ECR 2013 Focus: Justifying CT in Paediatric Radiology
The optimisation and justification of procedures is vital when using CT as an imaging modality; particularly on children, who are more sensitive to ionising radiation than adults. Therefore, it is crucial that all those who use CT understand the physics behind the equipment and ultimately use this understanding to minimise the potential risks while maximising the potential benefits to each individual patient. Patients should also be informed of the risks and benefits of undergoing a CT scan. World-renowned experts will explain these issues in detail during a Special Focus Session at ECR 2013.
“Not all radiologists and technicians are aware of the latest dose reduction strategies. Some are not necessarily so well-informed and perhaps do not realise how important this is. We believe that it is a question of trying to get everybody to a certain level of knowledge and expertise,” said Dr. Catherine Owens, paediatric radiologist and CT unit lead at Great Ormond Street Children’s Hospital in London, U.K.
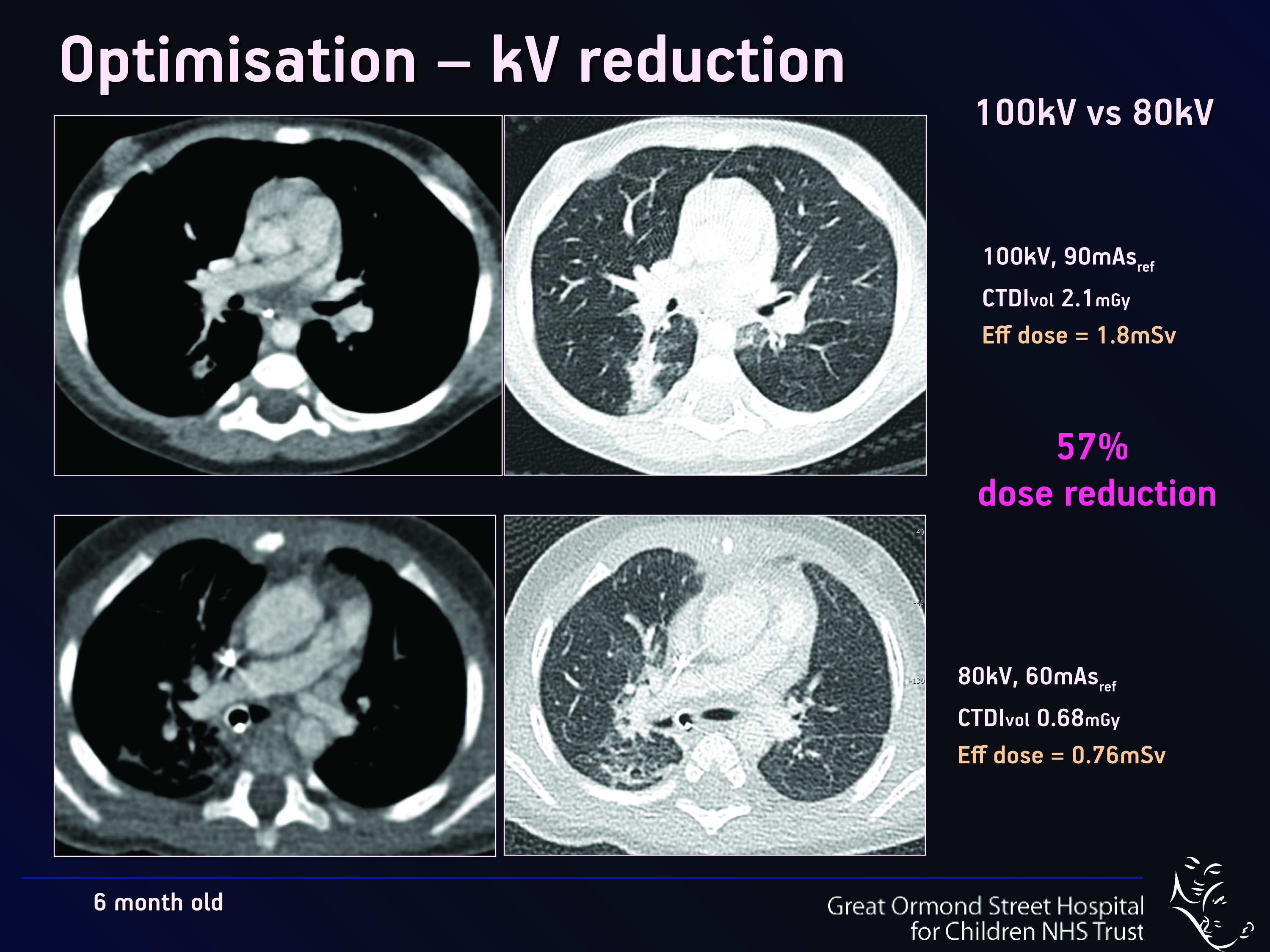
Fig. 1
Each time a patient undergoes a CT scan they are exposed to radiation doses, which can be temporally equated and compared to natural background radiation exposure. This can help to rationalise the levels of radiation exposure for the patient and referring clinician, and put them into a more intelligible format for the public. In the U.K., the average effective natural background radiation dose is 2.5 mSv per year. In adolescents, a CT scan of the chest can subject the patient to a similar dose, but CT protocols are so variable that a patient of similar size can be subjected to ten times that dose, depending on what type of CT protocol is being used, especially when the technician who performs the examination does not have adequate knowledge of CT dose reduction techniques.
