Today’s images belong to a 57-year-old male who is going to undergo a lung transplant for chronic lung disease.
What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
Findings: chest radiographs show emphysematous lungs with calcified granulomas and signs of pulmonary hypertension. The PA film shows an apparent mass with circular calcification (A, arrows) above the aortic knob. It is visible behind the trachea in the lateral view (B, arrow).
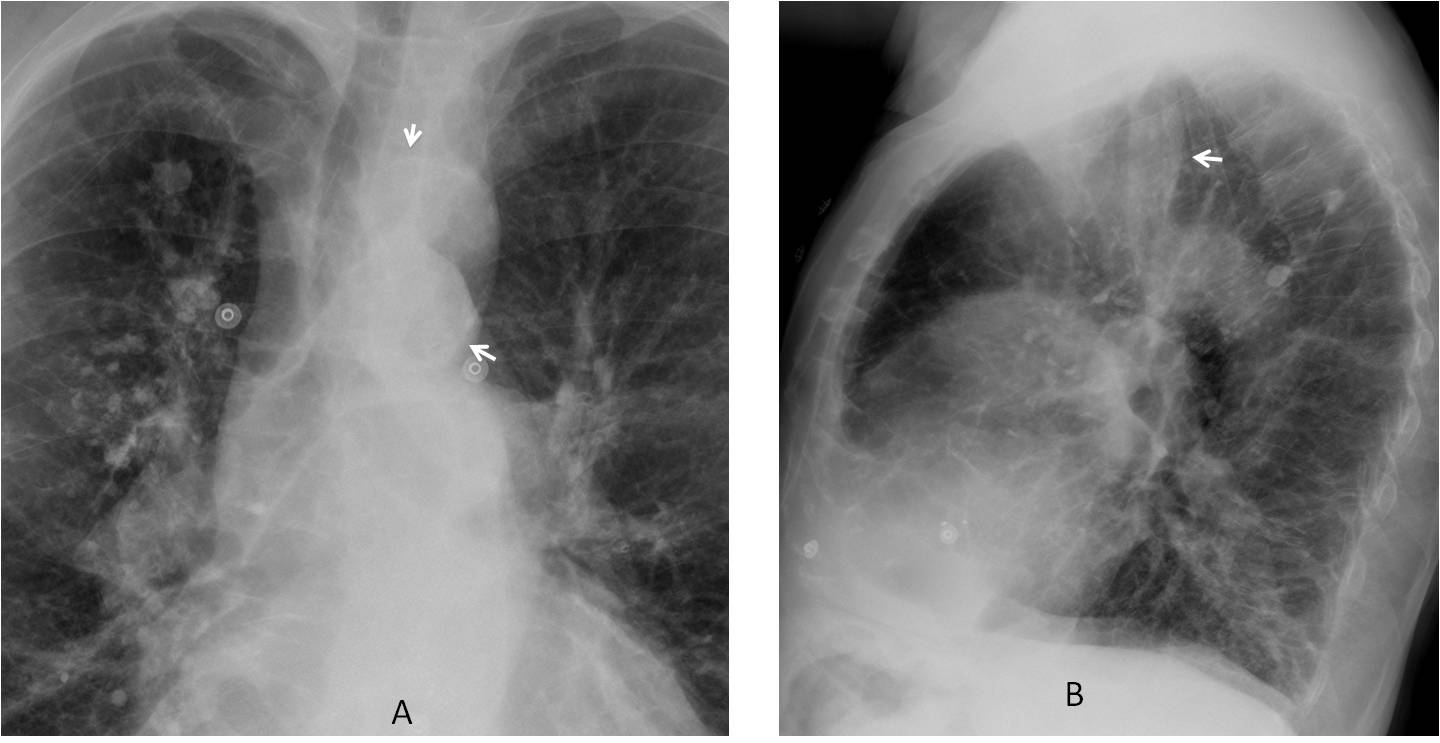
Unenhanced sagittal CT shows that the apparent mass represents a high aortic arch (C, red arrow), which angles when joining the descending aorta (C-D, red arrows).

