
B-0169 High-resolution computed tomography (HRCT) of the lungs in brain dead pigs: a feasibility study
G. Bozovic, S. Steen, T. Sjöberg, C. Schaefer-Prokop, J. Verschakelen, Q. Liao, R. Siemund, I. Björkman-Burtscher | Thursday, March 7, 14:00 – 15:30 / Room D1
Purpose: Brain death has adverse effects on lung perfusion and ventilation with possible damage of lung parenchyma pre-transplantation. We wanted to assess brain dead subjects treated with a new drug regime with HRCT as a pre-transplant work-up.
Methods and Materials: Eleven pigs were decapitated (DC) assuring brain death, attached to ventilator and treated with a new drug regime optimising circulation thereby preventing lung edema. Thirteen non-decapitated pigs (N-DC) attached to ventilator, supported with conventional treatment served as controls. All were monitored 24h and thereafter examined with chest HRCT. Images were analysed by two radiologists using a pre-defined questionnaire assessing parenchymal and airway changes. In consensus, an overall conclusion inferred presence of edema, infection/atelectasis or airway pathology. Severity was estimated with a subjective scale.
Results: After 24h there were no significant differences between the groups regarding mean arterial pressure (MAP), arterial oxygen/fraction of inspired oxygen (PaO2/FiO2), amount of infused fluid, urine production or clinical signs of edema. Both groups showed parenchymal changes in a comparable extent (consolidation in 6/11 (DC) and 10/13 (N-DC) and GGO in 6/11 (DC) and 9/13 (N-DC), respectively). Overall conclusion appraised the presence of oedema in 2/11 (DC) but none of the N-DC pigs, signs of old/ recent infection in 6/11 (DC) and 7/13 (N-DC) and possible hypersensitive pneumonitis in 1/13 (N-DC).
Conclusion: After 24h, there were no significant differences in clinical and imaging findings between the groups supporting the successful hemodynamic optimising with the new drug regime. HRCT allows evaluation of pre-transplant lungs.

B-0232 Detection of HCC and liver metastases with BR14: final results of a multicentre phase IIA study
J. Hohmann, A. Müller, J. Skrok, K.-J. Wolf, A. Martegani, C.F. Dietrich, T. Albrecht | Thursday, March 7, 14:00 – 15:30 / Room I/K
Purpose: The study was primarily designed to find the optimal dose range of BR14 to detect malignant focal liver lesions. Secondary objectives were the evaluation of the safety profile and comparison with contrast-enhanced MRI (CE MRI).
Methods and Materials: 25 patients (9f, 16m, mean age: 66y) with known HCC or liver metastases were examined in three centres during a time period of three months. Each patient underwent a baseline and at least three contrast-enhanced US (CEUS) with ascending dose levels (0.25ml, 1.0ml, 4.0ml) of BR14. CE MRI was done 4 weeks prior or post-study examination. Lesions were recorded in on a liver map, with respect to localisation, size and suggested lesion type. Examination quality was documented and safety parameters were assessed.
Results: The number of lesions detected with BR14 CEUS increased with dose, while the number of missed lesions and the lesion size decreased. Despite the increasing contrast enhancement no other image quality parameter showed a substantial difference. No significant changes were found for the analysed safety parameters and no serious adverse events were reported.
Conclusion: We finally conclude that the recommended dose level of BR14 is between 1.0 ml and 4.0 ml for which the lesion detection was comparable to the CE MRI. In addition, we found a higher number of especially small lesions with higher doses of BR14 which might be due to a higher sensitivity of CEUS for the detection of liver metastases. However, this is an interesting and debatable finding.
Dear Friends,
Our next case is that of a 60-year-old male with intermittent chest pain for the last year. If it is of any help, Muppet made the wrong diagnosis in this case. His mind was probably still in Mexico.
What do you see? What would be your diagnosis? Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
Read more…

