Dr. Pepe’s Diploma Casebook: Case 98 – A painless approach to interpretation (Chapter 5) – SOLVED!
Dear Friends,
Today we are moving to a new chapter in the Painless Approach to Interpretation, addressing what to do when the chest radiograph does not show an obvious abnormality.
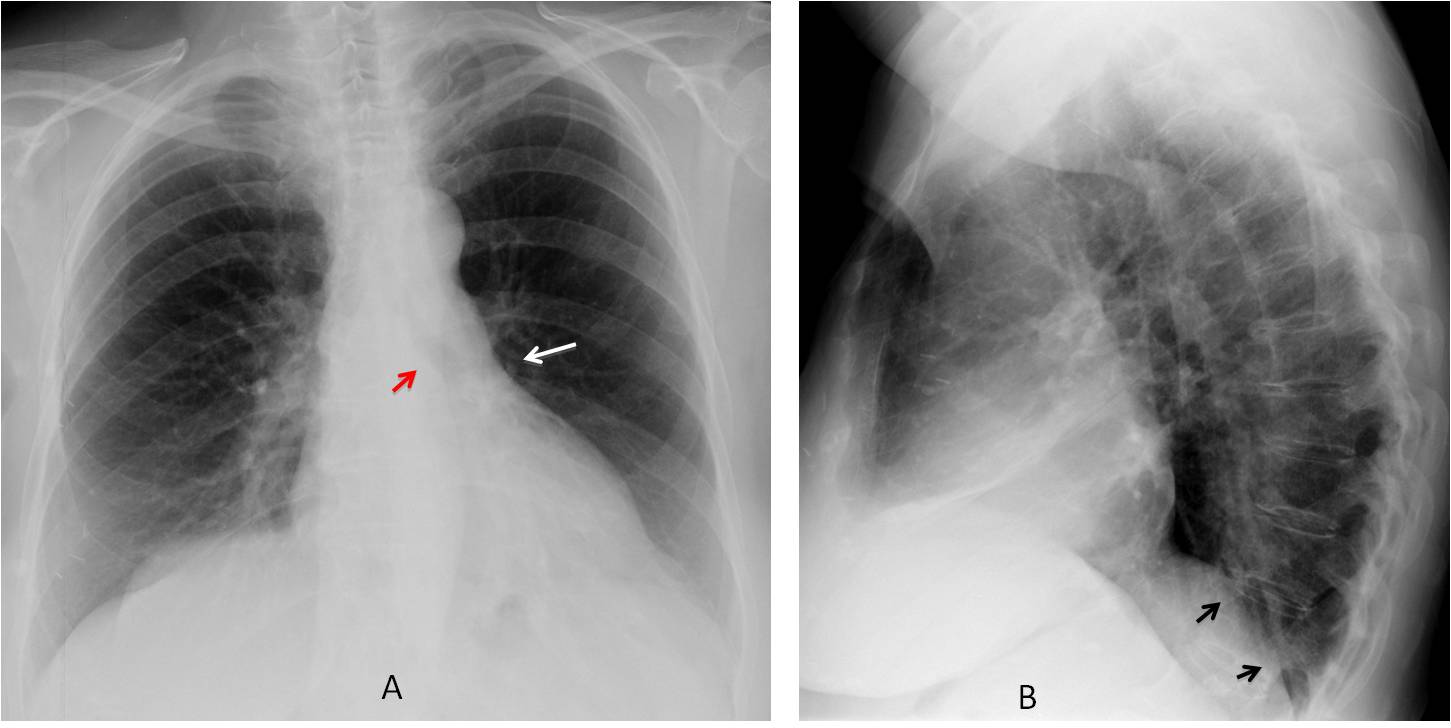
For this purpose I am presenting the PA and lateral radiographs of a 57-year-old man with a chronic cough. What do you see?
Examine the image below, leave your thoughts in the comments section and come back on Friday for the answer.


Findings: PA film shows increased lucency of the left lung. The left hilum appears small because it is descended and hidden behind the cardiac silhouette (A, white arrow). The left bronchus is vertically oriented (A, red arrow). In the lateral view, there is blurring of the left hemidiaphragm (B, arrows).
These signs are characteristic of LLL collapse with increased lucency of the left lung due to compensatory expansion of the LUL.
Coronal CT MIP reconstruction confirms the descent of the left hilum (C, white arrow) and the vertical orientation of the main left bronchus (C, red arrow). No endobronchial lesions are seen. Coronal CT shows partial collapse of the LLL with medial displacement of the major fissure (D, white arrow) and bronchiectasis (D, red arrows). There is compensatory elevation of the left hemidiaphragm.
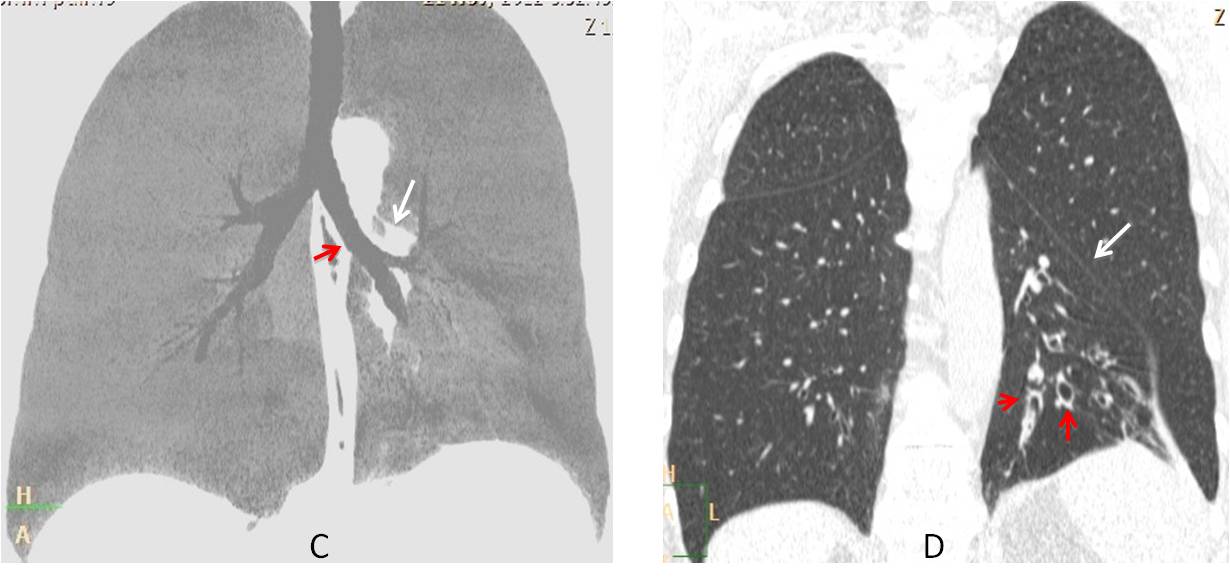
Final diagnosis: LLL collapse, secondary to bronchiectasis.
