Since some of you misdiagnosed the right aortic arch in case 9, I will give you another chance with another mediastinal case in a 45-year-old man, who is asymptomatic.
1. Pericardial cyst
2. Pericardial fat pad
3. Thymic tumour
4. All of the above
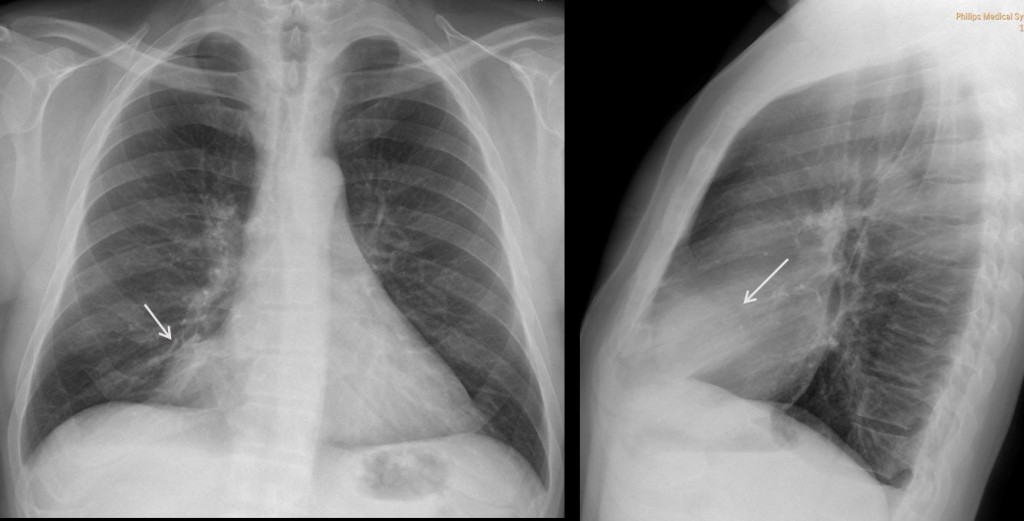
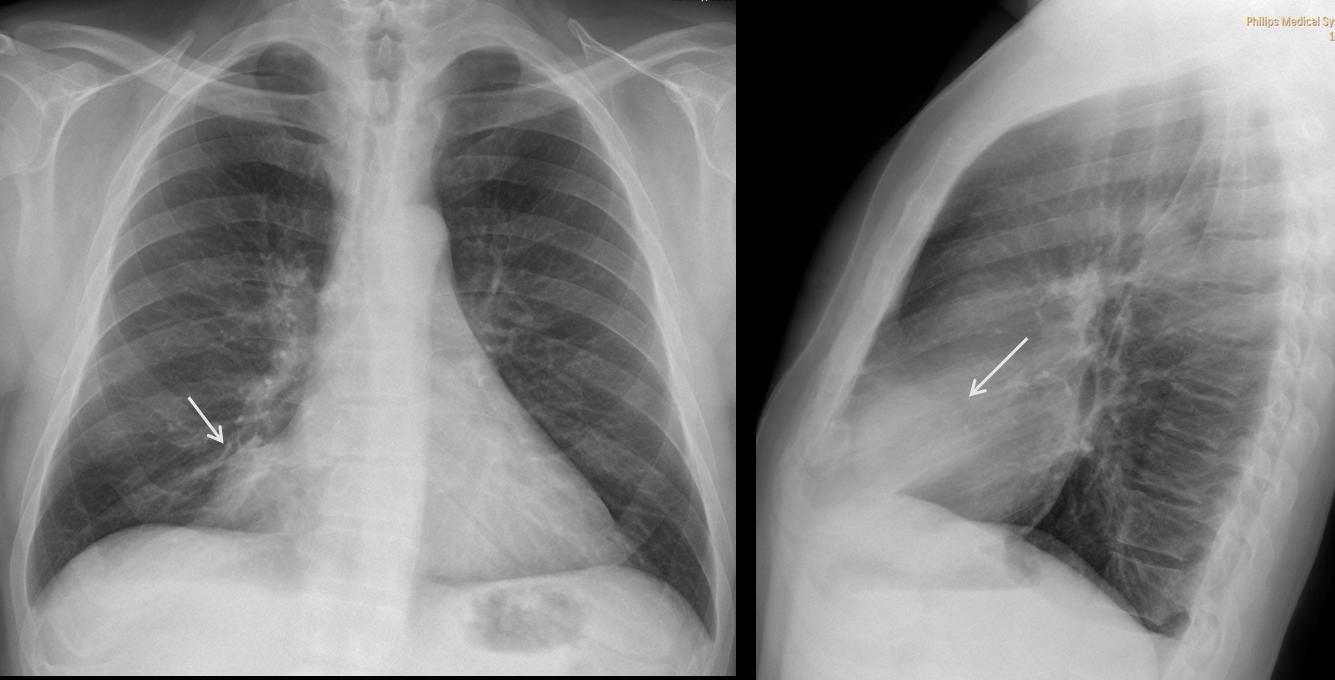
Fig. 2
Findings: PA and lateral chest radiographs show an extrapulmonary mediastinal mass (arrows) occupying what is called the cardiophrenic space.