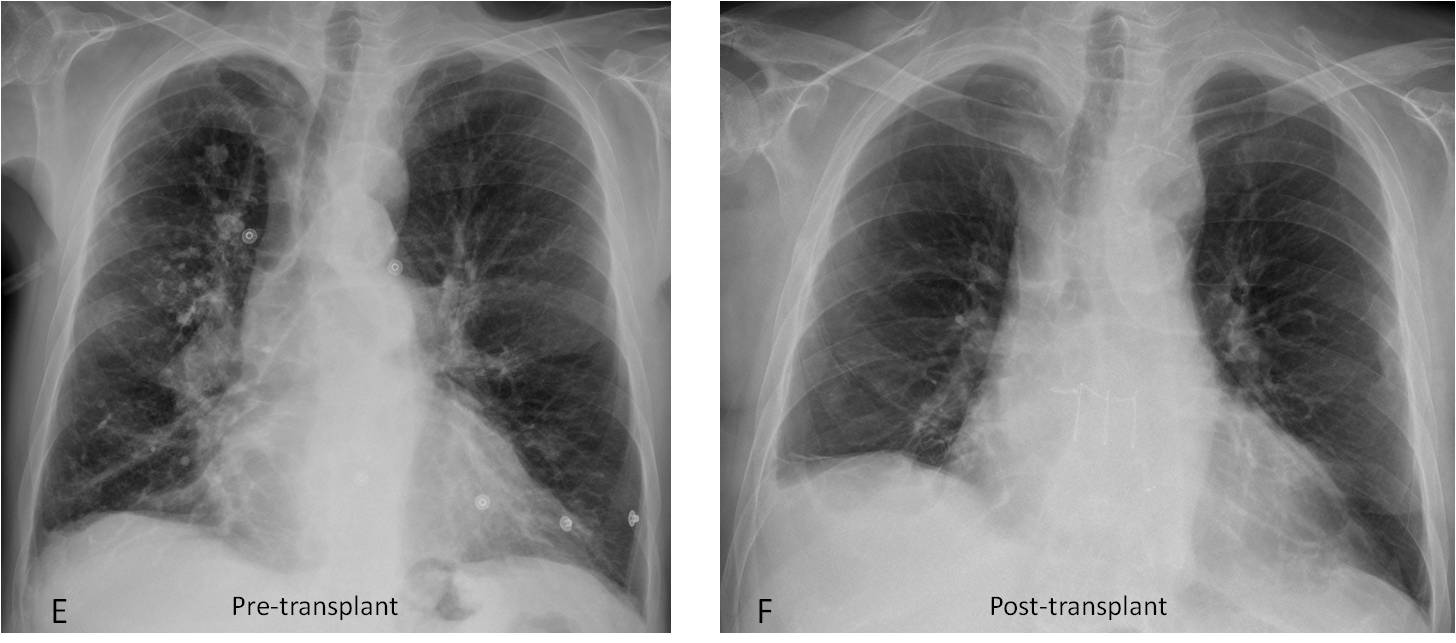
This appearance is typical of aortic pseudocoartation, which should be suspected in the plain film (I have seen several with similar appearance. See Cáceres’ Corner Case 42). The patient had normal blood pressure and underwent a bilateral lung transplant without complications (E-F).
Final diagnosis: unexpected aortic pseudocoarctation in a patient with severe emphysema pending lung transplant.
Congratulations to Pasquale and sht, who were the first to suggest a vascular anomaly of the mediastinum.
Teaching points:
1. When seeing circular calcification in the mediastinum always think of a cyst or a vascular structure.
2. Avoid satisfaction of search. Do not focus on the obvious.




i think their is anodule in the upper right lobe
The nodule is calcified and it is part of the process that indicated the trasplant
Aortic aneurysm
Hello,
there are different size calcified nodules mainly in right lung. Some are laying on major fissure. Both hilas are enlarged with some calcification. Heart is enlarged and there is prominent interstitium.
I suspect granulomas or some kind of occupational disease.