I am presenting this case to point out that radiographic findings are not always obvious and may be overlooked. To avoid that, it is convenient to use checklists that remind us to review areas where disease may be hidden. The objective of the next four chapters is to present basic checklists to use when viewing PA and lateral radiographs.
In this chapter I will discuss the initial checklist for the PA radiograph, which should include the following areas or anatomical structures:
The hila
The fissures
The apical region
The costophrenic sinuses
The pulmonary hila should be the first structures investigated. As we all know, the two hila represent the right and left main pulmonary arteries. They are both about the same size and density, and for practical purposes, are at the same level (Fig. 1A). In our checklist we should look for changes in the position of one hilum (elevated or descended) or changes in size/density (Fig. 1B).

Fig. 1
Fig. 1: Normal hila (A, arrows). Note that their density is similar and they are at the same level. In another patient, chronic TB has resulted in marked elevation of the left hilum (B, arrow), which is also denser than the right one.
Elevation/descent of a hilum is indicative of lobar collapse. Since most cases of lobar collapse in adults are due to an endobronchial neoplasm, this finding should not be overlooked, even though it may not be obvious at first glance (Figs. 2-3).
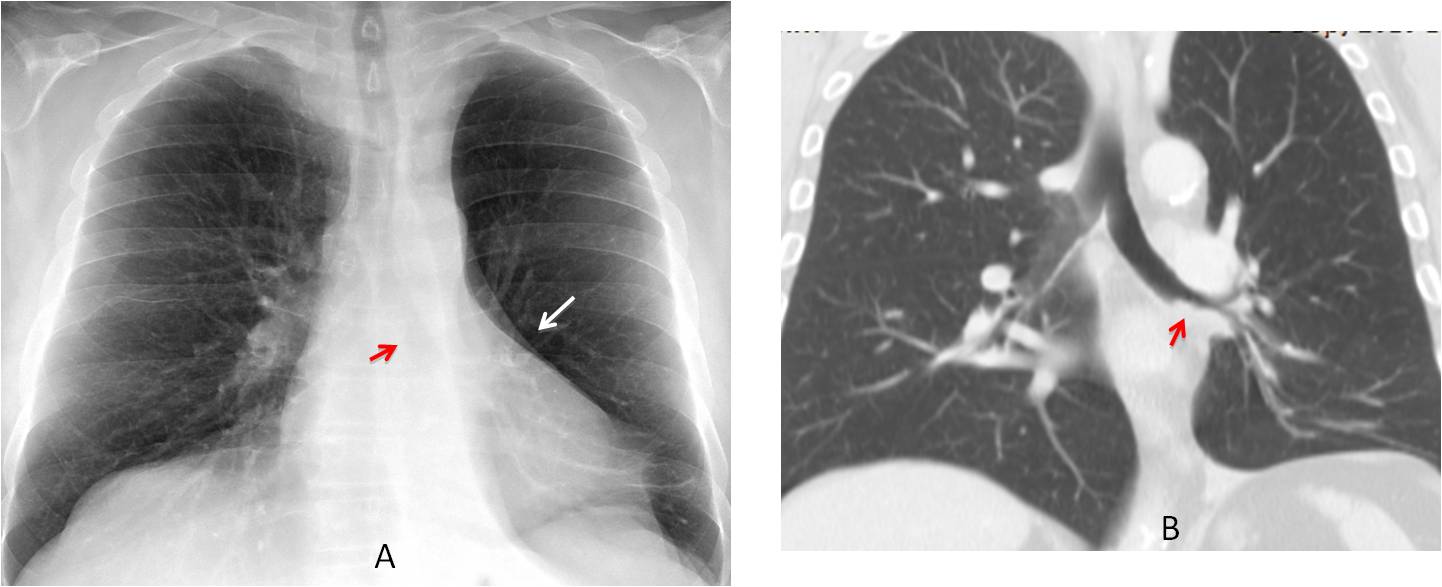
Fig. 2
Fig. 2: Pre-op film for cataracts in a 72-year-old man. PA chest film shows a markedly lucent left lung. There is pronounced downward hilar displacement (A, white arrow) and verticalisation of the left main bronchus (A, red arrow). Coronal CT depicts a mass obstructing the LLL bronchus (B, arrow). Final diagnosis: carcinoma.
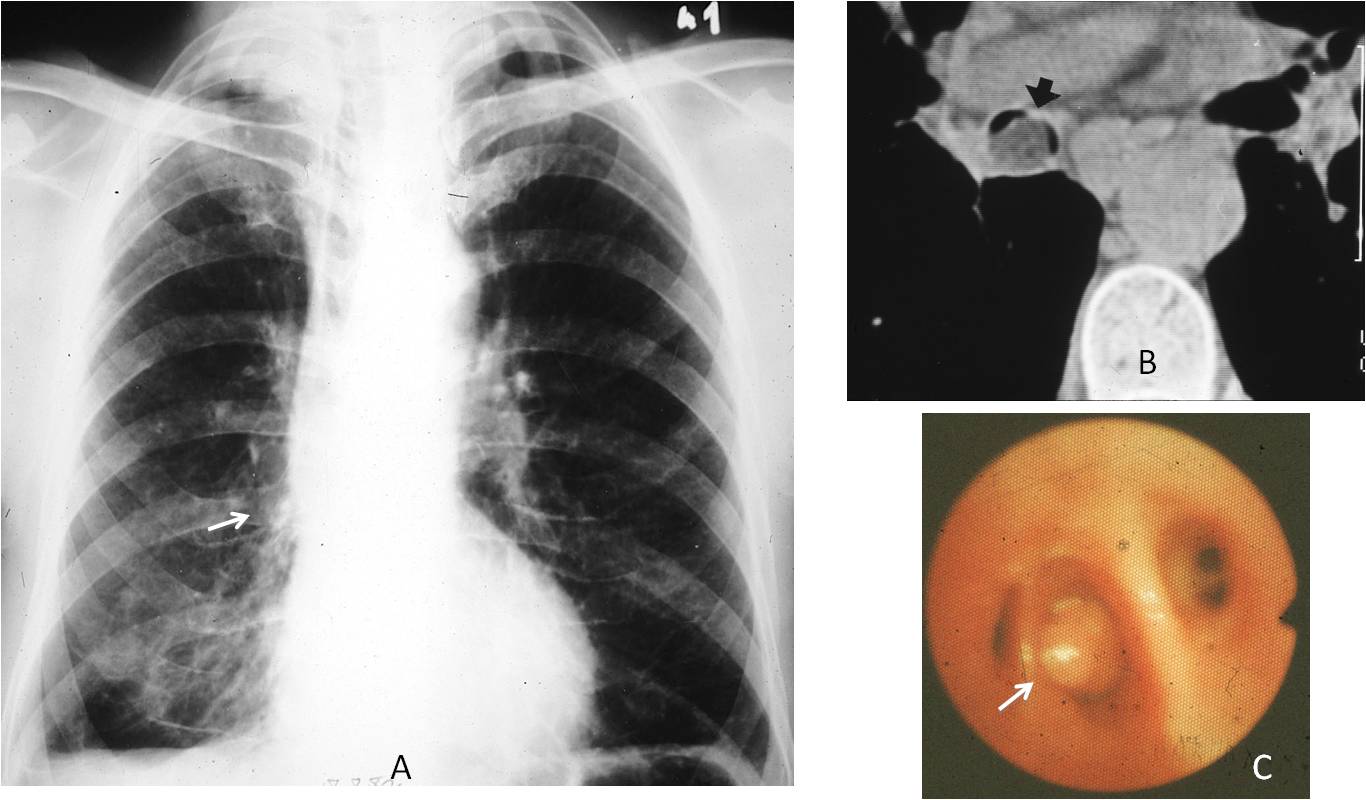
Fig. 3
Fig. 3: 57-year-old man with chronic cough. PA radiograph shows marked descent of the right hilum (A, arrow). This finding prompted a CT, which discovered a fatty mass within the RLL bronchus (B, arrow). Bronchoscopy discovered a yellowish tumour (C, arrow). Surgery confirmed an endobronchial lipoma (This case made me very happy, because I was the one who discovered the abnormality in 1982).
