Dr. Pepe’s Diploma Casebook: Case 79 – SOLVED
Dear Friends,
I would like to start the fourth season with an easy case. Showing pre-op radiographs for facial surgery of a 31-year-old woman. Check the images below, leave me your thoughts in the comments section, and come back on Friday for the answer.
Diagnosis:
1. Carcinoma of the lung
2. Subpulmonary fluid
3. Aspiration pneumonia
4. None of the above
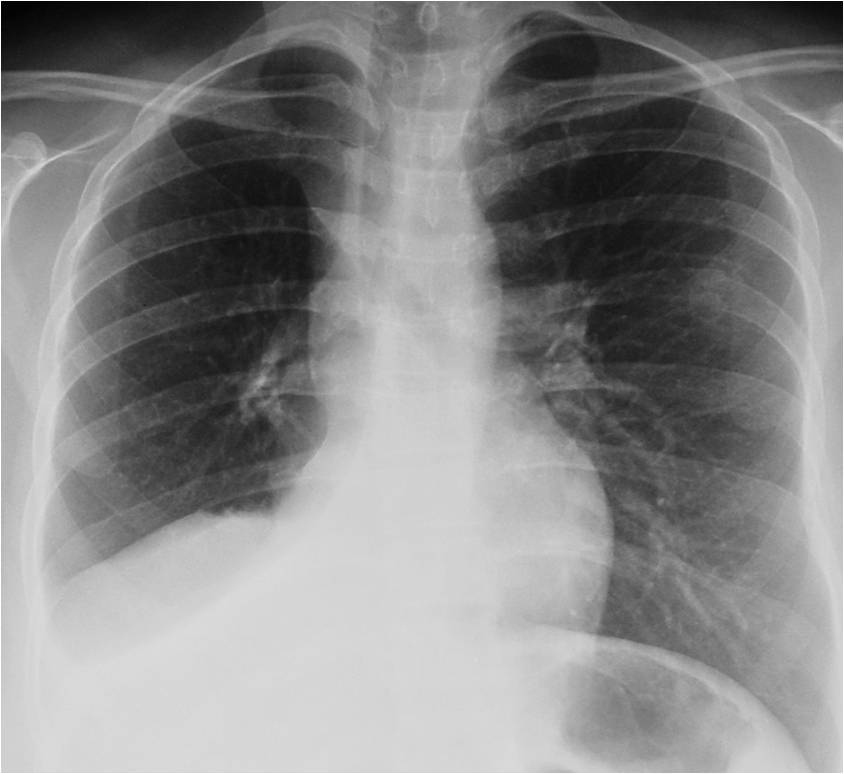
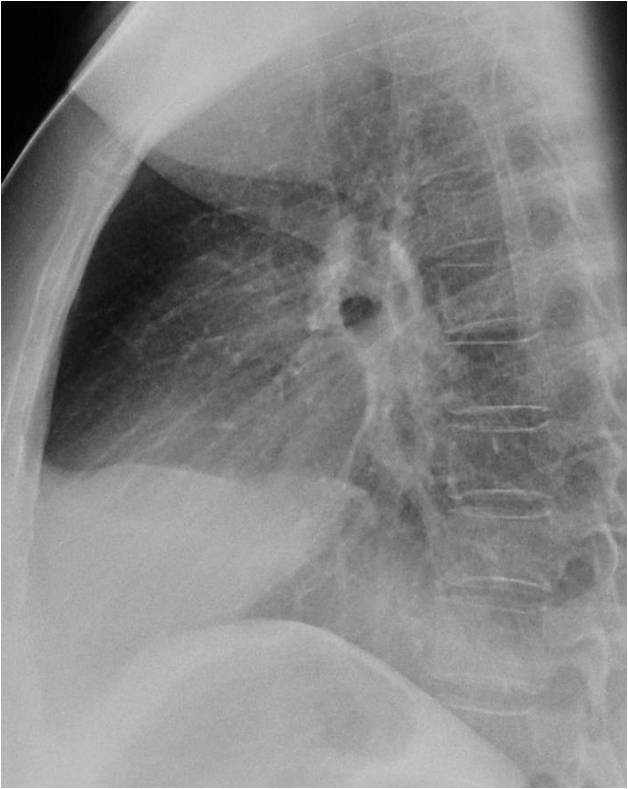
Findings: PA radiograph shows a triangular opacity in the right lower lung (A, white arrow) and an upper triangle sign (A, red arrow). These findings are highly suspicious of RLL collapse. There is also a mass in the right hilum, with narrowing and irregularity of the main bronchus (A, yellow arrow). A pathological fracture is visible in the left sixth rib (A,C, green arrow). The lateral view shows blurring of the posterior right hemidiaphragm (B, arrows).
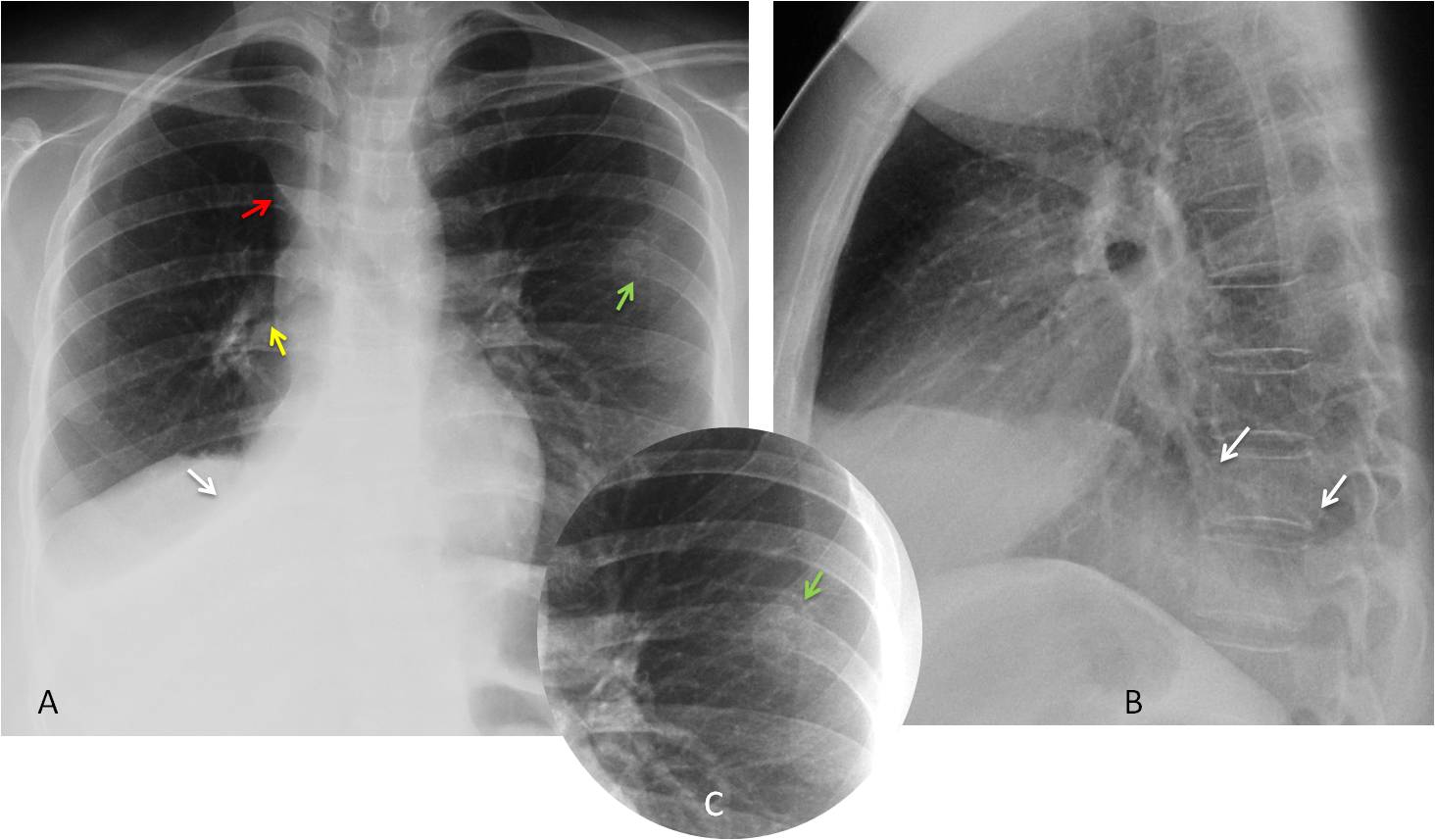
Unenhanced coronal CT confirms RLL collapse (C, D, white arrows) and the right hilar mass, with irregularity and narrowing of the main bronchus (C, D, red arrows).