I agree with this findings, Thanks.
hey,
there are multiple calcified pleural plaques and irregular opacities predominant in the right lobe. Has there been any asbestos exposure 10-15 years in the past? if yes, asbestosis.
I think amyloidosis would be in the differential.
Another possibility would be mitral valve disease, mainly stenosis, with subsequent pulmonary hemosiderosis. That would explain the heart enlargement and the signs of pulmonary hypertension.
lucent oval lesion projecting in mediastinum. Is the patient complaining for anything?
Other dyspnea, the patient has no complaints
heart enlarged.
reticulonodular markings both lungs, more extensive on the right.
calcifications are noted in some of the nodules.
wedge shadow right hilum – ?atelectasis.
an oval soft tissue shadow is seen (overlying aorta in frontal projection and anterior in lateral xr)
trachea shifted to right.
?vascular anomaly
There are calcifications and masses that could be related for example with silicosis although the appearance is not typical. There is loss of volume of the left lower lobe with narrowing od its bronchus and donut sign in the lateral view which suggests hilar lymph nodes. I would do a CT under the suspicion of a lung cancer underlying the chronic disease that could be silicosis or not.
there are multiple Rt. sided pulmonary nodules associated with fibrotic bands and decrease Rt lung volume resulting in shift of mediastinum to the Rt side , so we have to think about causes of unilateral pulmonary fibrosis like post primary TB,chronic pulmonary infection, systemic sclerosis, circulatory disorders, radiation induced, and ventilator induced lung injury .
Sarcoidosis
There are some probably pleural calcifications predominant in the right lobe, as well as a reticular pattern of the interstitial structures. Has there been any asbestos exposure years ago? If yes, I’d say probably asbestosis, even though basal plaques would be more typical.
No asbestos exposure.
Chest X-ray frontal projection showing coarse interstitial shadowing distributed in all lung zones bilaterally but with predominance over mid lung zones. Associated multiple nodules are also seen which are of variable sizes ans sims of them are showing calcification. These nodules are predominantly on right sided lung and mainly distributed along bronchvascular shadows and two of them seem to b along major fissure as evident in lateral view. Bilateral Hilas are asymmetrically enlarged pointing towards lymphadenopathy. I could not see any lung volume loss, consolidation or bronchiectasis —- all the above mentioned findings are favouring the diagnosis of sarcoidosis. With differential of other ILDs
Additional to it I can see a catheter over the right upper hemithorax. Can’t really decide for what purpose.
There is central mediastinal opacity overlying the heart and exiting anteriorly not displacing the mediastinal structures. I can’t c the calcification in it. I will give the differentials here as of bronchigenic cyst. Lymphadenopathy. Thymus mass. Less likely vascular as it is not in continuation with aorta. Very less likely teratoma at this age.
I would like to have the hrct of the patient and if required will go for CE CT.
Will show you the CT on Friday 😉
…quello che mi ha colpito di più è una opacità , rotondeggiante in AP ed ovaliforme in LL, a livello di origine dell’arco aortico…potrebbe trattarsi di un aneurisma (coronarico?)….il quadro polmonare è compatibile con i segni dell’ipertensione polmonare da trombo-embolismo cronico….MESSI SUPER OMNES !!!!
Occupation / history of exposure, please?
No history of exposure.
Creo que es un paciente con epoc porque tiene un aumento e hiperclaridad del espacio retroesternal y un aplanamiento de los diafragmas, y el tubo que se ve en el hemitorax derecho podrían ser gafas nasales para oxígeno.
Además veo un patrón intersticial reticular y nódulos calcificados que se pueden ver en una fibrosis que también puede tener un paciente con epoc.
Y por ultimo los hilios creo que están aumentados como consecuencia de hipertensión pulmonar mantenida.
You are correct. Severe emphysema was the reason to indicate the trasplant. But there are additional findings in the chest radiograph.
Right ventricle aneurysm maybe or massive right heart dilation…
pulmonary arterial hypertension plus some mass in the middle mediastinum – vascular etiology?