Unilateral increase in hilar size/density is easily recognisable by comparing with the opposite hilum. In my experience, increased hilar opacity is more reliable than increased size. The three main causes of increases in size/density of the hilum are: bronchogenic carcinoma, lymphadenopathy, and enlarged pulmonary artery (Figs. 4 and 5).
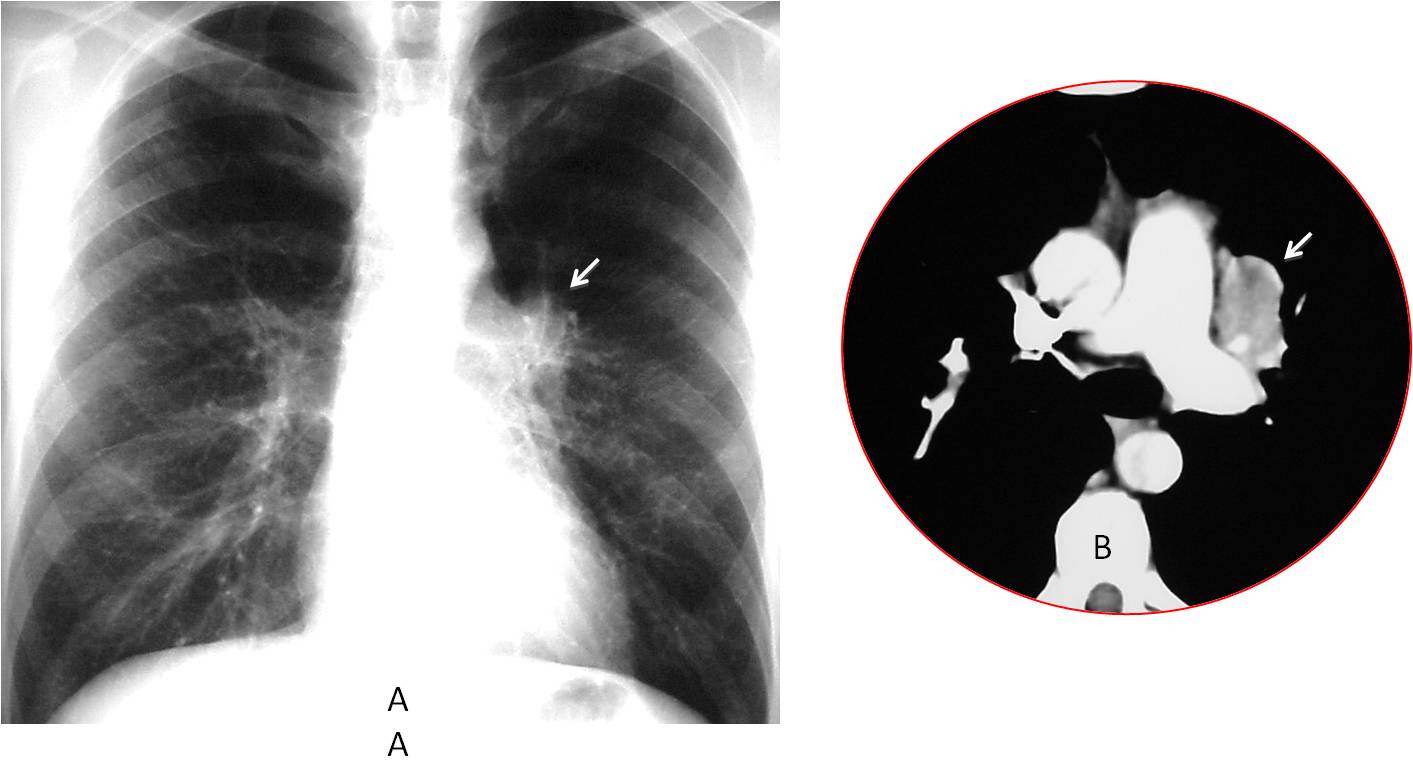
Fig. 4
Fig. 4. Increased opacity of a normal-sized left hilum (A, arrow). Enhanced axial CT shows a lung mass in the left hilum (B, arrow). Diagnosis: bronchogenic carcinoma.
Enlarged pulmonary artery is a less common cause of unilaterally increased hilar size/density. Enhanced CT is needed to differentiate the artery from a hilar mass (Fig. 5).