Final diagnosis: bronchogenic carcinoma with RLL collapse
In this presentation I’d like to discuss common and uncommon manifestations of RLL collapse. RLL collapse is easy to recognise when typical signs are present. However, it can have an unusual appearance and be confused with other conditions, leading to a delay in the diagnosis. A prompt diagnosis is important because the main cause of RLL collapse is carcinoma of the lung, followed by inflammatory bronchiectasis.
The typical signs of RLL collapse in the PA view are a well-defined triangular opacity in the lower lung, accompanied by downward displacement of the hilum. The lateral view shows a posterior opacity that blurs the posterior diaphragmatic outline. The diagnosis is easily confirmed by CT (Fig. 1).
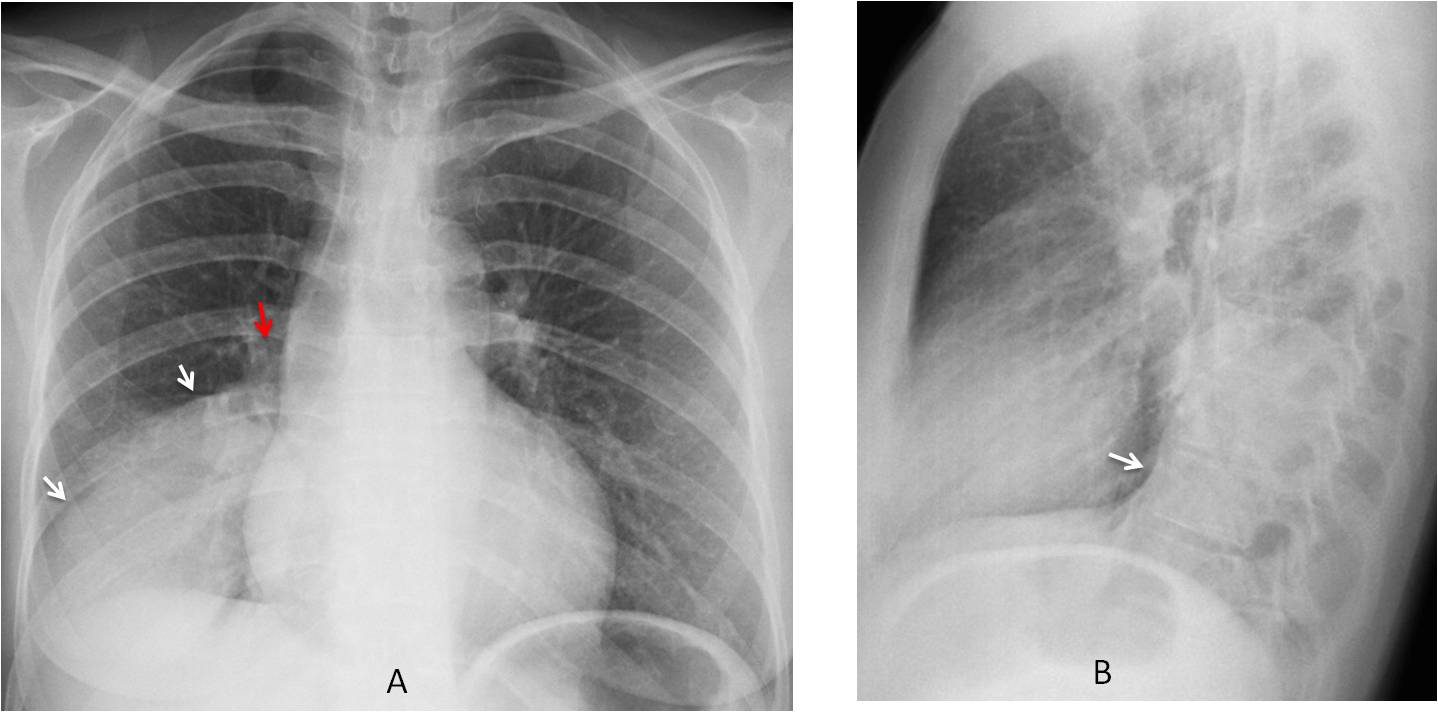
Fig. 1
Fig. 1: 55-year-old woman with carcinoma and partial RLL collapse. PA radiograph shows the triangular shape of the collapsed lobe (A, white arrows). The hilum is descended (A, red arrow). The lateral view shows a posterior opacity and concave major fissure (B, arrow).
Enhanced coronal and sagittal CT images confirm the collapsed lobe. The major fissure is displaced downward in the coronal view (C, white arrow) and is convex in the sagittal reconstruction (D, arrow). The obstructed bronchus is clearly visible (C, red arrow).
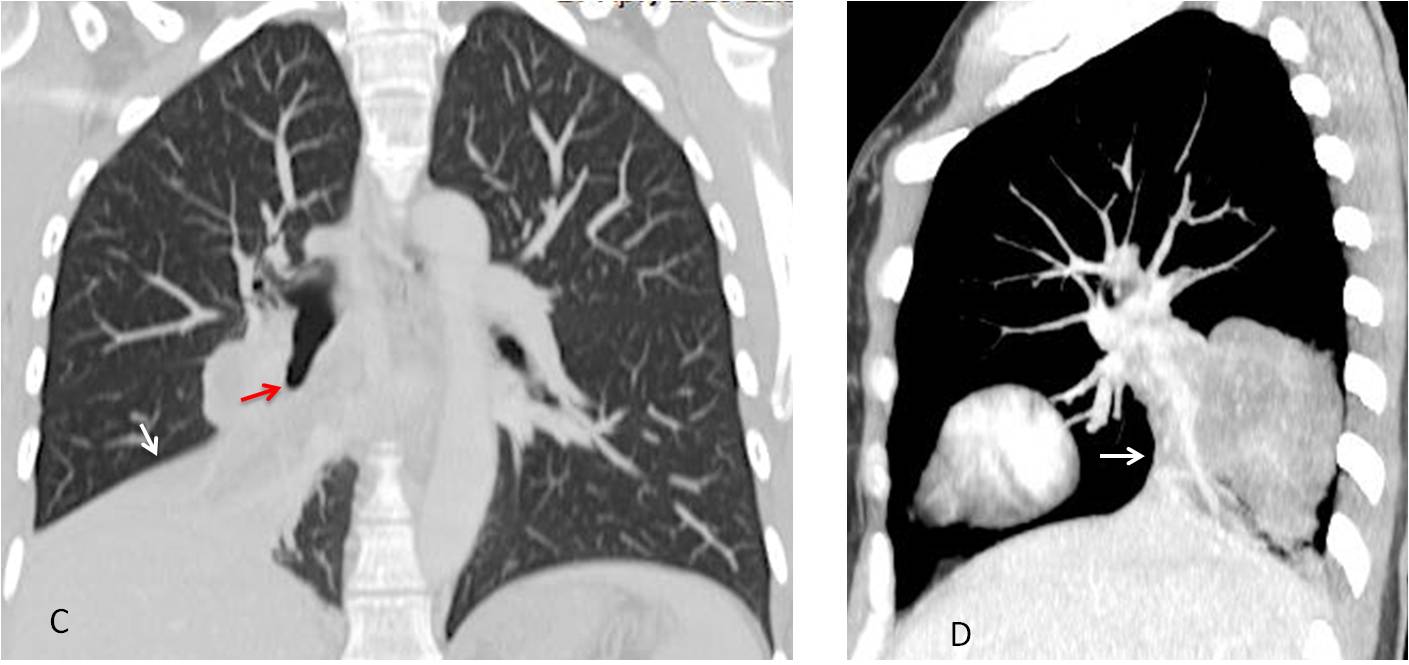
Fig. 1
A central mass causing RLL collapse may be visualized as an S, a variant of the Golden sign (Fig. 2).
