
A-508 Clinical aspects of computer aided detection and diagnosis in DBT
H.-P. Chan | Sunday, March 10, 16:00 – 17:30 / Room F2
Digital breast tomosynthesis (DBT) can potentially increase the sensitivity and reduce recall rate in breast cancer screening. However, the chance of oversight may not be negligible because of the very large search space (~50-80 slices per view) and the increased workload and possibly fatigue to the radiologists. CAD has been shown to reduce radiologists’ false negatives in screening mammography. It can be expected that CAD may be useful for DBT interpretation. DBT in clinical use is still at an early stage. Although the impact of CAD on DBT interpretation has not been reported, some important issues associated with CAD use can be expected based on the experiences in screening mammography. In this talk, the potential usefulness of CAD in DBT and the issues as observed from the reported prospective studies of CAD use in the clinic will be discussed, including the potential impact of off-label use (i.e., CAD systems approved as second reader used as concurrent or first reader), user training, and quality assurance of CAD performance. Because of the increased reading time for DBT, there will be an even stronger tendency that radiologists may want to use CAD as a concurrent or even first reader to improve workflow. To have a CAD system for such intended use, much more stringent requirements for the standalone performance of the CAD system and properly designed studies to evaluate its impact as a concurrent or first reader should be required before the CAD system can be approved for clinical use with DBT.
Dear friends,
This week Muppet and I are going on a dangerous trip abroad. Forgive me if I answer your comments a little bit later than usual; the locals may be hostile and refuse to share their WiFi.
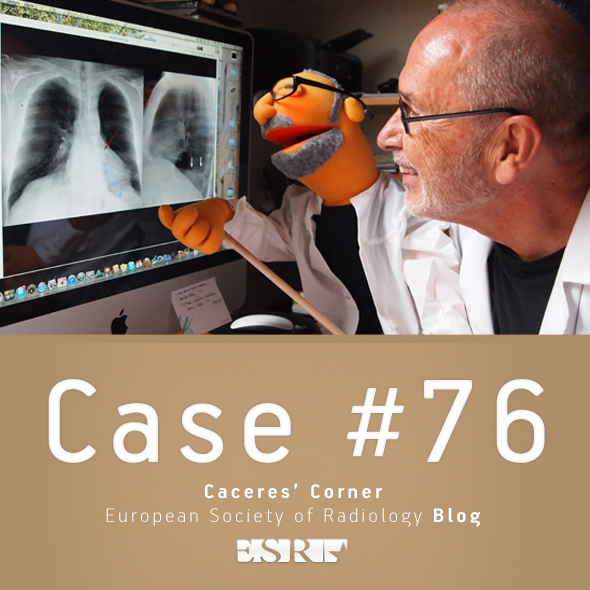
Radiographs belong to a 73 y.o. male with fever and symptoms of acute prostatitis.
How do you interpret the chest findings?
Read more…

A-153 CEST (chemical exchange saturation transfer)
B. Schmitt | Friday, March 8, 16:00 – 17:30 / Room C
CEST imaging in principle relies on the chemical exchange of protons bound to solute molecules and surrounding bulk water molecules. The effect can be used for MRI because the magnetization of each solute proton, is also transferred to bulk water, and can thus be visualized via the MR signal. CEST effects can be evaluated for specific molecular groups due to their characteristic proton resonance frequencies, which provides the technique with a high intrinsic sensitivity to these groups. In healthy cartilage tissue, strong CEST effects from exchangeable protons of glycosaminoglycan (GAG) molecules can be observed. The magnitude of these effects decreases when concentration ratio between bulk water protons and GAG protons decreases, e.g. in the early stages of osteoarthritis (OA). Initial studies on patients after cartilage repair surgery with GAG-dependent CEST (gagCEST) imaging have demonstrated that it is feasible to visualize GAG loss in vivo at 7.0 Tesla. Initial reports also claim that the technique might be transitioned to the clinical field strength of 3 T. Although CEST imaging can be performed with standard clinical equipment and protocols can easily be implemented in a routine clinical workflow, the signal analysis in gagCEST imaging and the reading of gagCEST images are technically complex. For example, effects, which alter the T2 relaxation time of tissue such as high relative water concentration, can affect the magnitude of gagCEST effects although the absolute concentration of GAG is unchanged. Unless confounding effects are automatically corrected, careful analysis of images is necessary for proper interpretation of results.