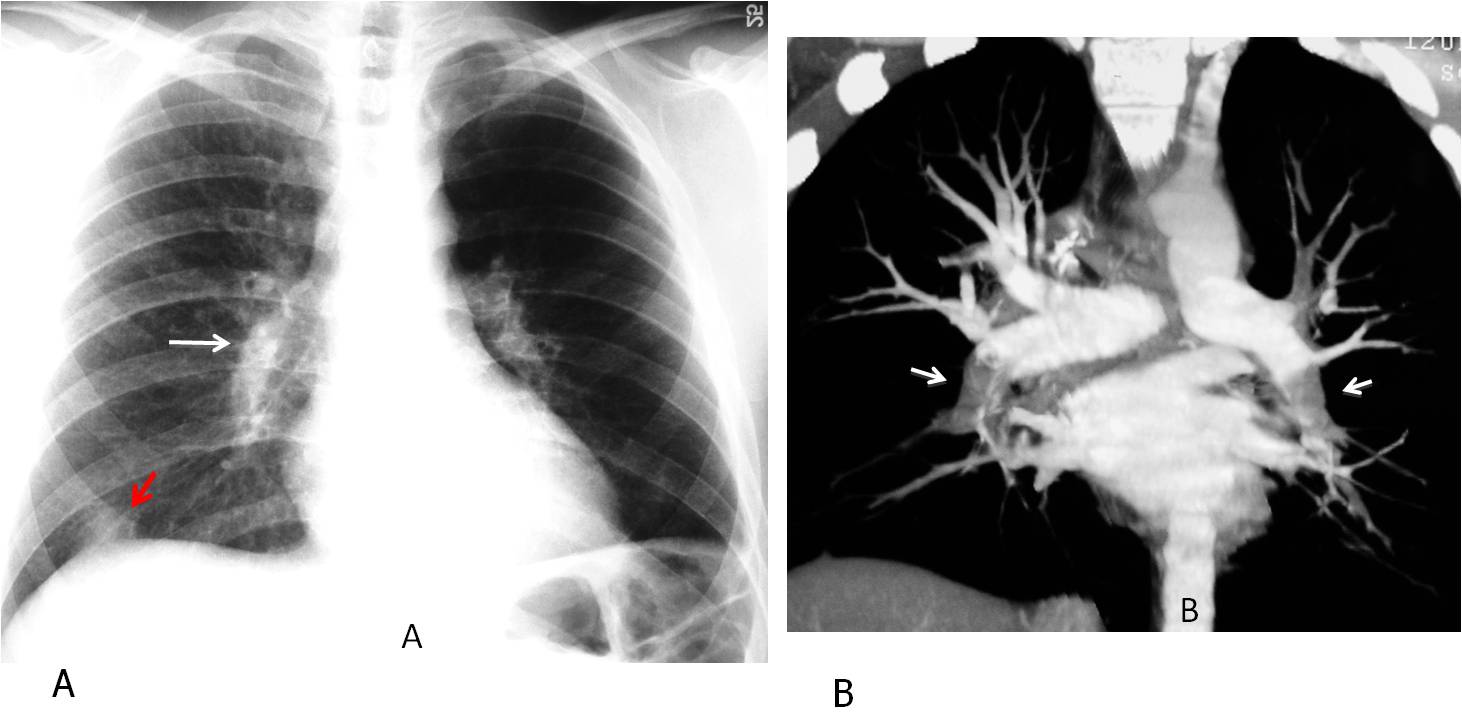
Fig. 5
Fig. 5: 23-year-old diabetic man with a pulmonary embolism. Note the enlarged, dense right hilum in the PA radiograph (A, white arrow). Hampton hump at the right lung base ( A, red arrow). Coronal CT reconstruction shows bilateral central emboli (B, arrows).
Next, we have to look at the right minor fissure, which is visible in the middle of the right lung in about half of PA radiographs. Fissure displacement indicates volume loss in the adjacent lobes. The most common etiologies are endobronchial lesions, fibrotic TB, and bronchiectasis (Fig. 6).
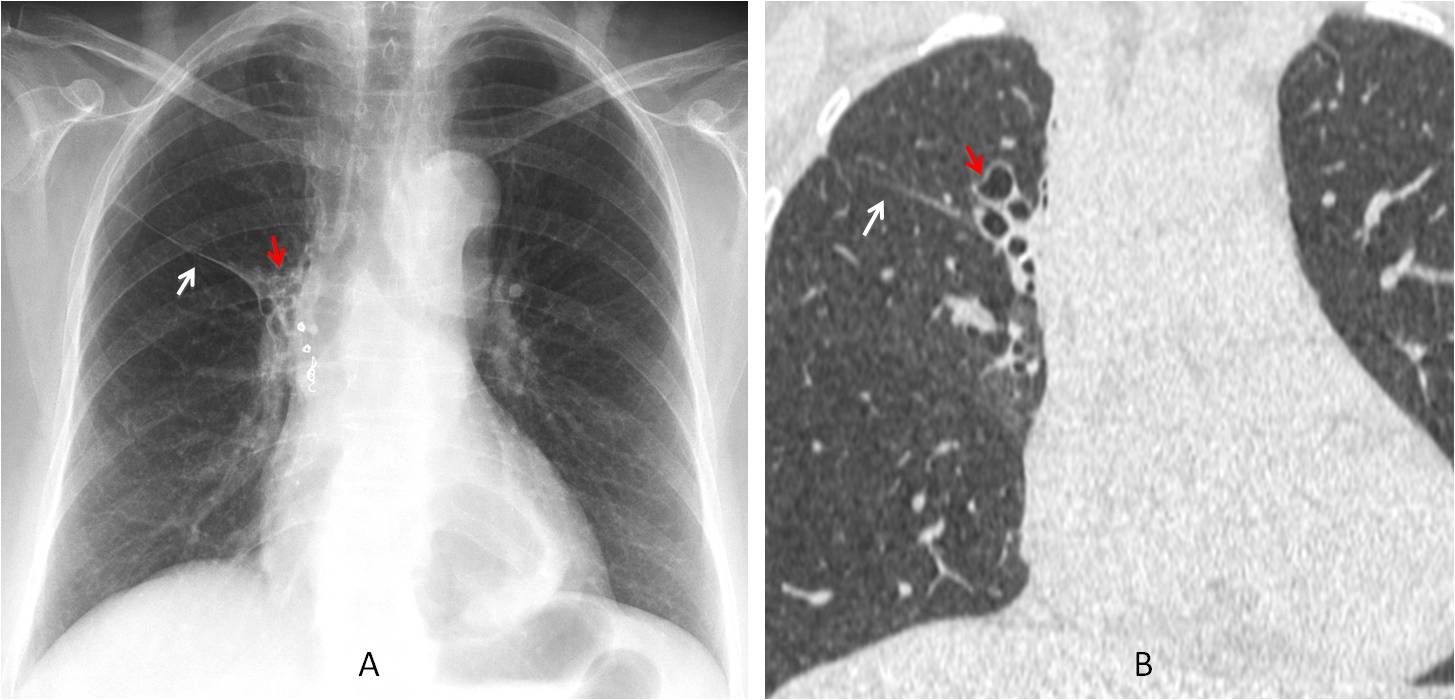
Fig. 6
Fig. 6: Old TB with minor fissure elevation (A and B, white arrows), indicating moderate RUL collapse secondary to previous TB. Bronchiectasis is visible (A and B, red arrows). Metal coils are secondary to embolisation for haemoptysis.