Masses in the cardiophrenic space (CS) are not uncommon and are easily recognized in the PA and lateral chest radiographs.
From the diagnostic viewpoint, all lesions in the CS have the same appearance on chest radiography and therefore, cannot be differentiated. The correct answer is: 4. All of the above.
On CT, these lesions can be of soft tissue density (mediastinal tumour), water density (pericardial cyst) or fat density (pericardial fat pad).
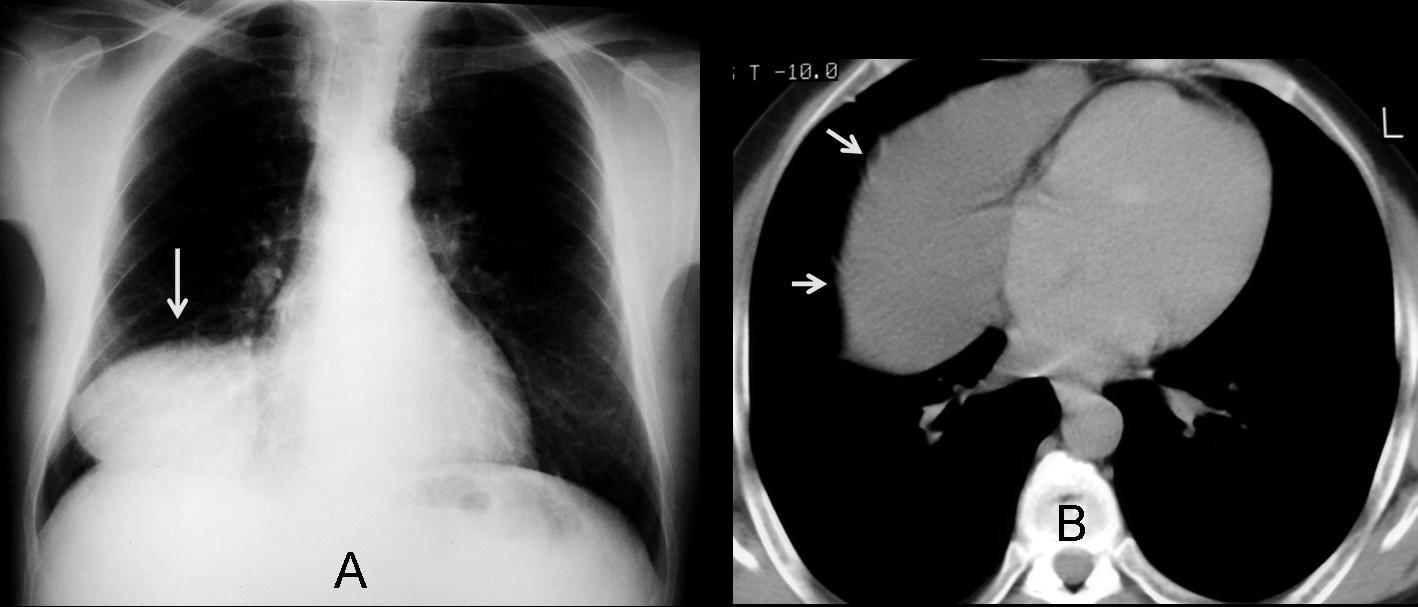
In the case shown, CT depicts a non-enhancing, rounded fluid-filled mass in the CS (arrow), measuring 7 H.U.