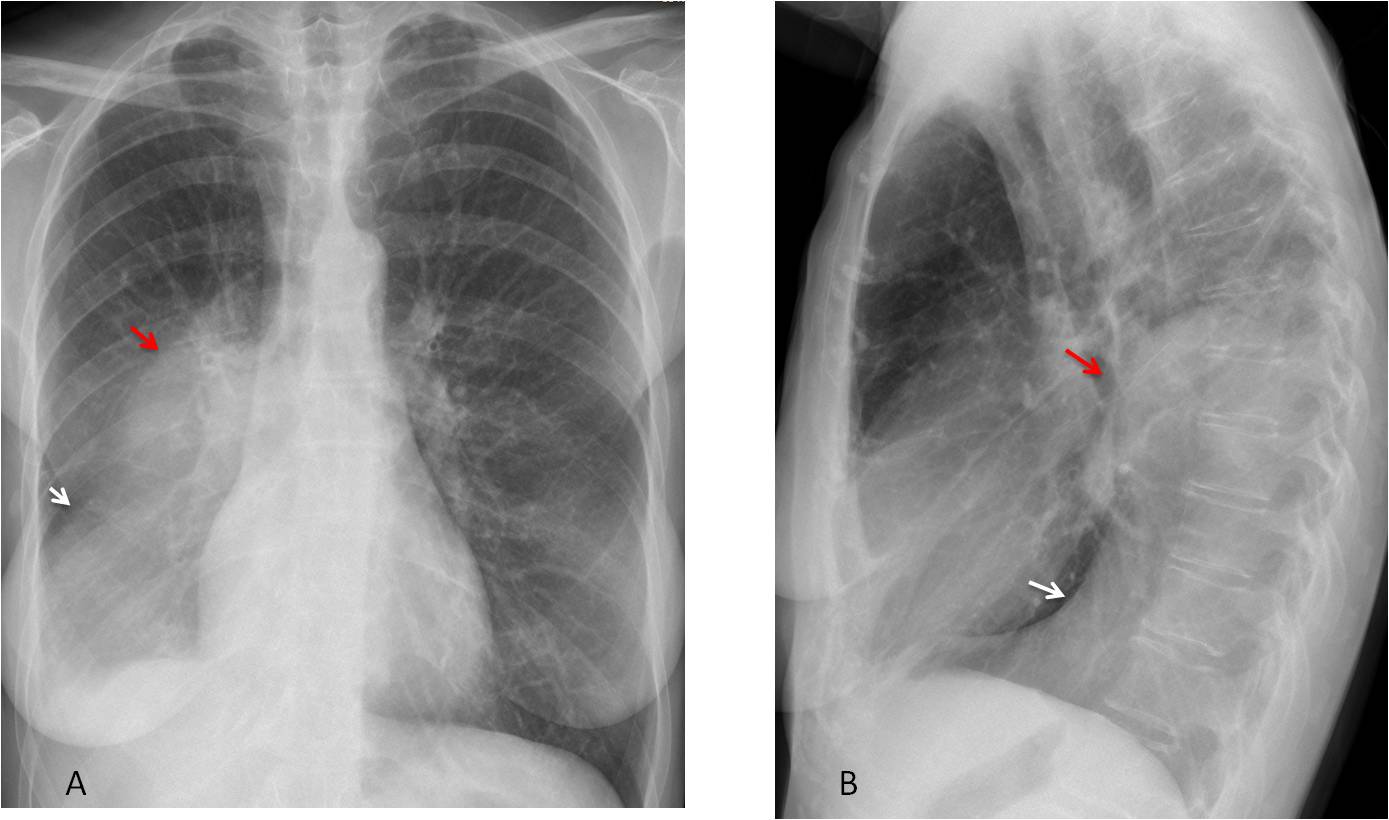
Fig. 2
Fig. 2: Carcinoma of RLL with Golden sign (A, B, red arrows). Note the oblique course of the displaced major fissure (A, white arrow), which is convex in the lateral view (B, white arrow)
Enhanced coronal and sagittal CT images confirm the central mass (C, D, red arrows), as well as the distal collapsed lobe (C, D, white arrows)
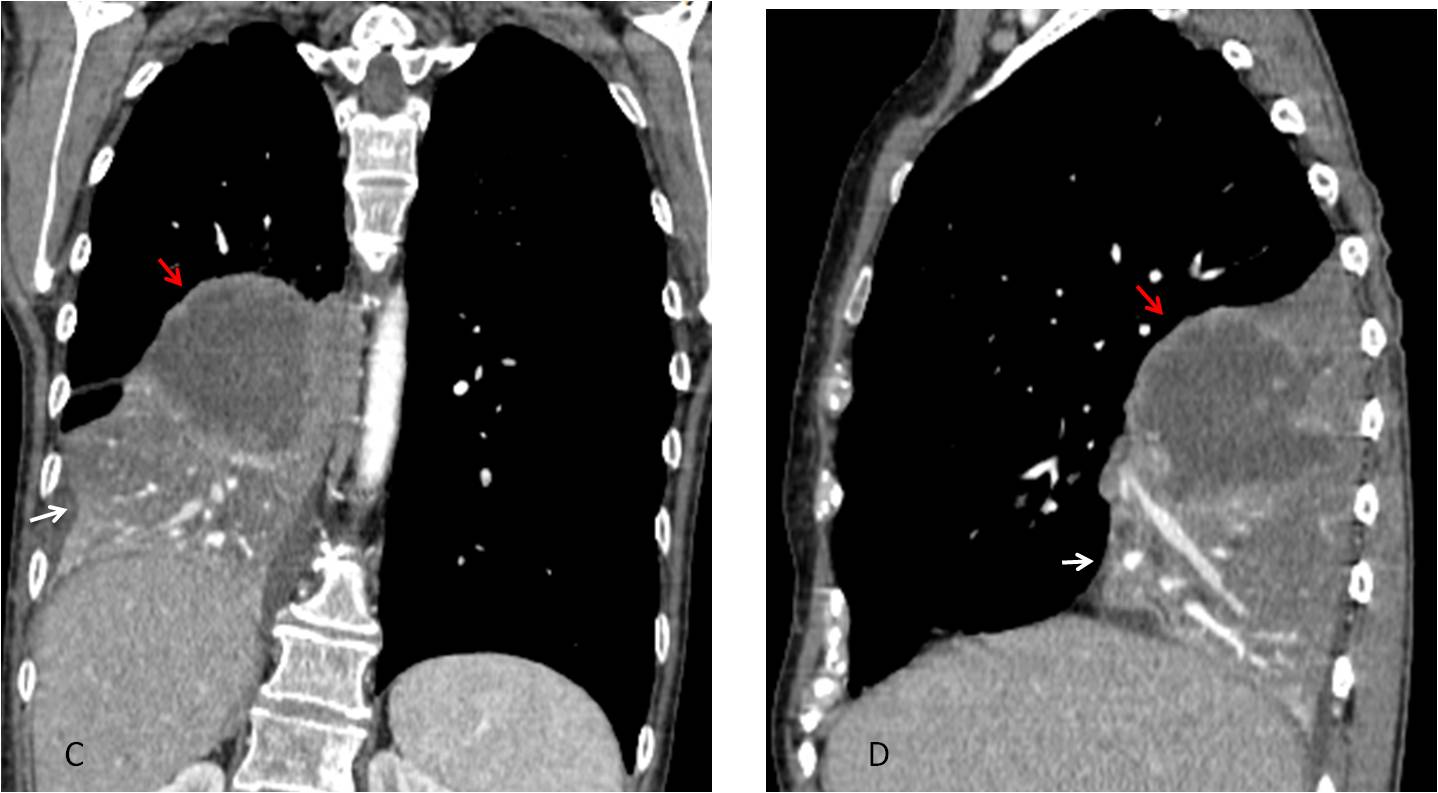
Fig. 2
In my experience, RLL collapse simulating pleural fluid is not uncommon. In this presentation form, the peripheral lung obliterates the costophrenic sinus in both views. The sharp interface of the major fissure helps to create the impression of pleural effusion. The clue to the correct diagnosis is the downward displacement of the hilum (Figs. 3 and 4).