The major fissure is not usually visible on PA radiography. When it is, it is because of medial displacement, which indicates loss of volume of the lower lobe (Fig. 7).
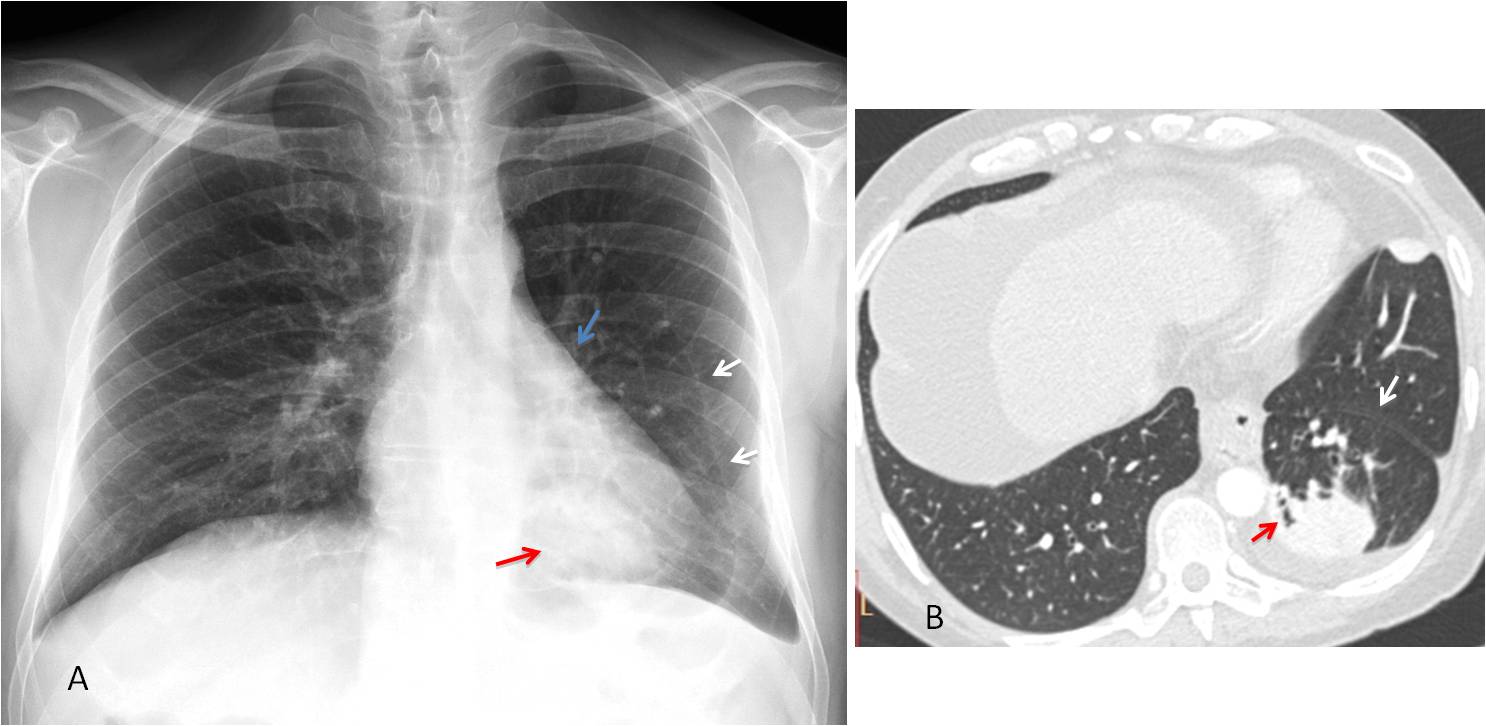
Fig. 7
Fig. 7: Visible left major fissure in the PA radiograph (A, white arrows), with downward displacement of the hilum (A, blue arrow), indicating partial LLL collapse. There is a rounded peripheral opacity in the LLL (A, red arrow). Axial CT confirms displacement of the major fissure (B, white arrow), with pleural thickening and an air bronchogram within the mass (B, red arrow). Diagnosis: rounded atelectasis with loss of LLL volume.
The lung apices should be scrutinised in every PA radiograph. The numerous bone structures in this region can impede visualisation of underlying disease, and missed lesions are not uncommon (Fig. 8).
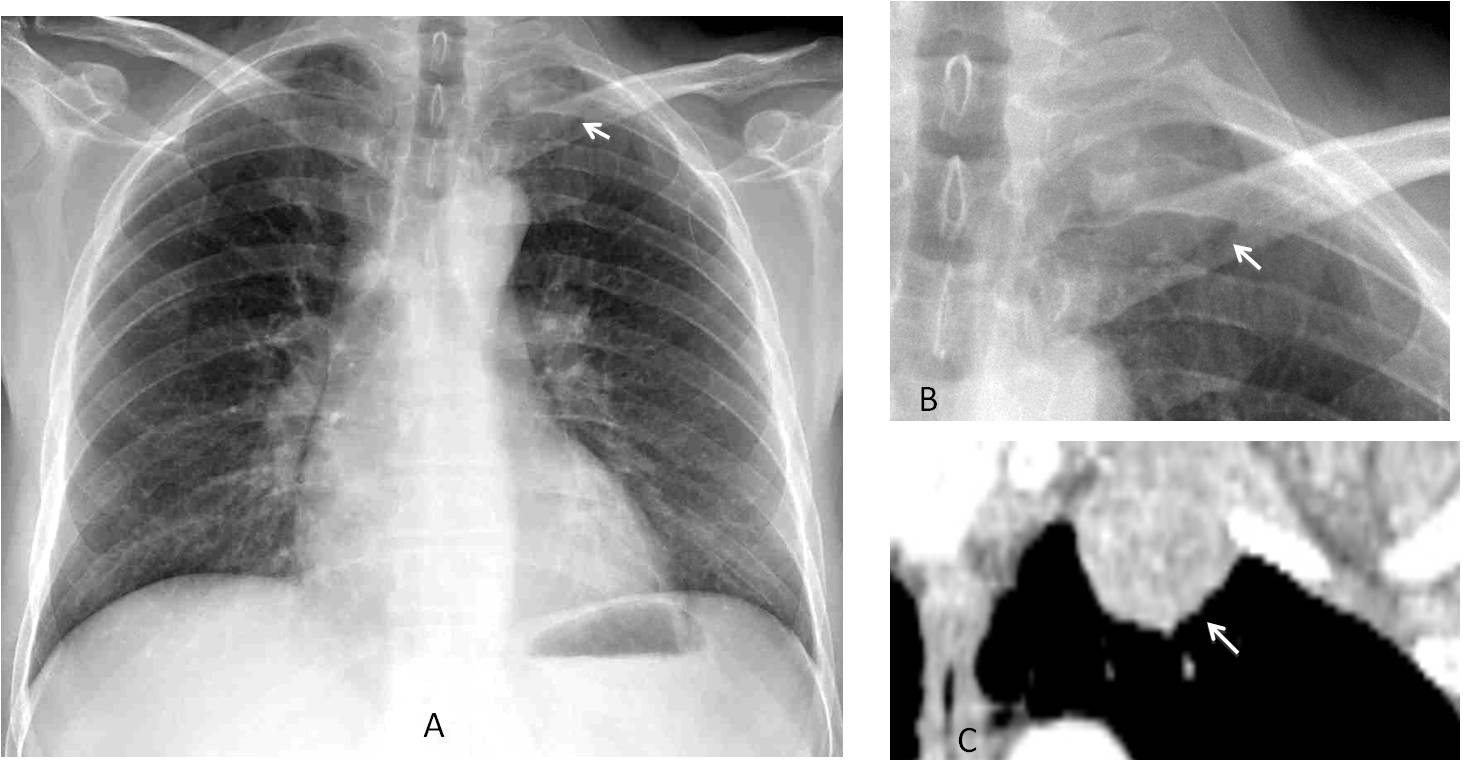
Fig. 8
Fig. 8: 47-year-old man with myasthenia. PA radiograph shows a rounded mass in the left apex (A and B, arrows). The mass was missed, and the chest radiograph was reported as normal. CT performed to investigate myasthenia shows the mass in the left apex (C, arrow). Needle biopsy returned the diagnosis of adenocarcinoma.