A-083 Bon appétit! Starters”: cystic fibrosis, pneumonia and pulmonary embolism
M.U. Puderbach | Friday, March 8, 08:30 – 10:00 / Room F2
CF: MRI is comparable to CT with regard to the detection of relevant morphological changes in the CF lung. Compared to CT, the strength of MRI is the additional assessment of “function”, i.e. perfusion, pulmonary haemodynamics and ventilation. In CF, regional ventilatory defects cause changes in regional lung perfusion due to the hypoxic vasoconstriction response or tissue destruction. Using dynamic contrast-enhanced MRI, these perfusion changes can be assessed. Pulmonary embolism: The current imaging reference technique in evaluation of acute pulmonary embolism is helical computed tomography. To be competitive with CT, an abbreviated MR protocol focusing on lung vessel imaging and lung perfusion may be accomplished within 15 min in-room time. As a first step, a steady-state GRE sequence acquired in two or three planes during free breathing enables a non-contrast-enhanced detection of large central emboli. As a second step, the protocol continues with the contrast-enhanced steps including first pass perfusion imaging, high spatial resolution contrast-enhanced (CE) MRA and a final acquisition with a volumetric interpolated 3D FLASH sequence in transverse orientation. Pneumonia: The potential of MRI to replace chest radiography, particularly in children, was already investigated several years ago. The experience from this work may be considered valid for the suggested protocols for 1.5-T scanners since image quality has significantly improved. Therefore, T2-weighted fat-suppressed as well as dynamic contrast-enhanced T1-GRE sequences are applied with a slice thickness between 5 and 6 mm. Disease entities encompassing community-acquired pneumonia, empyema, fungal infections and chronic bronchitis are detectable.

A-205 Can non-invasive techniques as CTA and MRA replace catheter angio for diagnostic work-up?
L. van den Hauwe, M. Voormolen, T. van der Zijden, R. Salgado, J. Van Goethem, P.M. Parizel | Saturday, March 9, 08:30 – 10:00 / Room B
Although catheter angiography remains the gold standard for cerebrovascular imaging, in recent years, it has been replaced to some extent by less-invasive techniques, such as CTA, MRA, and ultrasound. Some of these techniques allow for cerebrovascular imaging without exposure to ionizing radiation, and/or without requiring an exogenous contrast agent that could cause nephrotoxicity, allergic reaction, or other adverse effects. Moreover, all of these techniques avoid the extra time, expense, and possibility of complications that are associated with arterial catheterization. Ongoing developments in CT- and MR-based angiography continue to improve the effectiveness of these techniques, and to expand the clinical roles that they can fulfill. Nowadays, these noninvasive techniques not only provide images with high spatial resolution, but also offer time-resolved images, in which arterial and venous phases can be distinguished, and can provide selective visualization of vessels supplied by a single supplying artery. This presentation will review the latest developments in CT- and MR-based cerebral angiography, and illustrate the use of these CT- and MR-techniques in the diagnosis of cerebral aneurysms and vascular malformations.