B-0215 Ultrasound elastography in the diagnostic assessment of axillary lymph nodes in women presenting to a breast imaging centre
L. Sim, L. Leong | Thursday, March 7, 14:00 – 15:30 / Room F2
Purpose: To evaluate the performance of elastography in distinguishing benign and metastatic axillary lymph nodes.
Methods and Materials: 67 women with 72 sonographically visible axillary lymph nodes undergoing biopsy at our breast imaging centre were evaluated independently with conventional ultrasound, elastography and combined ultrasound and elastography (CEUS). The elastogram was classified as benign or malignant, based on the strain pattern, the length and area ratios of the lesion seen on elastography versus ultrasound. Validation of radiological diagnosis was by histopathology. The sensitivity, specificity, PPV, NPV and accuracy of each test were compared individually and with CEUS. To obtain a parameter for diagnostic performance, ROC curves were plotted.
Results: Of the 72 axillary lymph nodes biopsied, 33 had metastases and 39 were benign. The sensitivity, specificity and accuracy of conventional ultrasound were 93.9%, 30.8% and 59.7%, respectively. The sensitivity, specificity and accuracy of elastography were 93.9%, 97.4% and 95.8%, respectively, and that of combined ultrasound and elastography were 97 %, 92.3% and 94.4%, respectively. The sensitivities of all 3 tests were similar but the specificity and accuracy obtained by elastography and CEUS were significantly better than conventional ultrasound (P<0.0005). Elastography correctly diagnosed 96 % of histologically benign lymph nodes which were deemed malignant on ultrasound.
Conclusion: The use of elastography alone or combined with ultrasound has a higher specificity and accuracy than conventional ultrasound in evaluating axillary lymph nodes. Given the high specificity of elastography, biopsy could have been avoided in 96 % of cases classified as malignant on ultrasound but benign on elastography.
Dear Friends,
To continue reviewing basic chest patterns, I present the case of a 52-year-old man with a solitary pulmonary nodule.
Diagnosis:
1. Probably malignant
2. Probably benign
3. Indeterminate
4. Need previous films
Check the images below, leave your thoughts and conclusion in the comments section and come back on Friday for the answer.
Read more…

A-349 B. MDCT in a patient with small bowel ischaemia
S. Romano | Sunday, March 10, 08:30 – 10:00 / Room B
Intestinal ischaemia and infarction are important causes of acute abdominal disease which appropriate diagnosis has to be as more as accurate being of crucial importance for the surgical or medical managament of the affected patients. At the basis of an efficient report lays the deep knowledge of the patho-physiologic mechanism leading to arterial, venous or low-flow state vascular injury of the intestines. When the mechanism is clearly understood, from a radiological point of view, it is essential to know how to optimise the MDCT technique in case of suspected intestinal ischaemia and what are main findings and intestinal features of the injured intestine. A further step is represented from the differentiation of various stages of disease from early potential transient ischemia to late infarction. However, it is also strongly important to become familiar with the reperfusion damage of the intestine, frequently observed but as still as a challenge for an effective diagnosis. The accuracy of the various radiological signs of bowel ischaemia should be considered and discussed, whereas presentation of several clinical cases with the description of their respective reports and final diagnosis still represents the “key” to improve an effective diagnosis of intestinal ischemia in daily radiological practise.