Pulmonary nodules are a common presentation of carcinoma, and most occur in the upper lobes. It should not come as a surprise that they are often missed in the initial chest radiograph (Fig. 9). The reported miss rate reaches 60%.
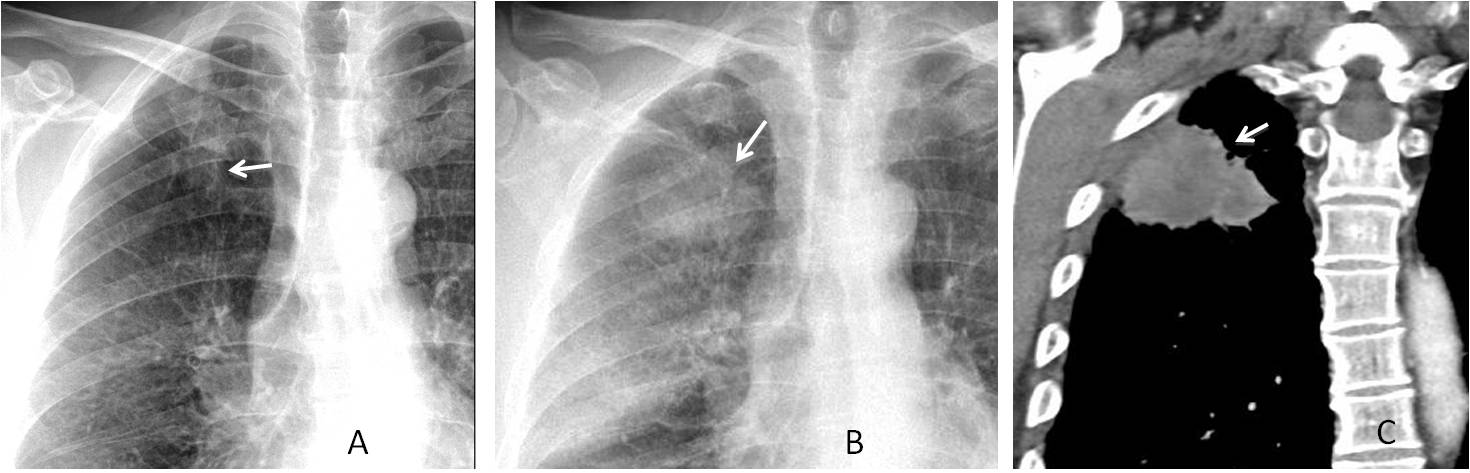
Fig. 9
Fig. 9. Missing a malignant nodule can have dire consequences. Images of a 63-year-old man, in whom a right apical nodule was not seen in 2009 (A, arrow). Radiographs taken two years later show that the nodule has increased markedly in size (B, arrow). CT confirms the findings (C, arrow). Diagnosis: carcinoma with chest wall invasion.
Calcified hypertrophic cartilage at the first costochondral junction should not be confused with a true nodule. They are fairly common in elderly persons and can be recognised by their increased opacity and proximity to the costochondral area. When in doubt, compare with previous films.
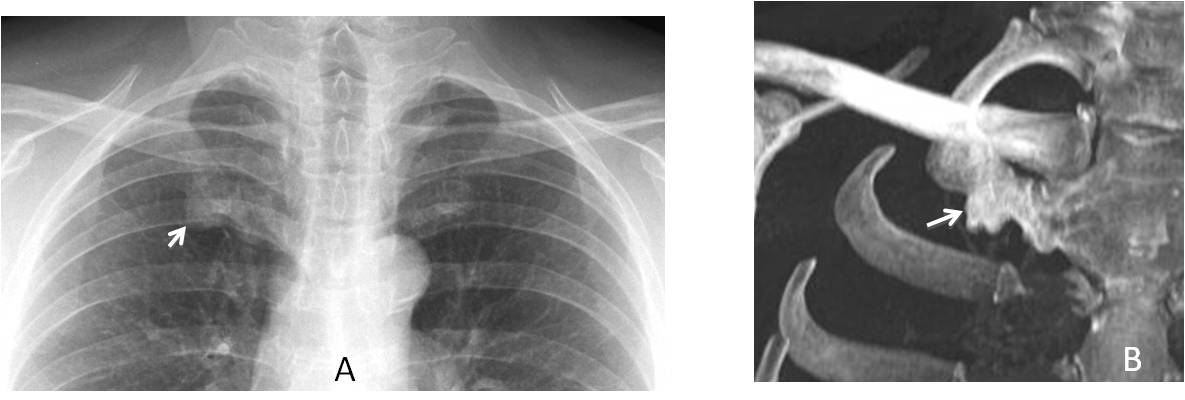
Fig. 10
Fig. 10: Calcified first cartilage simulating an apical nodule (A, arrow). CT confirms the diagnosis (B, arrow).
