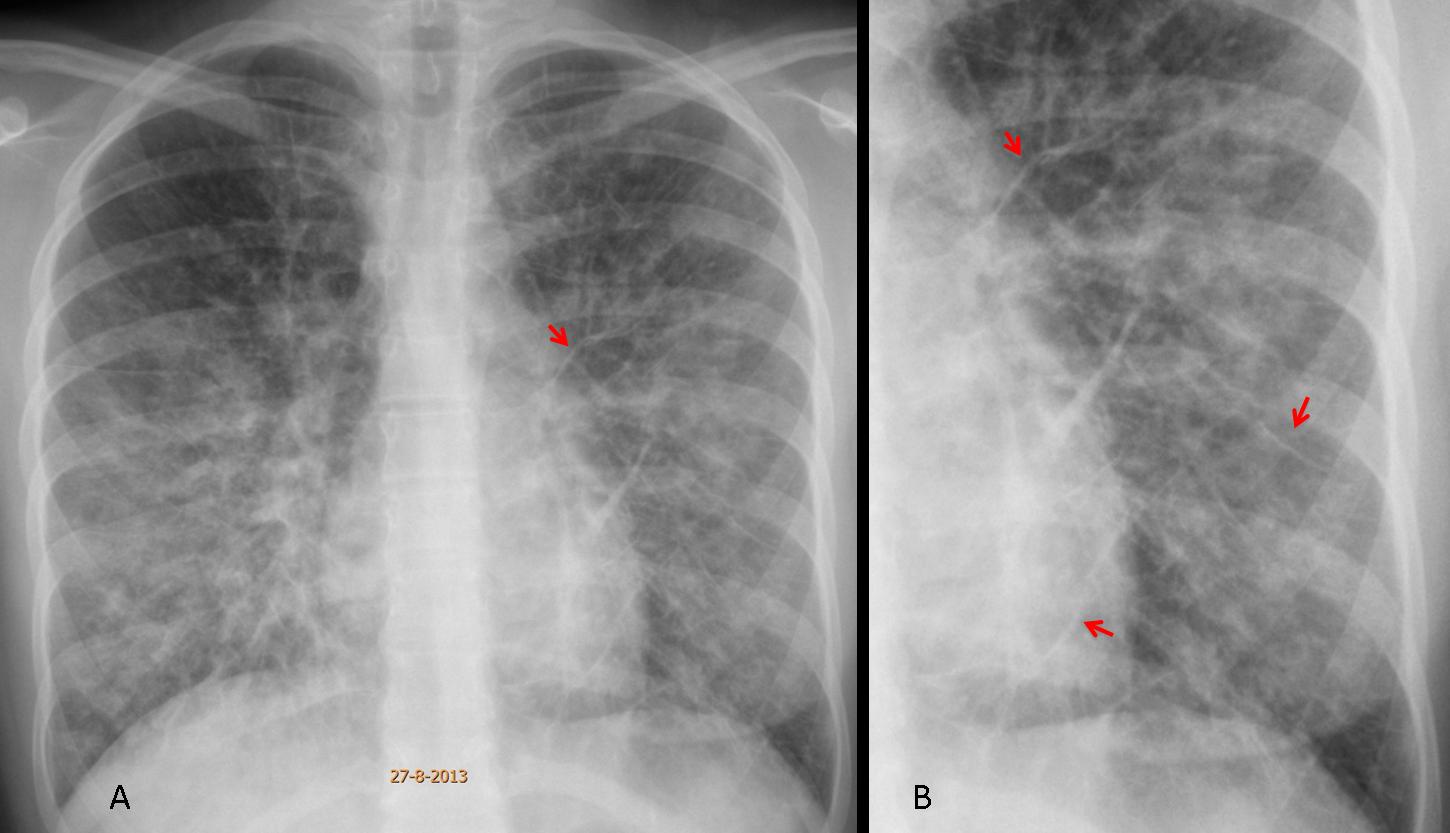
Fig. 6
Fig. 6 (above): 16-year-old girl with viral pneumonia. Notice the widespread air-space disease with prominent A lines (A, arrows), better seen in the close-up view (B, arrows).
Persistent Kerley lines are almost always due to lymphangitic metastasis secondary to the arrival of hematogenous tumour emboli to distal arterial branches and subsequent spread along the pulmonary lymphatics. Any tumour can cause lymphangitic metastasis, but the most common are lung and breast (usually unilateral) (Fig. 7) and GI malignancies: stomach, pancreas, and colon (usually bilateral) (Fig. 8).

Fig. 7
Fig. 7 (above): 41-year-old man with carcinoma of the lung. PA chest film shows an infiltrate along the right mediastinal border, with A lines better seen in the insert (B, arrows). Coronal and axial CT confirm paramediastinal spread of the tumour and septal thickening (C,D, arrows).

Fig. 8
Fig. 8 (above): 57-year-old woman with progressive dyspnea. PA chest film shows widespread Kerley lines (A, arrows), confirmed with CT ( B, arrows). Further studies demonstrated a carcinoma of the colon.
Aside from lymphangitic carcinomatosis, chronic interstitial lung disease may show Kerley lines, although they are not the relevant imaging finding (Fig. 9). Formerly, mitral disease was a classic exponent of Kerley B lines, but nowadays mitral disease is rarely seen in developed countries.

Fig. 9
Fig. 9 (above): 32-year-old man with lupus and interstitial lung disease (A). There are a few Kerley B lines at the left costophrenic angle (B, arrows).

