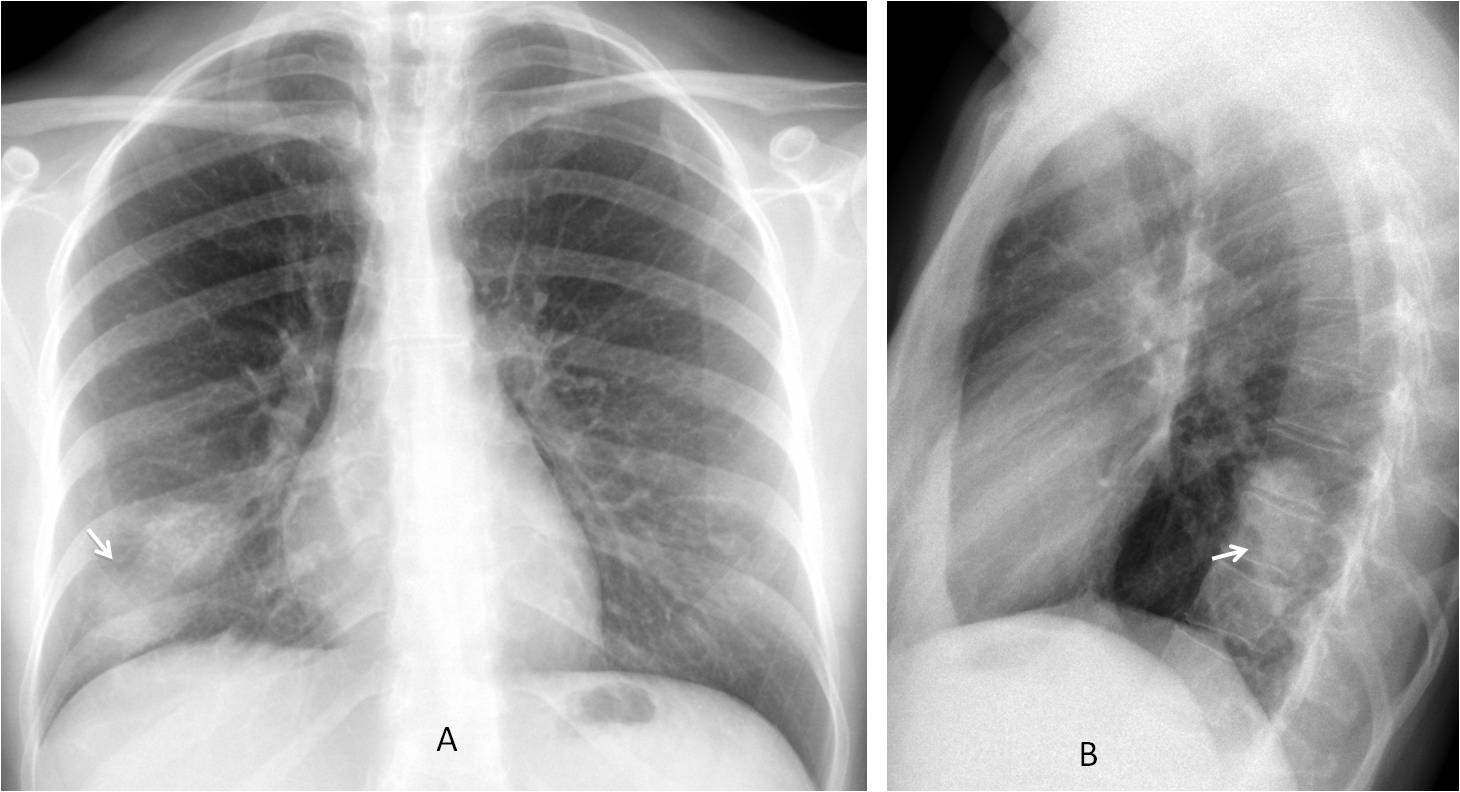
Dr. Pepe is back and he refuses to show easy cases. He has forced me to present the following images which belong to a 38-year-old woman with right chest pain. Check the three images below, leave us your thoughts in the comments section and come back on Friday for the answer.