The last areas to check are the costophrenic sinuses. They are an important landmark because pleural effusion collects there and small amounts of fluid can be missed (Fig. 11).
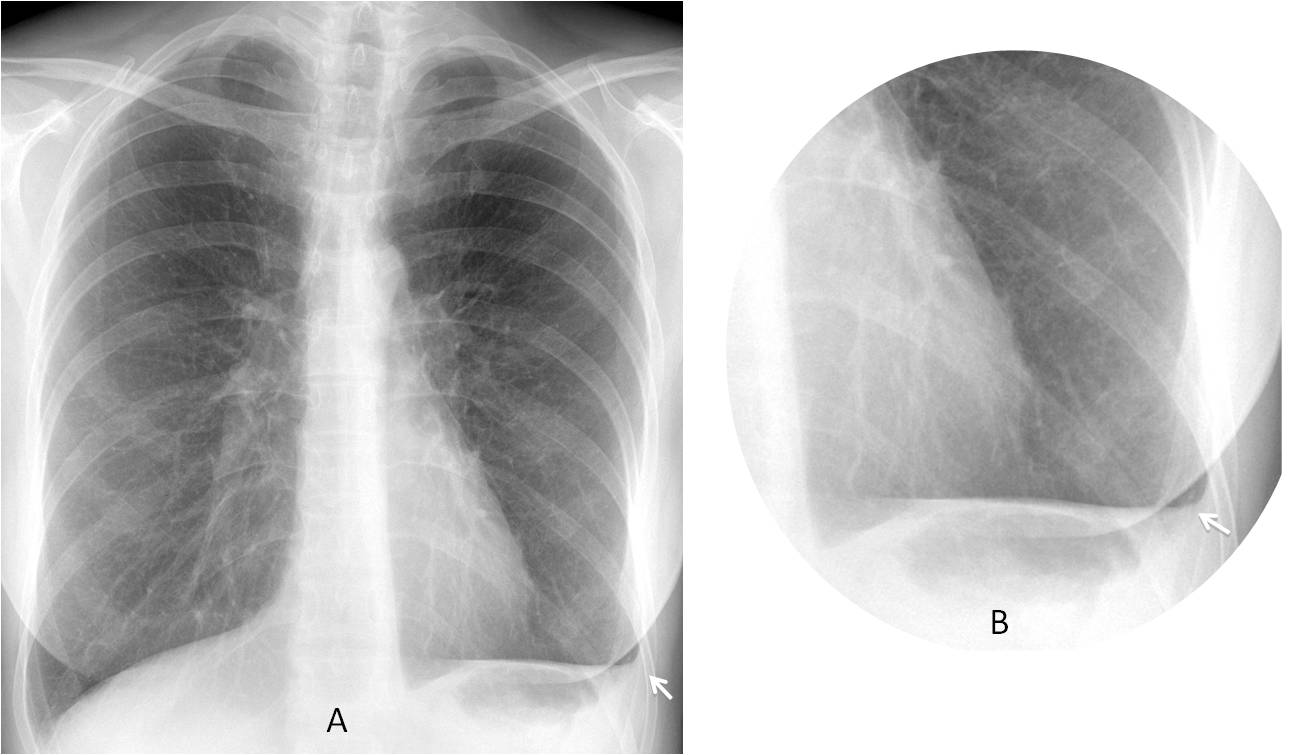
Fig. 11
Fig. 11: 27-year-old woman with blunting of the left costophrenic sinus. Despite the small amount of fluid, a typical concave meniscus can be seen (A and B, arrows).
Occasionally, pulmonary nodules hide in the costophrenic sinus. They may be overlooked unless we specifically examine the sinus, searching for occult disease (Fig. 12).
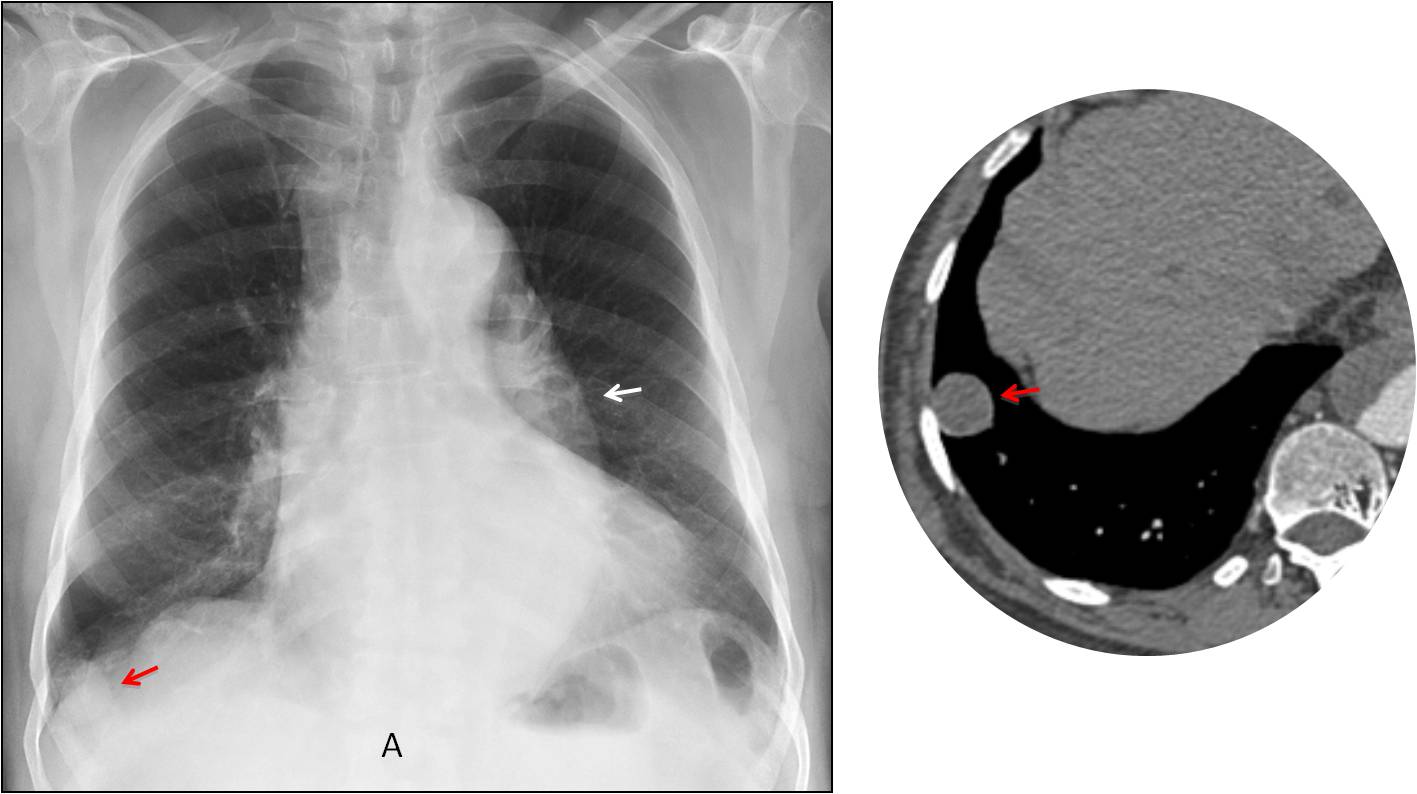
Fig. 12
Fig. 12: 73-year-old patient with suspected aortic dissection. Note the prominent descending aorta (A, white arrow). The nodule located in the right costophrenic sinus was overlooked and discovered on CT (A and B, red arrow).