A-329 Role of imaging in personalised therapy monitoring
A.R. Padhani | Saturday, March 9, 16:00 – 17:30 / Room F2
Many imaging biomarkers have emerged which individually or collectively provide unique information on tumour behaviour including response to treatment. There are several requirements that must be met before imaging biomarker(s) can be considered as being able to direct a person’s management. First, the biomarker should have a known biologic basis with a recognised method for quantification and to be adequately validated. With regard to the latter, it is important that the biomarker reports on/measures biologically meaningful cellular/tissue process such as reporting on cell death, on angiogenesis, proliferation and metabolic shutdown NOT simply conveying information on receptor occupancy or down regulation of pathways that may or may not be important. Data acquisition procedures should have been optimised and the test’s performance should have been established. The level of change in the imaging biomarker that can be considered as real should be known (that is, the measurement error). Reproducibility needs to have been determined by appropriately powered test-retest studies. Imaging biomarkers can only be useful if they can detect biologically meaningful effects directly related to treatments (that is, magnitude of biological effects detected must be greater than the reproducibility/measurement error) at appropriate time points to be able to effect patient management. Finally, it must be know how much therapy-induced change is meaningful in terms of patient benefit in terms of hard clinical endpoints such as surgical resectability, organ preservation, progression free and overall survival, etc. These aspects will be considered in detail using practical examples.
In the build up to ECR 2014, we will be showcasing a few of the optical illusions cases which will be presented in the interlude of ECR 2014’s new Case-based Diagnosis Training session. Our first case, below, was submitted by Dutch neuroradiologist, Dr. A. A. Jacobi-Postma. The picture shows a patient with a non-functioning macro-adenoma, but it looks a little like something else.
What do you see? Leave your illusion interpretation as a comment.
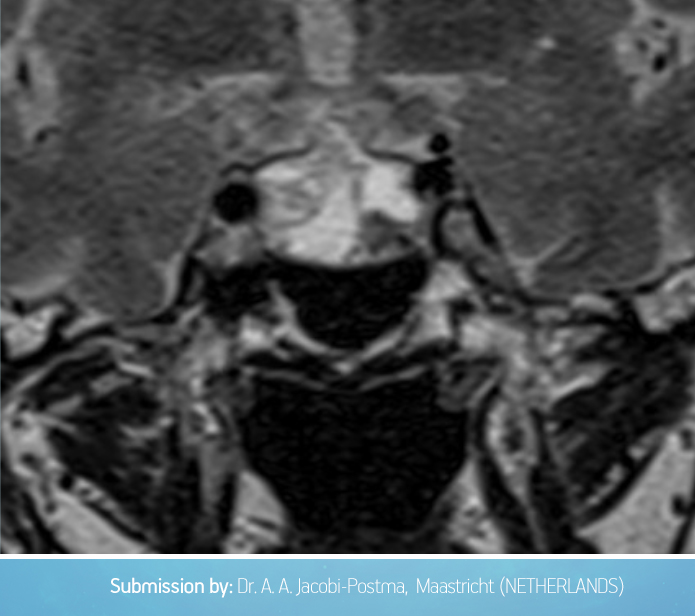
Stop by the session at the congress on Monday, March 10, or come back to the blog in a few days to see if your interpretation matches Dr. Jacobi-Postma’s.

B-0403 MR spectroscopy in mild and moderate cognitive impairment as illness outcome predictor: preliminary experience
J. Forner Giner, A. Alberich-Bayarri, G. Garcia Marti, A. Pomar-Nadal, J. Rayón-Aledo, L. Martí-Bonmatí | Friday, March 8, 14:00 – 15:30 / Room B
Purpose: To evaluate Alzheimer’s disease premature diagnosis based on spectroscopy MRI.
Methods and Materials: We carried out a prospective study on 178 patients (116 women and 62 men) whose ages ranged 27 to 68 years (mean age 65 ± 12). Every patient presented mild or moderate cognitive impairment according to Reisberg score (3-4 grade). Standard brain MR and spectroscopy brain MR were performed using a 3 T intensity MRI device (Archieva TX, Philips Healthcare, Best, The Netherlands). Spectroscopy MR was focused in posterior parietal and frontal lobes gray substance using a unique volume (20 x 20 x 15 mm) and two different echo-times, TE (32 and 136). Morphology and volume of temporal lobes were evaluated through FLAIR coronal images which were used to quantify temporal horn width and so classify patients in four groups. JMRUI (Java Magnetic Resonance User Interface) was used to calculate quantitative parameters in MR spectroscopy. MR was used to measure: calculation of NAA (N-acetyl aspartate), Cr (creatinine), Cho (choline) and mI (myo-inositol) metabolites ratios. We used analysis of variance to compare metabolite ratios between the different patient groups previously defined.
Results: We found significant differences (p ≤ 0,05) between groups in NAA/Cho concentration (p=0,022), both in long and in short eco times and frontal and parietal anatomical regions. No other significant differences between groups were found.
Conclusion: MR spectroscopy could increase efficiency in Alzheimer’s disease premature diagnosis as well as turning out to be a useful additional tool for the clinician next to clinical history.

Dear Friends,
I am back with radiographs of a 63-year-old woman with malaise and low-grade fever. Check the images below and leave me your thoughts and diagnosis in the comments section. Come back on Friday for the answer.
Diagnosis:
1. Carcinoma of the lung
2. Pneumonia
3. Thymoma
4. None of the above
Read more…