B-0120 Determining the vulnerable plaque: correlation between 18F-FDG PET and dynamic contrast-enhanced MRI in atherosclerotic plaques of symptomatic patients
M.T.B. Truijman, R.M. Kwee, R.H.M. van Hoof, R.J. van Oostenbrugge, W.H. Mess, J.E. Wildberger, W.H. Backes, J.A. Bucerius, M.E. Kooi | Thursday, March 7, 10:30 – 12:00 / Room N/O
Purpose: Identifying vulnerable atherosclerotic plaques in symptomatic patients with moderate (30-69%) carotid artery stenosis can contribute to clinical decision making. Hallmarks of plaque vulnerability are inflammation and increased neovascularisation. Inflammation can be assessed with 18F-FDG PET, while neovascularisation can be quantified with dynamic contrast-enhanced (DCE) MRI. We aimed to investigate the correlation between inflammation as assessed by18F-FDG PET and neovascularisation as assessed by DCE-MRI.
Methods and Materials: Fifty-eight patients with transient ischaemic attack (TIA) or minor stroke in the carotid territory and ipsilateral carotid plaque causing a moderate stenosis were included. All patients underwent 1.5 T multi-sequence MR imaging. Quantification of neovascularisation was done using a custom-made Matlab program which calculates Ktrans. A 3D PET-CT scan was performed on all patients one hour after injection of 2.75 MBq/kg body weight 18F-FDG. Dedicated fusion software was used to calculate mean blood-normalised 18F-FDG standard uptake values (SUV) of the plaque.
Results: Of the 58 patients, 9 were excluded due to poor image quality of the DCE-MRI. In total, we analysed 49 patients. The mean Ktrans and mean normalised SUV were 0.110 (±0.027) and 1.446 (±0.255), respectively. We found a weak but significant positive correlation between the mean normalised SUV and the meanKtrans (Spearman’s r=0.302, p=0.035).
Conclusion: There is a weak but significant positive correlation between Ktrans, which is a marker for neovascularisation and SUV, which is a marker for inflammation. Future studies are warranted to investigate whether DCE-MRI and/or 18F-FDG PET can be used to predict cerebrovascular events.
Dear Friends,
The Muppet is very happy with your responses to the previous case. As a prize, he wants to show you the following case that we saw together this July before he went on vacation with Miss Piggy (and left me working). Radiographs belong to a 46-year-old woman, with pain in the chest.
Leave your thoughts and diagnosis in the comments section below, and come back on Friday for the answer.
Diagnosis:
1. Empyema necessitatis
2. Chest wall tumour
3. Metastatic disease
4. None of the above
Read more…

B-0627 Additional value of diffusion-weighted (DWI) MRI for predicting complete tumour response (T0N0) in rectal cancer treated with neo-adjuvant chemoradiation therapy (CRT)
S. Sassen, M. de Booij, M.N. Sosef, G. Lammering, C.M.M. Bakker, R. Clarijs, R.C.M. Berendsen, J. Wals, R.F.A. Vliegen | Sunday, March 10, 10:30 – 12:00 / Room A
Purpose: Patients with complete response (CR) after CRT might be considered for less aggressive treatment like a wait-and-see strategy. Few studies investigated the value of DWI-MRI for predicting CR after CRT, but none included lymph nodes in the analysis (ypT0N0). The aim of the present study was to retrospectively determine the additional value of DWI-MRI to conventional (T2-weighted) MRI for predicting CR after CRT.
Methods and Materials: Eighty locally advanced rectal cancer patients underwent CRT followed by restaging MRI and operation. MRI consisted of conventional sequences and DWI. Two readers with different levels of experience independently scored conventional images for CR and, in a second reading, combined conventional and DWI-MRI images. A 5-point confidence level score was used to generate ROC curves. Differences in performance were calculated by comparing areas under the ROC curves (AUC). Interobserver agreement, sensitivity, specificity and positive predictive values (PPV) were calculated. Histology served as reference standard.
Results: Ten of 80 patients (13%) had a pathologic complete response (ypT0N0). Comparison of the ROC curves showed significant improvement of the AUC only for the experienced reader 1 from 0,77 to 0,88 (p=0,009). Sensitivity improved from 20-30% to 40-70%. Specificity and PPV improved only for reader 1 from 87 to 93 %, resp., 25 to 58 %. Interobserver agreement improved from 0,14 to 0,27.
Conclusion: Adding DWI to conventional MRI improves diagnostic performance of experienced readers and increases interobserver agreement for identification of CR. Sensitivity and PPV remain low, with a considerable risk of over- and undertreatment.

A-236 Role of tomosynthesis in lung imaging
M. Båth | Saturday, March 9, 08:30 – 10:00 / Room G/H
Tomosynthesis is an imaging technique that in recent years has become available for lung imaging. Using low-dose projections of the chest, acquired over a limited angular range, an arbitrary number of section images can be reconstructed, enabling the chest to be visualised in millimetre-thick slices at a very low effective dose. Compared to conventional chest radiography, the disturbance of overlapping anatomy (the main limiting factor for detection of pathology, e.g. pulmonary nodules in chest radiography) is considerably reduced in chest tomosynthesis. Early evaluations have also shown that the detectability of pulmonary nodules is significantly higher in chest tomosynthesis than in conventional radiography. However, compared to computed tomography (CT) the limited angular range used in tomosynthesis results in a reduction in depth resolution, not allowing tomosynthesis to reach the same detection rate as can be obtained with CT. Especially, pathology in the subpleural region may be more difficult to interpret. Nevertheless, most lesions are visible in retrospect on chest tomosynthesis, suggesting that the technique may be suitable for follow-up. This presentation will summarise early evaluations and reported clinical experiences of the technique, as well as describe some of its strengths and limitations.