In conclusion, it is advisable to use checklists to avoid missing abnormalities in the chest radiograph. The following areas should be investigated in the PA view:
The hila, to evaluate changes in position (usually secondary to lobar collapse) and changes in density (caused by neoplasm, lymphadenopathy, or enlarged pulmonary artery).
The minor fissure. Displacement indicates loss of volume of adjacent lobes.
The apices. Nodules in this region are often missed, unless we actively search for them.
The costophrenic sinus, to detect small amounts of pleural fluid and, occasionally, hidden pulmonary nodules.
Next week I will continue with further checklists.

Follow Dr. Pepe’s advice:
1. The use of checklists is of great help to avoid missing subtle findings.
2. The main areas to be scrutinised in the PA radiograph are the hila, right middle fissure, apical region, and costophrenic sinuses.


Hello.
I see two rounded calcifications located in the soft tissues of the right hemithorax, laterally. I also see some linear hyperdensities which seem to be in the periphery of the right lung, lower third. Did this patient undergo any surgery?
No previous surgery
There are some straights metallic opacities in the right soft tissues and proyected over the lung. Is no surgery history we can think about acupuncture needles.
The PA view is poorly inspired with a prominent right hilum, but I can find anything eles in the lung fields. Perhaps we can recomended a high resolution CT for studing the chronic cought Ifara others clínicas causes have been excluded
Sorry, ….CT for studing the chronic cought if others clinical causes have been excluded.
Frío, frío…;-)
Subcutaneous short linear opacities, right chest; queries iatrogenic/ parasitic infection
Mild thoracic spondylosis
Thickened left oblique fissures
Middle lobe atelectasis
right hemitorax
right hemitorax
Les a gradesco mucho por su pagina y los casos son muy interesantes
Les a gradesco por su pagina y sobreto por los casos son muy interesantes
Gracias. I try my best
In my opinion, the left hemithorax is hyperlucent with signs of oligaemia. Asymmetry of hila, structures of left hilum are poorly seen. Maybe some vascular anomaly (for example hypoplasia of left pulmonary artery) or pulmonary embolus. I think also that there are some discrete atelectatic parts of lingula.
Any other cause of hyperlucency?
When i saw only p-a x-ray idea of LLL collapse came to me but no after looking on lateral view. But some atelectases look strange 🙂
You should have followed your first impression 😉
Ok 🙂
Subsegmental collapse in lingula
Additional radiopaque shadow in right lower zone
There is obvious decrease of right hemithorax and the diaphragm relaxation on the right (trauma, e.g. fall in anamnesis or partial lung resection – this could explain metallic shadows on the right)
On lateral view there is thickend pleura in great fissure with the obliteration of anterior sinus also due to pleural thickening – post inflamatory changes?
There is also a tube-like lucent space on the cardiac shadow and is following to the abdomen level – something wrong with esophagus? the early stage of achalasia?
There should be the air in stomach visible on the left side both on PA and lateral view, which in this case is not seen.
I think also about esophageal defect replacement with the part of intestine or possible gastrectomy
There is left retrocardiac opacity, ct is of help for further evaluation.
Come on, you don’t need a CT 😉
Second round:
The left ventricle is increased in size in the PA and Lateral view.
In the lateral view there is a haziness of the anterior clear space, so a dilatation of the ascending aorta will be an option (aortic valve stenosis?). Mayor fissure is thickened.
The right hilum is increased respect to the opposite.
Which one is abnormal, the right or the left hilum?
I think the left is the abnormal
Sd. Swyer-James-McLeod?
To make this diagnosis you need an expiratory film.What if I tell you that no air trapping was present?
I think surgery for right breast cancer and pulmonary changes after radiation.
Another causes of hiperlucency hemithorax without air trapping and surgery history are: pulmonary artery agenesis/hypoplasia, wall chest anomalies, technical rotational factors.
Foreign body without air traping is possible?
Me rindo….
What about compensatory emphysema secondary to lobar collapse?
….stimatissimo Maestro……il problema è a sx, ove il polmone è ipertrasparente perchè in compenso funzionale alla estrema atelettasia del lobo inferiore…profilo cardiaco e diaframma a margini “flou” quale segno indiretto…..
I take my hat off to you…
left hilum is poor, and hypertransparency in left side.
pulmonory left artery atrésia
At this time of the week I have to point out the marked downward displacement of the left hilum, indicative of LLL collapse with compensatory increased lucency of LUL. Congratulations to Genchi Bari for his diagnosis.
Professor, quick question. Is the right hemidiaphragm on the PA an example of eventration? Thanks for the great case 🙂
Elevation of the anterior right hemidiaphragm is not uncommon. I will not call it eventration.
can we call it “hump diaphragm”, and how can we distinguish the hyperlucency from compensation to patient rotation. Thanks, Prof
hypertransparancy in the left side with poor hilum
…..goals !!!!!! Professore son quelli che mancano al Bari…..ancora una prestazione deludente….Il Barca e’ sempre galattico!!!!
Good evening, Dear Doctor.
Right hemithorax with small volume reduction.
left hemithorax is hyperlucent, left hilum is smaller.
We are not able to see the left diafragmae dome( siluette sign). Behid the heart there is visible slight triangle opacity without any particular coresponding changes in lateral view.
I woud say it is LLL collaps with compensatory distension the rest of the left lung parenhyma. The most common cause is tumor, chronic inflamatory changes, foregin body in segmental bronchus.
And what happen with the metallic densities?
Don’t have the foggiest idea! Sometimes you cannot explain everything.
But you should not center in the metallic densities and because of them overlook a descended hilum
Thanks!!!