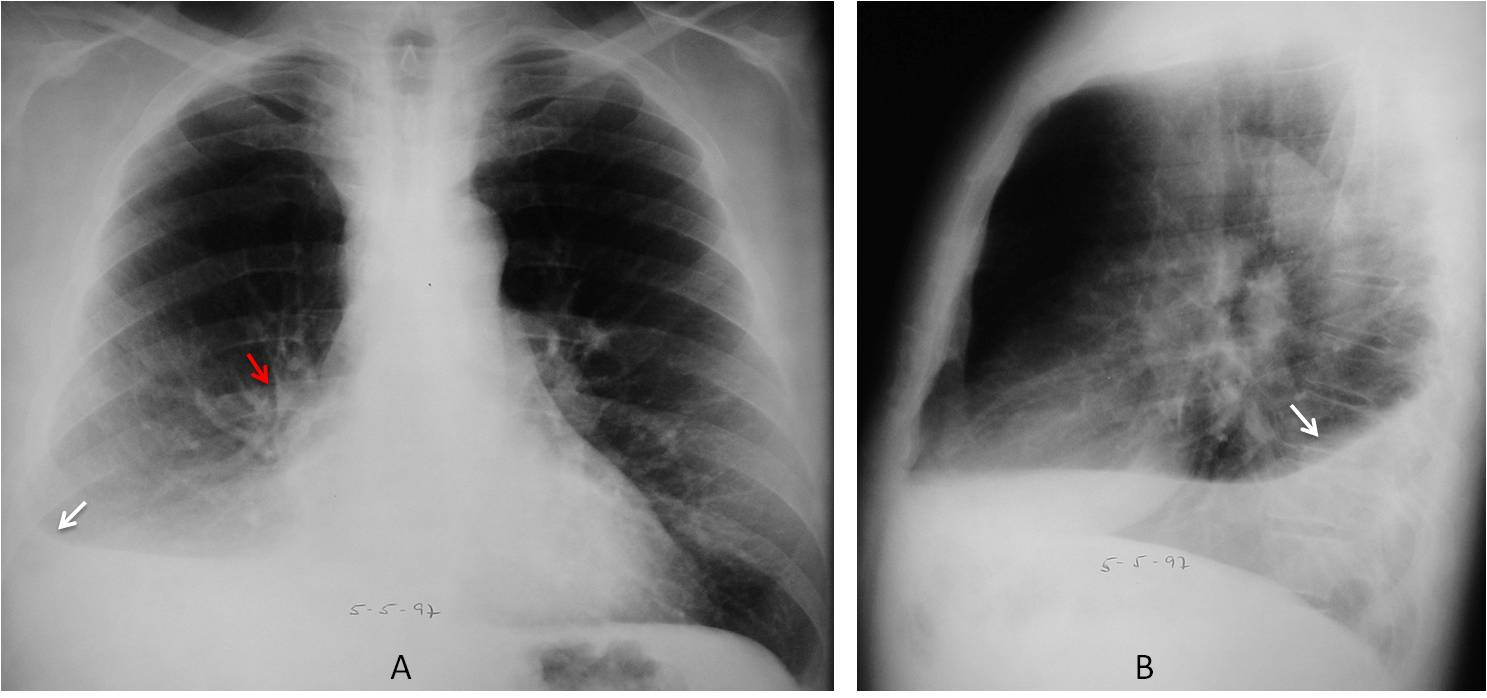
Fig. 3
Fig. 3: RLL collapse simulating pleural effusion. There is blunting of the costophrenic sinus in the PA radiograph with a horizontal major fissure (A, white arrow). The collapsed lobe in the lateral view simulates free fluid (B, arrow). Note the descended right hilum (A, red arrow).
Unenhanced axial CT shows marked narrowing of the RLL bronchus (C, arrow). The distal lobe is visible in the posterior costophrenic sulcus and shows an air bronchogram (D, arrow). There is no evidence of pleural fluid.
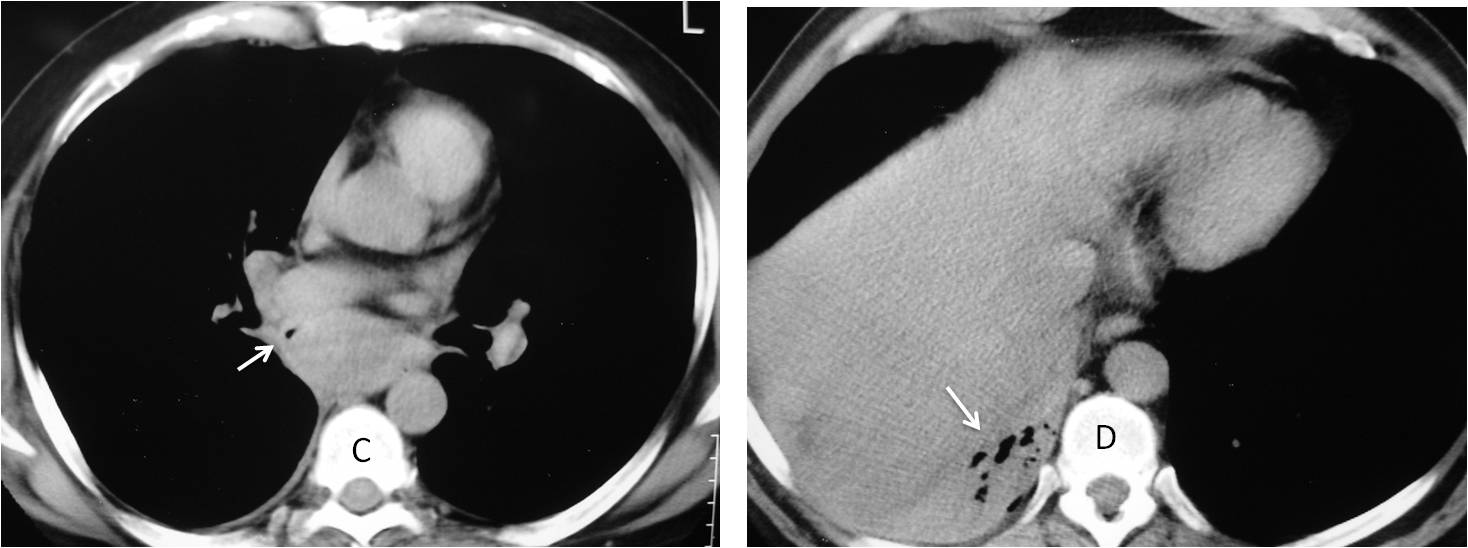
Fig. 3
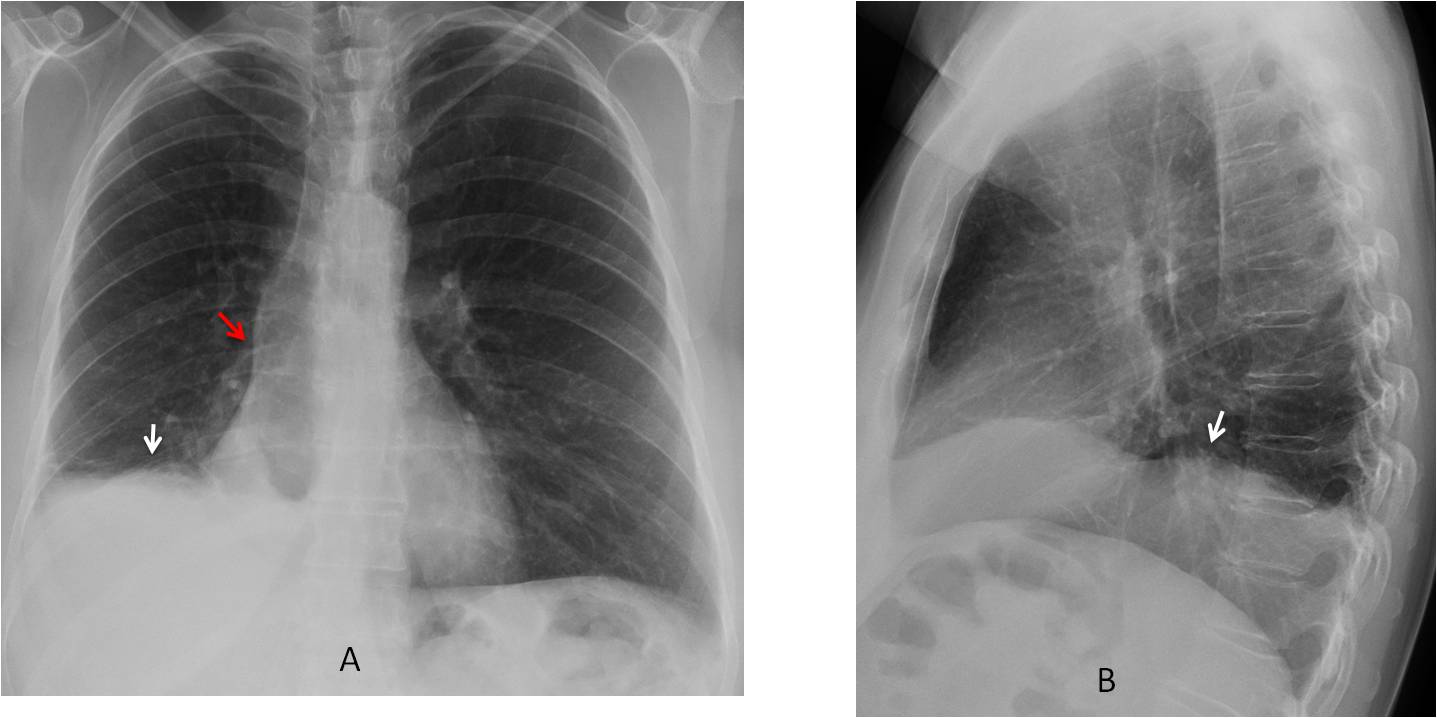
Fig. 4
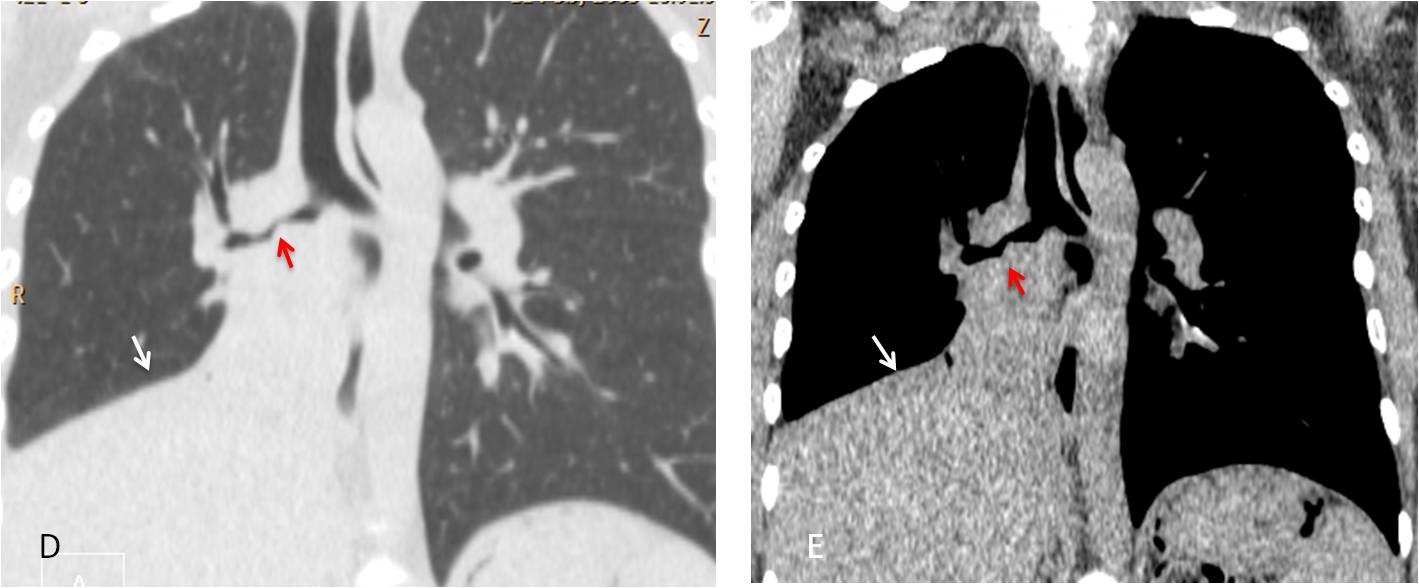