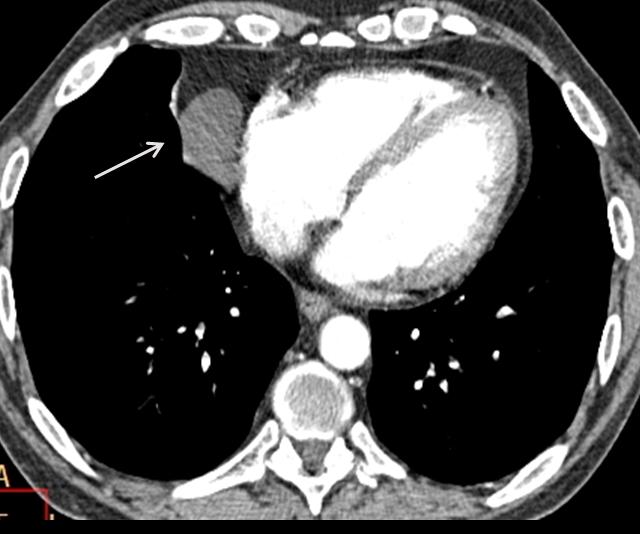
Fig. 3
Final diagnosis: pericardial cyst
Pericardial cyst (Fig. 4, arrows) is the most common fluid-filled mass in the CS. It is located more commonly on the right than on the left and appears as a CS mass in the chest radiograph (Fig. 4a, arrow). CT shows a cystic lesion with well-defined borders and smooth walls (Fig. 4b, arrows). Note the change of shape in the upright and recumbent position, indicating a partially filled cyst.