“There are many tips and tricks which can be implemented to help decrease radiation dose without loss of diagnostic images, which must be ‘fit for purpose’,” said Owens, who will chair the session.
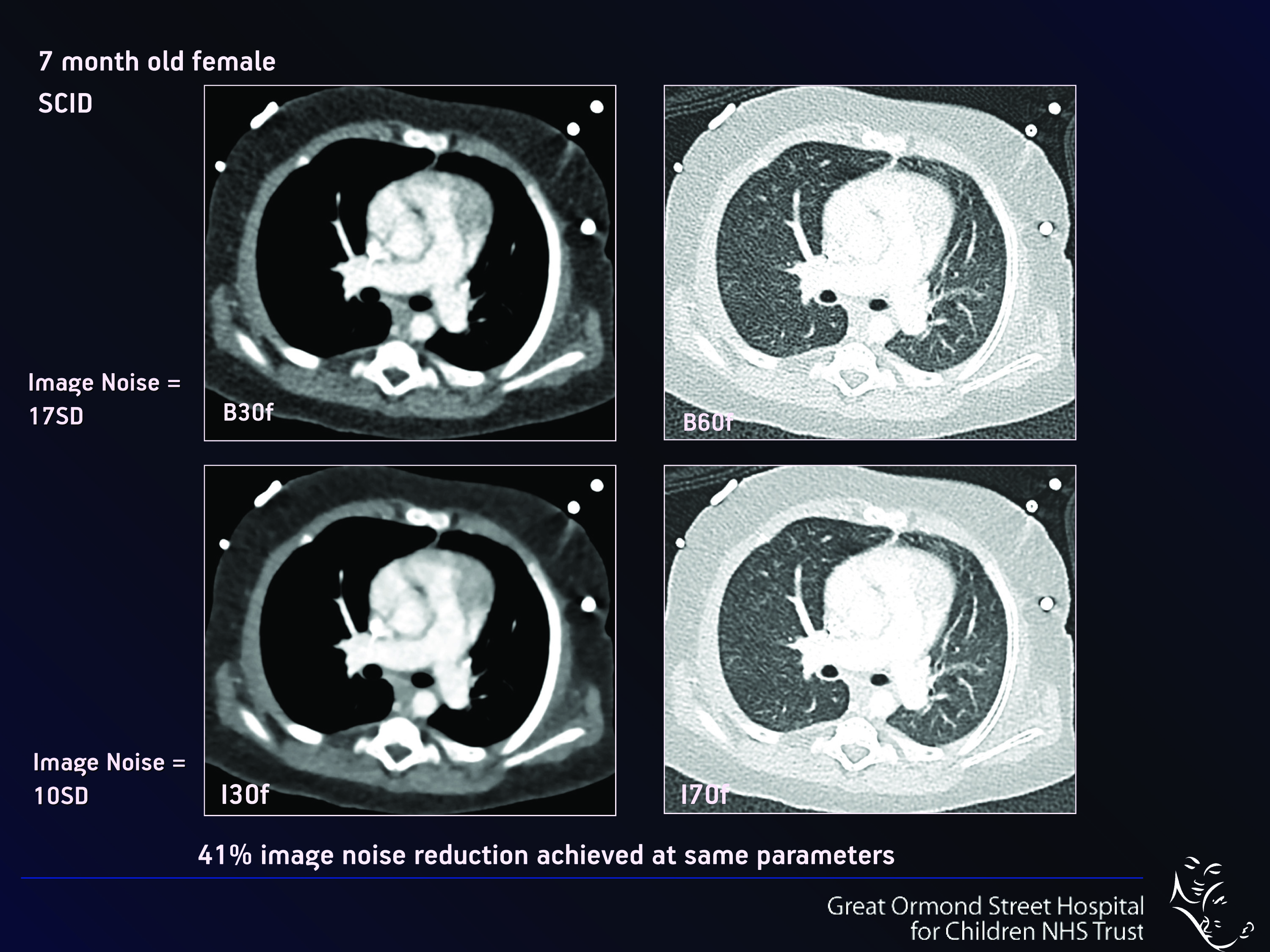
Lowering scan operating parameters such as kilovoltage (kVp – Fig.1), current and exposure time (mAs – Fig. 2) significantly reduces the dose to the patient. “Normally if you reduce the dose, the picture quality may not be so attractive initially, as the images become more ‘noisy’. But with CT you can manipulate even noisy images on the computer afterwards, in order to enhance their diagnostic quality so that they are indeed diagnostic or ‘fit for purpose’,” she said.