Fig. 4: 44-year-old woman with haemoptysis. PA and lateral radiographs depict an irregular right hemidiaphragm with the appearance of subpulmonary fluid (A, B, white arrows). However, the right hilum is descended (A, red arrow), which raises the possibility of RLL collapse.
Post-contrast CT demonstrates an enhancing sliver of RLL that simulates pulmonary fluid (C, D, arrows). A more cephalad slice shows occupation of he RLL bronchus (E, arrow). Bronchoscopy demonstrated a blood clot occluding the bronchus, with no evidence of tumour.
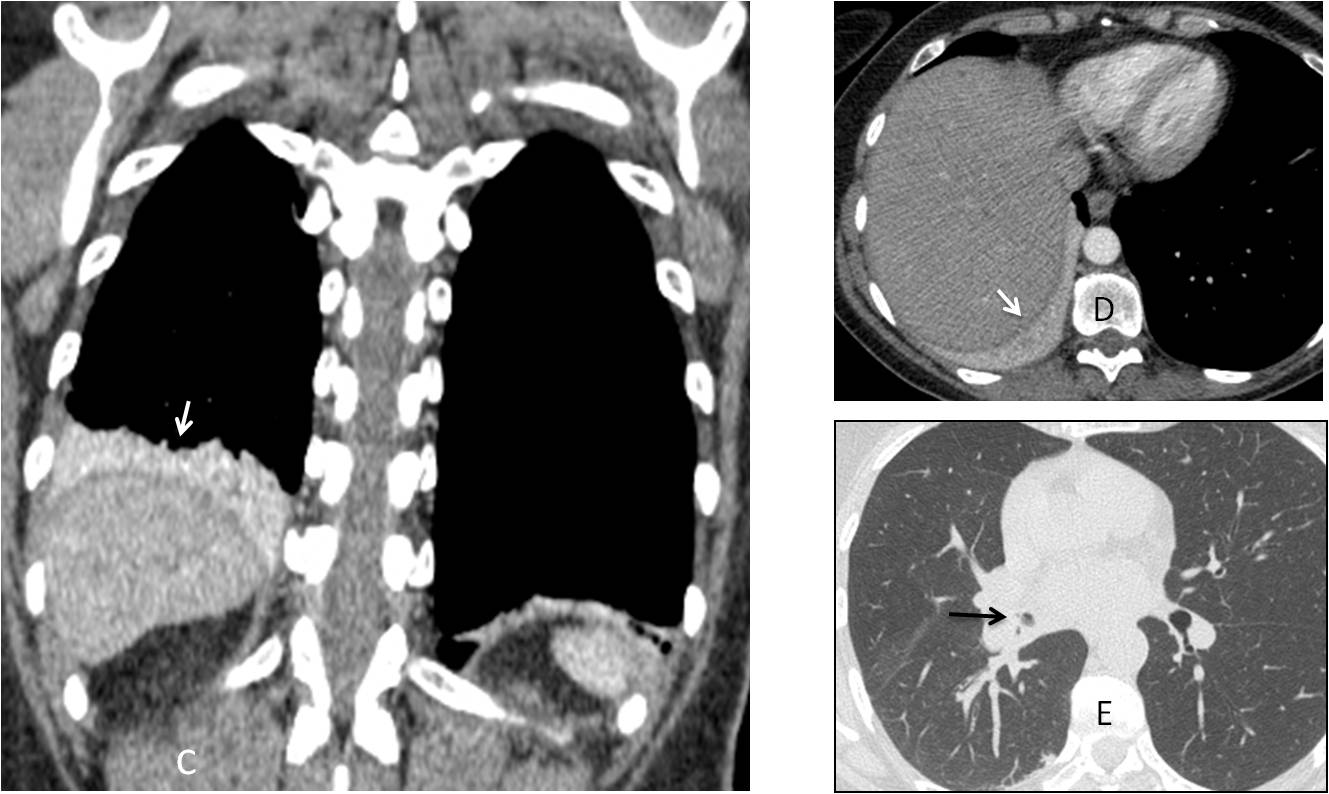
Fig. 4
On chest radiography a few days after bronchoscopy, the chest had a normal appearance. Note the normal aspect of the diaphragm and correct location of the right hilum (F, G, arrows).