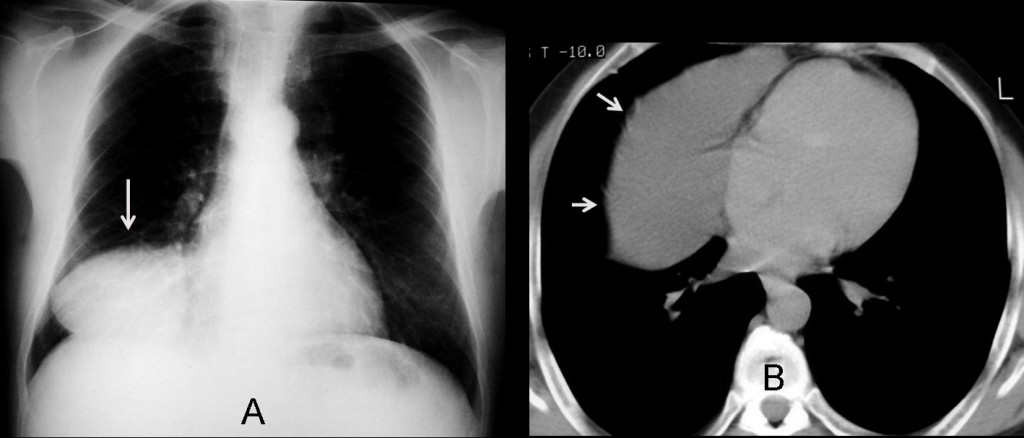
Fig. 4
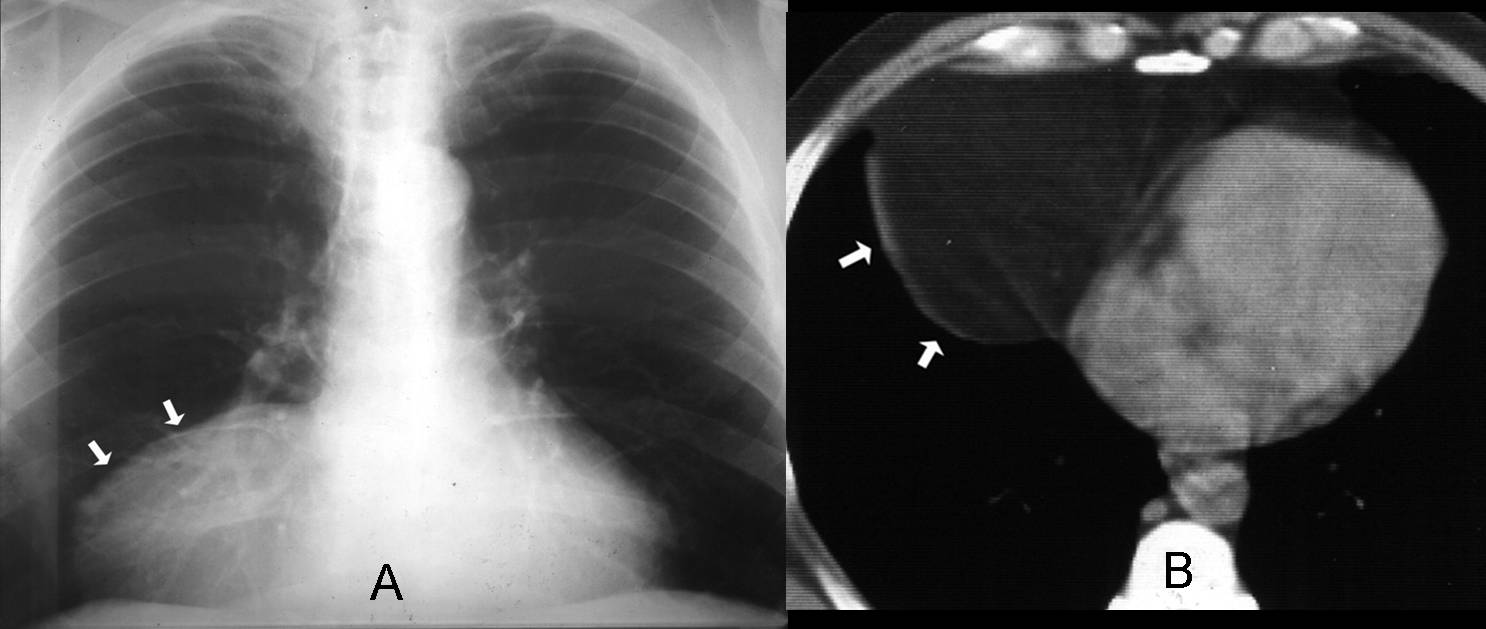
Fatty lesions
The most common fatty lesion in the CS is the pericardial fat pad. An enlarged fat pad can simulate a mass in the chest radiograph (Fig 5a, arrows). The diagnosis is easily made with CT, which confirms the large fat pad (Fig. 5b, arrows). The absence of encapsulation and lack of a soft-tissue component differentiate normal fat from the rare fat-containing tumour.