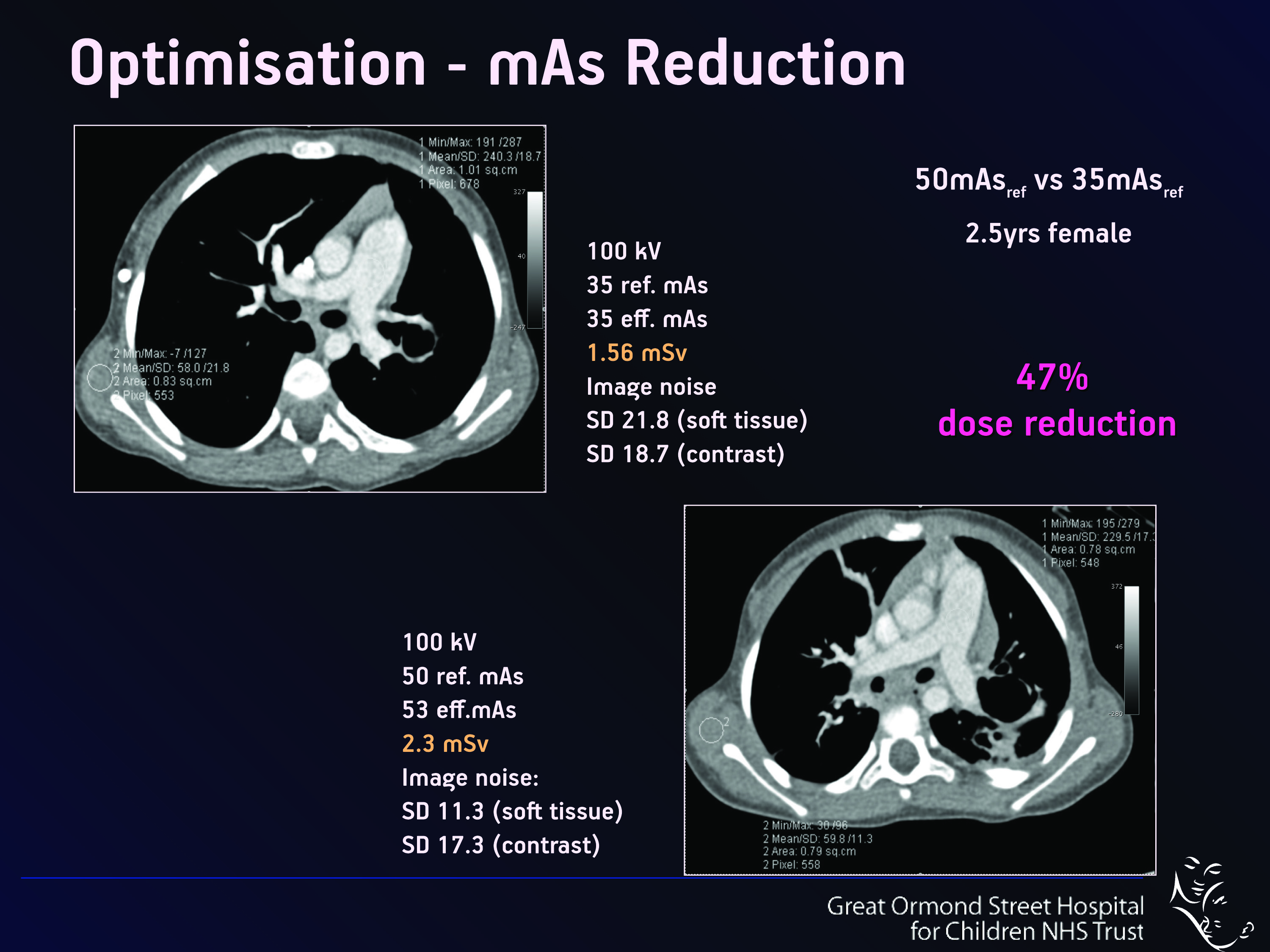
Fig. 2
Many new developments and improvements in the equipment used can help to reduce the effective dose, such as the use of more efficient detectors and special mechanical cones, to reduce overbeaming and overscanning, and the use of post-processing techniques such as mathematical iterative reconstruction. The use of ever thinner collimation in combination with more efficient detectors, which later reduces the background noise, particularly at low doses, also helps to decrease dose. But even with optimised protocols, a CT examination must always be clinically justified for each patient.