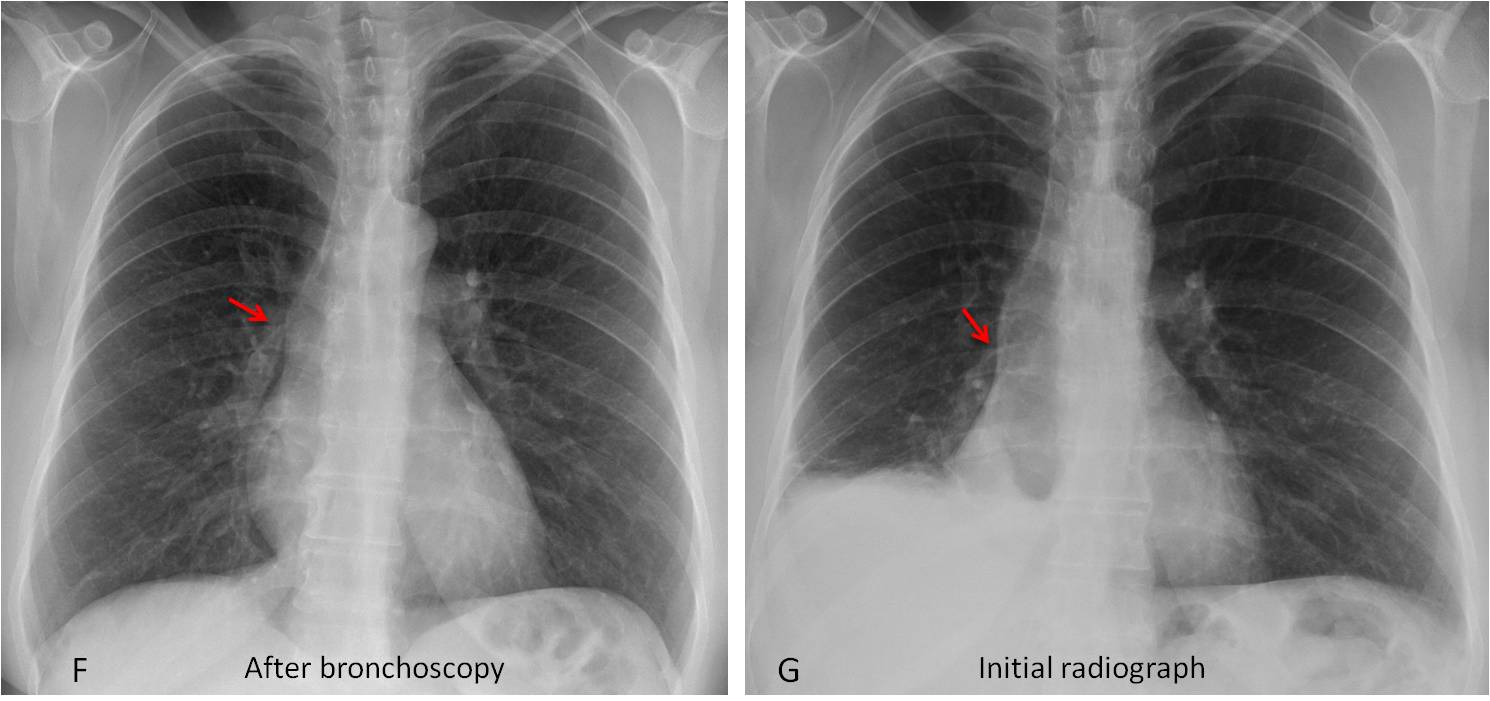
Fig. 4
In aerated RLL collapse the lobe loses volume but there is no increase in opacity, making the collapse less obvious. The descended hilum and major fissure are clues to the diagnosis (Figs. 5 and 6). The lack of opacity may be secondary to incomplete obstruction of the lobar bronchus, collateral ventilation through an incomplete major fissure, or both.
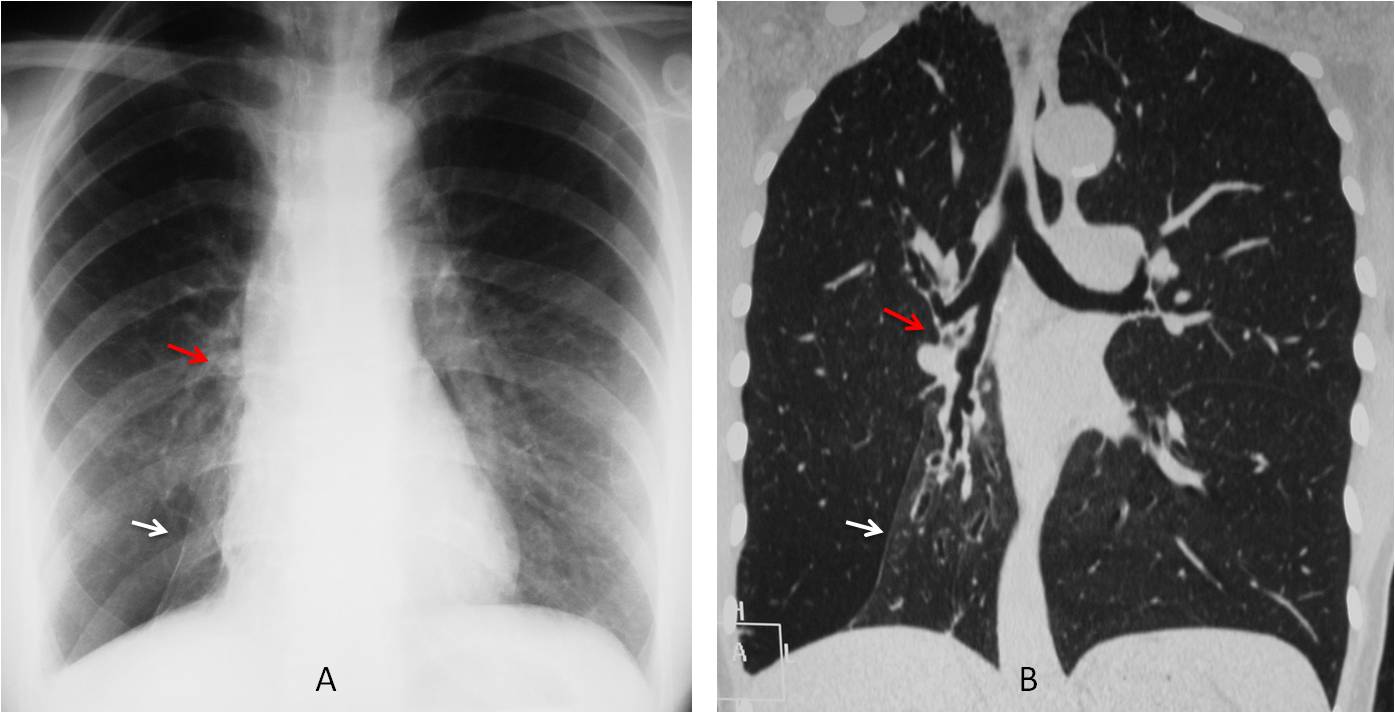
Fig. 5
Fig. 5: Aerated RLL collapse secondary to bronchiectasis. PA radiograph shows a markedly displaced major fissure simulating an inferior accessory fissure (A, white arrow). There is marked downward displacement of the right hilum (A, B, red arrows). Coronal CT shows the collapsed lobe (B, white arrow) with bronchiectasis and open RLL bronchus.