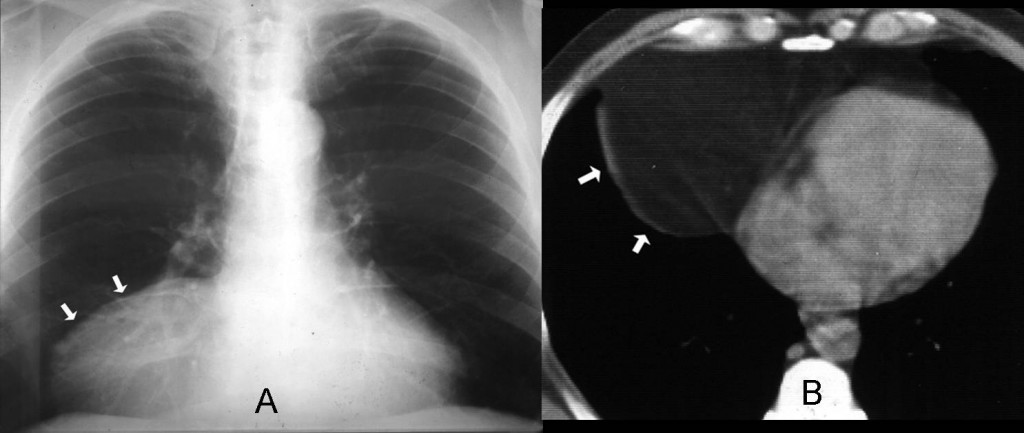
Fig. 5
Soft tissue density
The most common solid lesion in the CS is lymphadenopathy; they are usually multiple and not very large (Fig. 6, arrows). Lymphoma is the most frequent cause. They may also originate from tumors above or below the diaphragm.
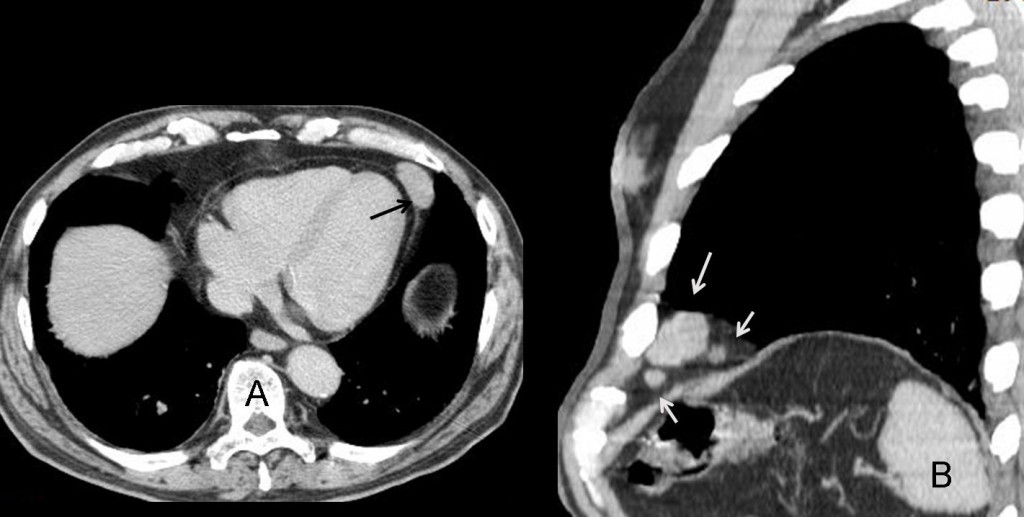
Fig. 6
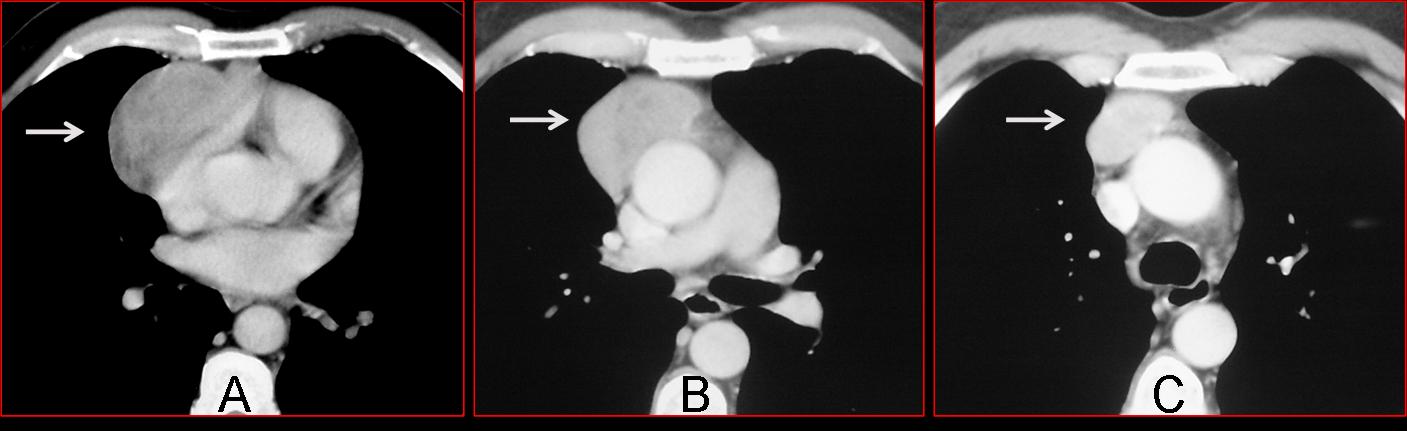
In large soft-tissue tumours of the CS, a thymic origin should be