Paediatric CT examinations are still relatively rare outside of specialist centres, as radiologists try to avoid them in favour of non-ionising radiation techniques such as ultrasound or MRI. “In my hospital we do many more ultrasound and MRI examinations than we do CT. There are not many reasons to perform CT on new-borns, as ultrasound and echocardiography are often sufficient for diagnosis outside of some more complex congenital cardiothoracic and neurological disorders,” Owens said.
Cardiac imaging is one instance where CT can be an alternative for children, when electrocardiogram proves inconclusive. CT provides very fast and detailed images of the extracardiac thoracic anatomy while using very small contrast doses with low radiation doses of less than 1 mSv, which is equivalent to less than four months of background radiation.
“In my centre, with the equivalent of about two to three months of background radiation, we acquire superb diagnostic images on a tiny baby in a very short time, which are diagnostic and alter the patient’s clinical management in many cases. Approximately 40% of the CT examinations we do in children are acquired for anatomical mapping of the cardiothoracic structures,” Owens said. CT shows some areas of the heart that are difficult to see on the US electrocardiogram because of its proximity to the lungs. Imaging a major vessel that originates in the heart and goes into the neck can, for instance, be difficult with US because of the presence of air within the lungs, which does not conduct sound well.
Echocardiography cannot always answer questions related to structures that are connected to the heart. Intracardiac anatomy is better shown by echocardiography, while CT offers great insight into the extracardiac anatomy and the relationship of the blood vessels and the heart with the lungs and trachea. These structures can sometimes be affected badly in children with heart disease, contributing to their clinical distress, by making them very breathless for instance. “CT exquisitely images the combination of cardiac and tracheobronchial disease as the gold standard images,” Owens said.
Another advantage of CT is its wide availability in most developed countries, whereas MRI access is still limited and waiting lists are long. Moreover, MRI is challenging to use in children because it is time consuming and requires a long period of time in the scanner (30–60 minutes compared to less than 10 seconds for CT). “In children who won’t lie still for long you need to sedate or give them a general anaesthetic (GA). In patients aged between one to four years especially, sedation or GA clearly has an inherent risk. Sometimes children are deemed by the anaesthetist to be too sick to undergo a GA or sedation for an imaging procedure,” she said.
In short, radiologists should always question the need and clinical advantages for the patient to undergo any exam which uses ionising radiation. The procedure must be ‘justified’. If there is an alternative imaging technique which does not use ionising radiation, such as US or MRI, this may be the best option. In many cases MRI scanning may yield better information than CT. Professor Michel Claudon, from Nancy University Hospital in France, will focus on this topic during the ECR session. Whatever the modality, the objective for radiologists remains the same: to produce the best possible pictures to facilitate treatment and provide a roadmap, particularly for surgeons.
“Surgeons like to have a clear picture of the patient’s anatomy and pathology before they operate. They like to have all the information in advance, like a roadmap, and the last thing they want is to find something unexpected. They prefer to tell the patients and their families exactly what they plan to do. We, as radiologists, can give them advance warning with excellent quality reconstructed images in various different planes, so that they can then operate via tiny incisions, i.e. keyhole surgery, with smaller scars and enhanced speedy postoperative recovery times,” Owens explained.
The role of radiologists extends beyond that, she believes. Together with the medical team, they have to speak for children and make sure that their interests are represented, especially when it comes to deciding on optimal imaging techniques for the patients’ diagnostic pathway.
“Different working groups know things about radiation: physicists know the theory, manufacturers know how to put the theory into the building of a machine and radiologists know how best to use the technology in a patient-focused clinical setting. We all need to work together to optimise all the knowledge we have in order to get the best outcome for the patient. The pitfalls are that everyone works in their own world, and they don’t necessarily share all the relevant information. We have to identify and understand our common vision and goal, and work together to try to achieve it. We should also try to encourage manufacturers to be very honest about what their scanners deliver,” she said.
Most machines are designed for adults, who make up the majority of patients as not so many children undergo CT, so companies do not focus on the minority market. “Children can’t speak for themselves, so radiologists must speak up for them, and unite with other disciplines to provide the best child/patient-focused care. That is our duty at the end of the day,” added Owens.
Special Focus Session
Friday, March 8, 08:30–10:00
SF 4b: Justifying CT in paediatric radiology


This article previously appeared in the ECR 2013 Preliminary Programme
All images provided by Dr. Catherine Owens.


Hi,
Thanks for sharing this information. There are some conferences happening in which medical specialty would be “Pediatric Radiology” and here is one of those conferences the conference details are given below.
Penn Radiology CME is Organizing Pearls, Pitfalls & Protocols: Spring Imaging Update 2020 held from Mar 23 – 27, 2020 at Lake Buena Vista, Florida, USA.
Source: https://www.emedevents.com/c/medical-conferences-2020/pearls-pitfalls-and-protocols-spring-imaging-update/