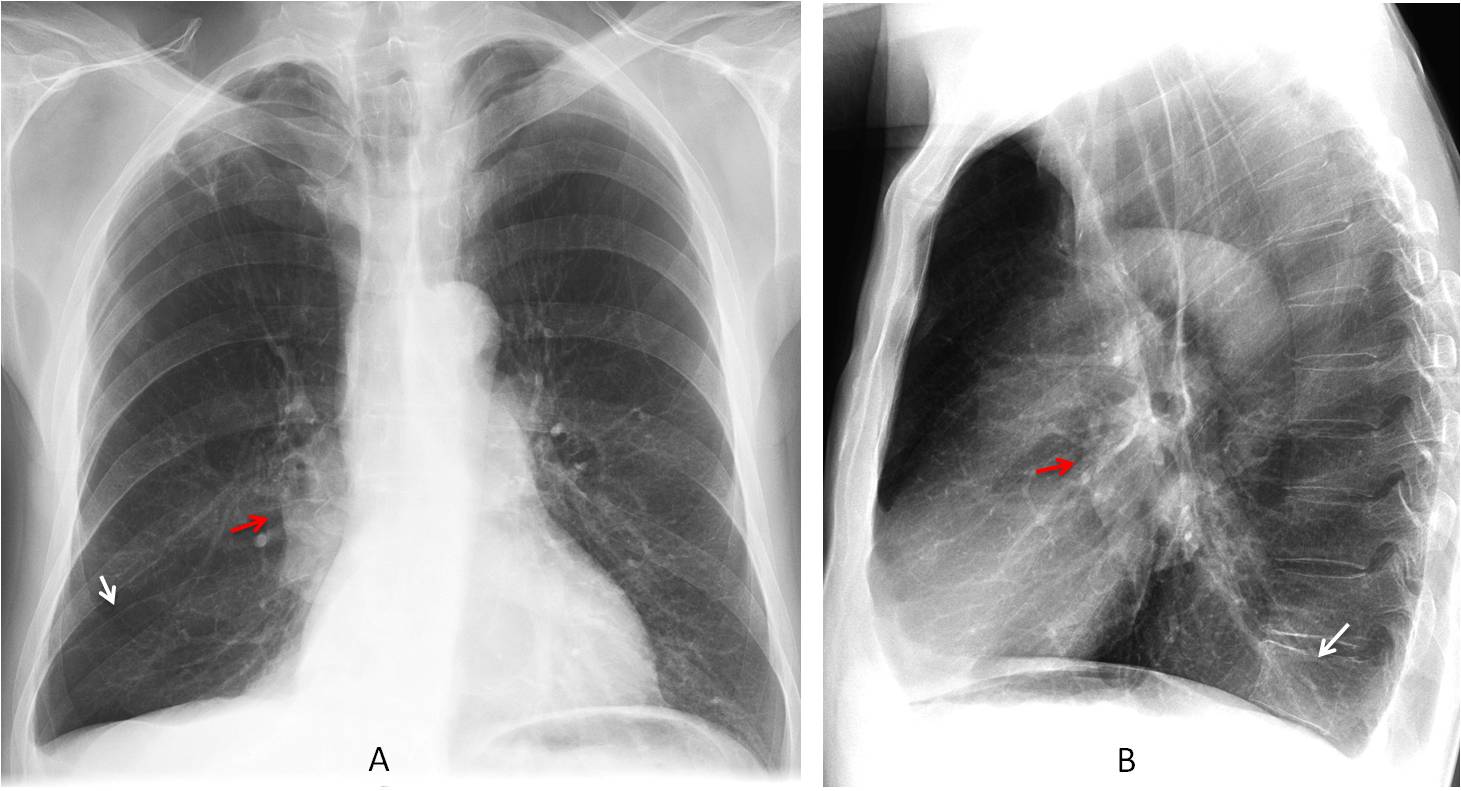
Fig. 6
Fig. 6: Aerated RLL collapse in carcinoma. PA chest film depicts a right hilar mass (A, B, red arrows), with descended hilum. The lowered major fissure is barely visible (A, white arrow). In the lateral view, the collapsed lobe is seen as a faint opacity projected over the spine (B, white arrow).
In marked RLL collapse the opaque lobe hides behind the right side of the heart and may be difficult to detect. The increased lucency of the expanded RUL may be misleading. The descended hilum and upper triangle sign, when present, are clues leading to the correct diagnosis (Figs. 7 and 8). The upper triangle is due to shifting of the superior mediastinum, secondary to RLL volume loss.
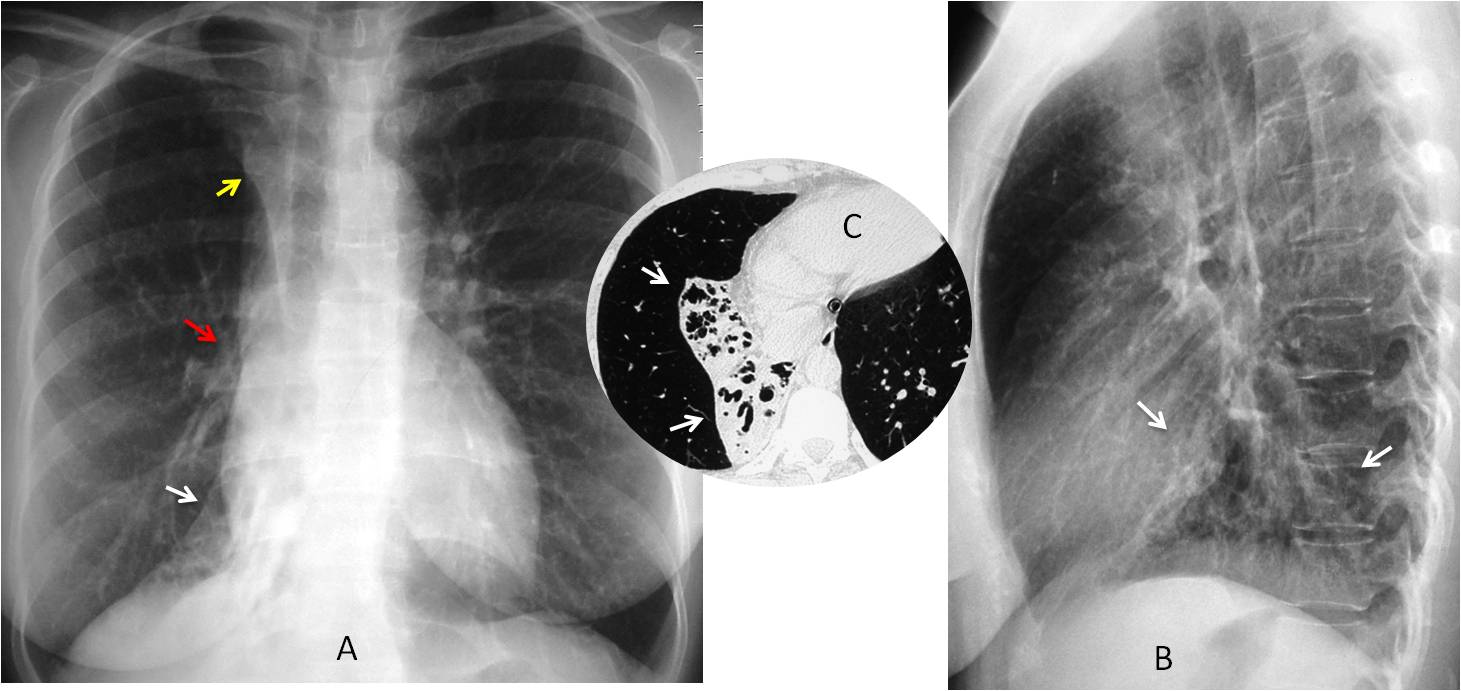
Fig. 7
Fig. 7: PA radiograph shows marked RLL collapse partially hidden behind the heart (A, white arrow), hilum displaced downward (A, red arrow), and upper triangle sign (A, yellow arrow). In the lateral view the changes appear as a triangular RLL opacity blurring the left hemidiaphragm (B, arrows). Diagnosis: inflammatory bronchiectasis (C, arrows).