Follow Dr. Pepe’s advice:
1. Kerley lines can be classified as transient or persistent.
2. To differentiate transient Kerley lines from persistent ones, we need serial studies or correlation with clinical findings (acute vs. chronic).
3. The most common cause of transient Kerley lines is pulmonary edema of any cause.
4. The most common cause of persistent Kerley lines is lymphangitic carcinomatosis.


the Kerley-lines suggest either pulmonary congestion, or lymphangitic carcinomatosis.
Due to the normal configuration of the heart and lack of apparent pleural fluid, it’s probably lymphangitic carcinomatosis.
I agree with gaborini(breast ca?)
i can’t see osseous metastasis.
That i can’t understand is where is going these subclavicular catheter.
i think the catheter is the key.
Is lymphatic catheter?
The catheter was before diagnosis?
Good observation. It is a central venous catheter that has been pushed pass the right atrium. It is an accident and has no other significance.
….il quadro radiologico è quello di una malattia granulomatosa, per la presenza di micronoduli, prevalenti nel polmone medio-inferiore;non ci sono adenopatie nè ilari nè mediastiniche;non ci sono immagini cistiche( da air-trapping a causa di infiltrazioni linfoidi peri.bronchiolari)…,per queste ragioni si esclude rispettivamente , la sarcoidosi e la LIP(polmonite interstiziale linfocitica)…si vedono inoltre strie rx-opache, trasversali, Kerley-like in assenza di cardiopatia( probabilmente infiltrazione cellulari nei vasi linfatici, sub-pleurici)…..pertanto alla luce del contesto anamnestico di eventuale cr, la diagnosi piu’ probabile è linfangite carcinomatosa.
Intersticial pneumonia.
Lymphangitic carcinomatosis
I agree with Gaborini, it can be lymphangitic carcinomatosis.
Interstitial pneumonia.
How is her lateral chest graph?
Fibrosi interstiziale idiopatica: No carcinosi endolinfatica diffusa!!!!!!
Hello, IMHO
the severity of this case is caused by inconsitency of the x-ray appaerence and clinical image and demographics.
Difuse fibrosis with interlobular septal thickening- in the right lower lobe the changes have tendency to consolidate (really can’t say if anything is hiding there)- this made me think Intertitial neumonia but the patient’s age is not right.
In the upper poles I think I can see discrete nodular pattern that could be caused by Lymphangitis carcinomatosa or Sarcoidosis- no apparent npl diseaserules out LC so I’m left with Sarcoidosis although the distribution of changes is atypical.
Unless this patient has an autoimmunological disorder like SLE?
How often do you see widespread Kerley lines in sarcoidosis vs. lymphangitic carcinomatosis?
What is meaning of IMHO?
IMHO- in my humble opinion :]
Kerley lines are way more often in lymphangitic carcinomatosis but:
-would they be so diffuse and symmetrical and do We have a known malignancy?
-sarcoidosis has many faces and this appaerance would be quite a rare case as the previous ones 😉
can’t wait for the answer
….per la Sarcoiodosi, che effettivamente può presentarsi UNICAMENTE, con un quadro parenchimale, ci sono i segni clinici di una patologia Sistemica, nonché i risultati sierici di aumento ACE, nonché positività del test di Kveim….secondo IMHO….
Sorry to disagree with you. In my not-so-humble opinion (quoting Snoopy,it’s difficult to be humble when you are as great as I am), widespread lymphangitic carcinomatosis is not uncommon in G.I. tumors. It is very uncommon in sarcoidosis, in my experience.
….la risposta che hai data era per me o per Murzin?…..io dicevo che non poteva essere sarcoidosi,( solo parenchimale) anche perchè non hai citato eventuali segni sistemici della sarcoidosi, nonchè eventuali dati di laboratorio( ACE…B2microglobulina…BAL…) che accompagnano una Sarcoidosi…per me la diagnosi, come nel primo commento è linfangite carcinomatosa
Also in stage IV? I haven’t ever really seen one- I thought that fibrotic in sarcoidosis changes could have this appaerance… also in sarcoidosis.
I’ll surely remember that.
Were the shortness of breath and x-ray image first findings in this case or the malignant process was well known all the way ?
To Genchi Bari: the answer was obviously for Murzin.
To Murzin: this chest was pre-op. We suspected GI carcinoma and investigated the clinical history.
Patient had a gastric carcinoma. Her doctor was informed and intervention suspended.
….grande dott Pepe,,, come il Barca ed il…..Bari!!!!!!
The Kerley B lines suggest interlobular septal thickening.
The normal heart and the demographics go against pulmonary edema.
The absence of upper and middle lobe compromise go against sarcoidosis, but the sex, age and symptoms do correspond.
Lymphangitic carcinomatosis is a good option for a 36 years old woman, in the context of breast cancer mainly.
An interstitial pneumonia can not be excluded, but I would like ground glaas opacities. I would love a HRCT.
I pick lymphangitic carcinomatosis as my first option.
Greetings!
I agree with the group suggesting lymphangitic carcinomatosis.
Good for the group!
Chest X Ray PA view
Diffuse, bilateral reticulonodular opacification with Kerley B lines is noted especially in the right lowr zone suggestive of lymphangitic carcinomatosis.
The primary sites are the breasts (mostly) or GIT.
Friday is here and I want to thank you all for participating. Congratulations to Gaborini, who led the group that made the correct diagnosis.
Interstitial pneumonia
and there’s not only one single book or a collection of books that could consistently be used for training…some sort of Trojan horse that has infected all sources ok knowledge rendering us retarded…