suspected. Although thymic tumours originate in the anterior superior mediastinum, they may slide down along the mediastinal planes and appear in the CS (Fig 7a+b, arrows). A useful diagnostic feature is that they always maintain a connection with the superior mediastinum, visible on CT (Fig 7c, arrow).
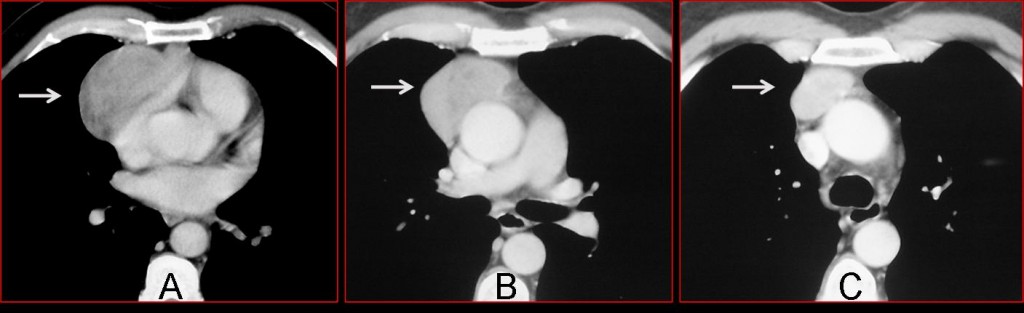
Fig. 7
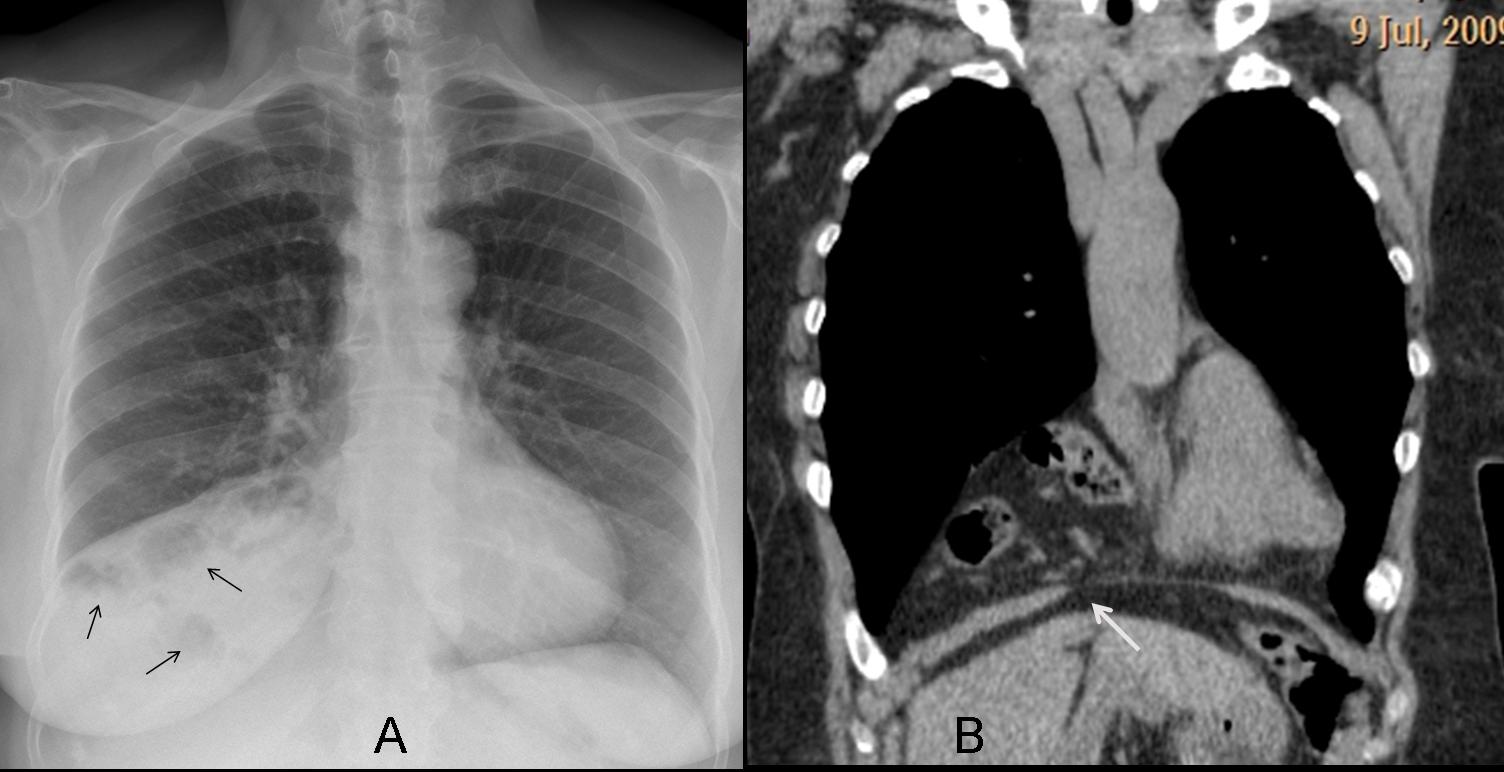
Morgagni hernia
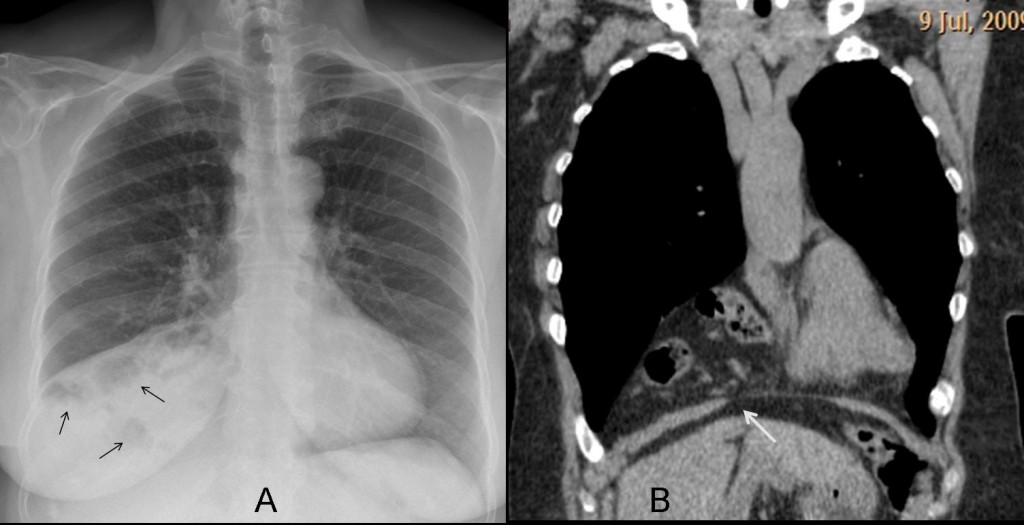
Fig. 8
A hernia through the foramen of Morgagni may simulate a mass in the CS. The diagnosis can be suggested in the chest radiograph if aerated bowel loops are seen (Fig. 8a, arrows). If not, the diagnosis rests on CT, which shows the herniated fat and bowel and the diaphragmatic defect (Fig. 8b, arrow).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
Masses in the CS are not uncommon, and their etiology cannot be determined in the chest radiograph.