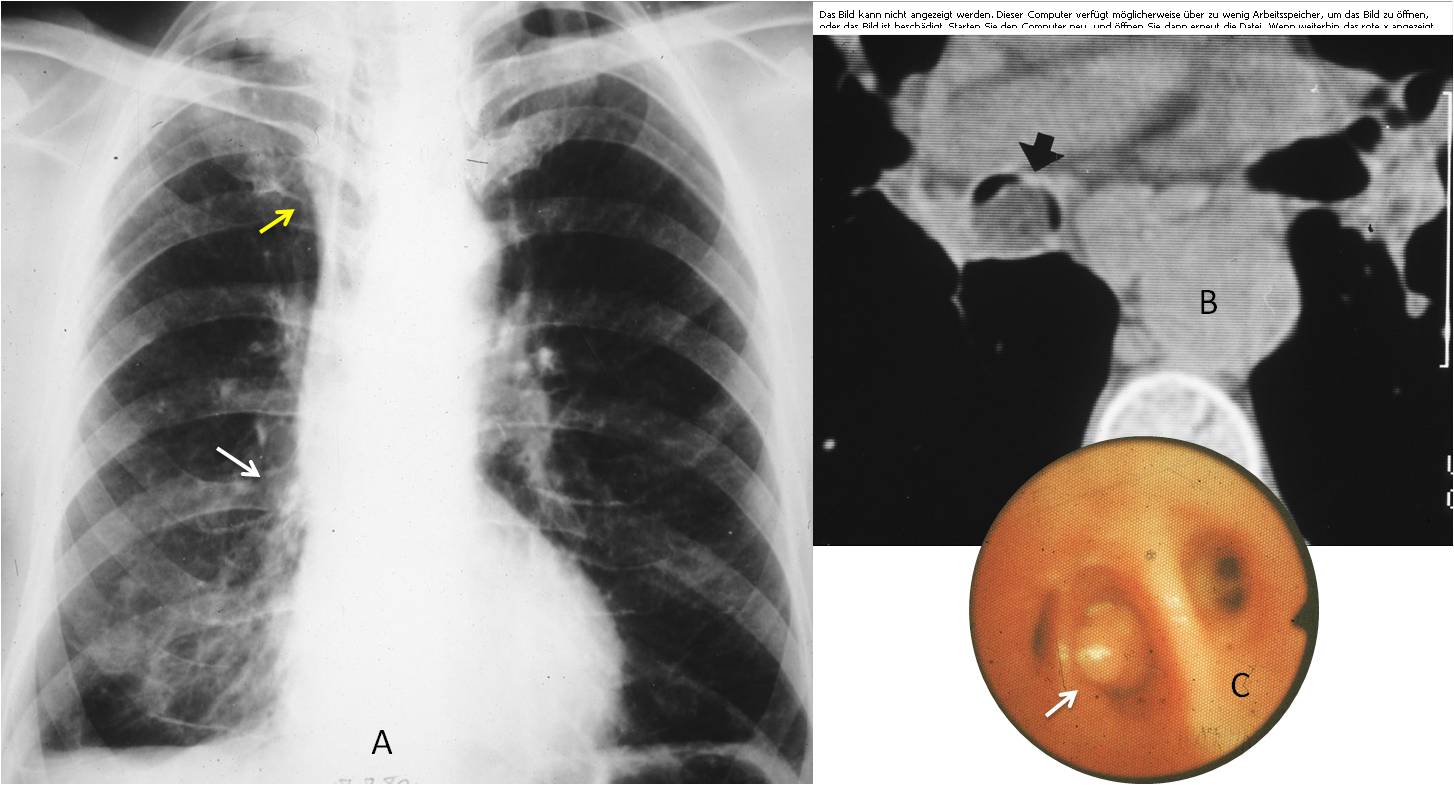
Fig. 8
Fig. 8: 65-year-old man treated in the outpatient clinic for non-specific respiratory complaints. The chest remained unchanged for several years, until somebody noticed the descended hilum (A, arrow) and the upper triangle sign (A, yellow arrow). Axial CT shows a fatty tumour inside the RLL bronchus (B, arrow), confirmed with bronchoscopy (C, arrow). Diagnosis: endobronchial lipoma.
Follow Dr.Pepe’s Advice:
1. In the PA view, typical RLL collapse appears as a triangular opacity at the base of the lung with downward displacement of the hilum.
2. RLL collapse may simulate pleural effusion. Look for a descended hilum.
3. Aerated RLL collapse may be overlooked. It is suspected by visualization of a descended hilum and major fissure.
4. Marked RLL collapse may be hidden behind the right heart. Look for a descended hilum and upper triangle sign.


Right middle and probable lower lobe atelectasis -/+ small pleural effusion.
Right hilum bulky with irregular thickening of main bronchial walls.
i think 1
I would like to choose subpulmonary fluid, but seeing the lateral film the ‘fluid’ is not in dependent position. Does not seem to be carcinoma. Aspiration pneumonia i dont think so to be so well defined. Maybe 4?
I agree with Gus. There is RML atelectasis with silhouette sign of right heart border and medial part of diaphragm. Also mediastinal shift to the right is seen.
Answer nr 1 is best choice.
There is a right lower lobe atelectasis and for that reason the posteror portion of the right hemidiaphragm is blurred. The RML seems to me normal. RLL bronchus is narrowed and seems like beaded and posterior wall thickening in the lateral view. There can be hilar calcified lymph nodes and left pleural calcification. For me there is no clear evidence of very enlarged right hilar lymph nodes regarding the lateral view. Patient is young. I would compare with previous looking for the chronicity of the RLL loss of volume. If it is new I would do a CT for ruling out a bronchial carcinoma or a foreing body. If it is old I would go for an old TB causing RLL bronchus stenoses or a right lower lobe hypoplasia. If there are not previous chest x rays I would do a CT because there is a possibility of lung cancer
Nice discussion. Will give you a hint: satisfaction of search.
Then I see the right hilum is well possitioned which shouldnt be in a RLL athelectasis. Could it be a mass in the right lower portion either pulmonary or pleural a fibrous mesothelioma for example?
Or a right subpulmonary effusion as well
Rt lower lobe consolidation collapse. The lower vertebrae in the lateral image are whiter than the upper ones. With subpulmonary effusion.
?Rt middle lobe consolidation – the triangular opacity on the lateral image.
2 subpulmonic fluid. US correlation suggested.
iperchiarezza del polmone dx, in relazione ad iperventilazione vicariante da atelettasia del lobo polmonare inferiore dx e versameNto pleurico. lieve attrazione omolaterale dell’ombra cardiomediastiNIca e scarsa definizione dell’ilo…A SX .sembrano evidenziarsi due tenui opacità in campo polmonare superiore.
So far, nobody is looking at the whole film.
il bronco principale di dx è irregolarmente distorto, ristretto e non sede….è chiaro che una TC, con ricostruzioni sul piano coronale chiarirà tutta la patologia…
Opacity in the left lung?
Getting warm…
rib metastasis?
Finally!
a nodular well circumscribed opacity in the left middle lung zone suggestive of ? lung CA. there is also RLL collapse.
Before the answer is posted, I want to congratulate Gus, who was the first the mention the correct diagnosis and the one that discovered the rib metastases.
…l’irregolarità e stenosi del bronco principale era stato segnalato, così pure la sospetta opacità in campo polmonare superiore di sx….oltre naturalmente al collasso del lobo polmonare inferiore dx…