CT is diagnostic by showing the radiographic density: fat (pericardial fat pad, Morgagni’s hernia); water (pericardial cyst) and soft-tissue ( lymphadenopathy and the occasional thymic tumour).
Suggested reading: Lesions at the cardiophrenic space: findings at cross-sectional imaging. RadioGraphics 27:19-32. 2007
Case prepared by Dr. Pepe





Thanks for the great case.I hope that this cases Will survive till ECR.
There is a round nodular, central radiolucency and rim capsular like lesion at the apex öd the heArt. This lesion is over the diapragm and inlerior the manibrium.. This can be a pericardial cyst.
The Pepe’nin hat is so Cool
Got it in Chicago, during RSNA
Pericardial Cyst.
1. Pericardial cyst
Pericardial Cyst
Is this an Aunt Minnie’s reply?
pericardial cyst
The answer correct Is number 4
Excellent. You gave the right answer
Pericardial cyst…typical location (right cardio-phrenic angle), not of fat density (ie does not look like a pericardial fat pad).
What does pericardial fat pad look like?
Hmmm…I am changing position here. Pericardial cysts are more homogenous and more discrete…and most of all more cyst like (round/oval).
On second thoughts, this looks more like a pericardial fat pad…triangular, does not produce a silhouette with the heart.
Which are your arguments against thymic tumor?
The site (thymic tumours are often in the anterior/superior mediastinum…although like anything thymic tumours can be ectopic).
Pericardial cyst??
1)Pericardial cyst.
2)Pericardial fat pad high density
Premesso che non si può differenziare sulle radiografie standard una cisti pericardica da un cuscinetto adiposo dell’angolo cardio-frenico, in quanto entrambe rx-opache, a me sembra invece che si tratti di una ernia di Morgagni a contenuto adiposo peritoneale: il profilo diaframmatico dx , anteriormente non è bel visibile ed invece si intuisce una opacità che sale dalla cavità addominale (vedi radiogramma LL).
pericardial fat pad
Classic differential of cardiophrenic angle opacity includes pericardial cyst, pericardial fat pad and Morgagni hernia.
It’s round shape and homogeneity (vs Morgagni) as well as the assimetry in the contralateral side (vs fat pad) makes me choose pericardial cyst as my first option.
You have to choose wisely.
Pericardial cyst
There is a rounded lesion which obscures the right heart border indicating that this is located in or is in contact with the middle mediastinum. The well defined lateral margin indicates contact with adjacent middle lobe lung parenchyma. The high density of the lesion and rounded shape does not fit with an epicardial fat pad. The low location of the mass and the normal retrosternal clear space goes against a thymic tumour. A pericardial cyst is therefore the most likely diagnosis.
Thymic tumor due to its location in the anterior mediastinum
Itis a good possibility; but not the correct answer
So we rule out the worst case scenario?
Looking forward to reading the correct answer
Thank you for answering
I must offer my gratitude and a lots of thanks for uploading such awesome educational material for us residents. Thanks a lot Dr Caceres. I hope you continue this process. You are a source of inspitaion for us.
Regards.