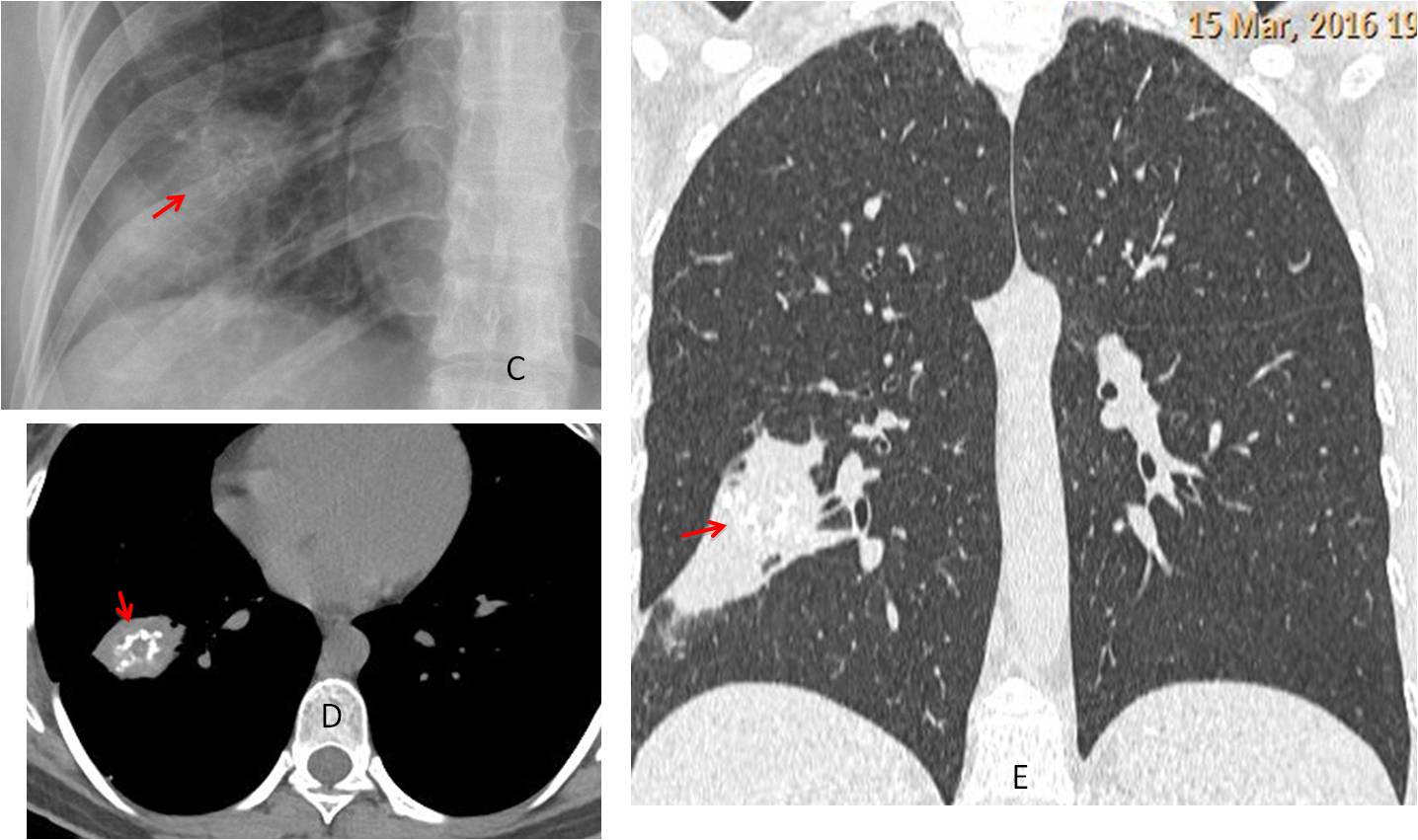
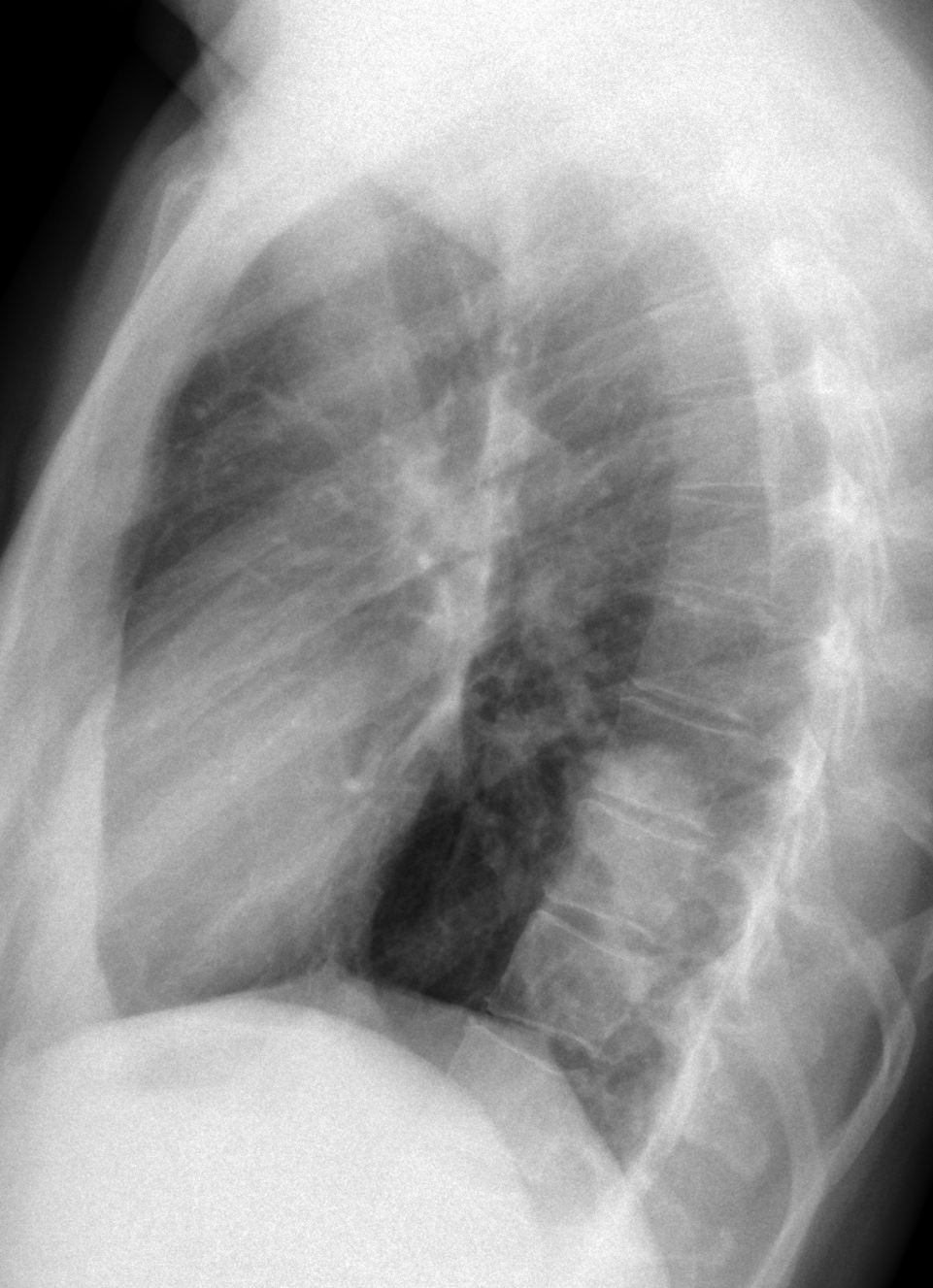
Findings: chest radiographs show an ovoid ill-defined opacity in the RLL (A-B, arrows). There are calcifications within it, better seen in the view of the ribs (C, red arrow).
The presence of visible calcifications excludes the diagnosis of carcinoma. The ill-defined contour and the oblong shape go against hamartoma. Chronic TB cannot be excluded, but I don’t like it.
Axial and coronal unenhanced CT confirms the pulmonary lesion adjacent to the major fissure. Calcifications are clearly visible (D-E, red arrows).
With the information provided by the chest radiograph we can assume that the lesion is chronic (calcium present), affects the parenchyma and does not give significant symptoms. A lesion that fits this description is an inflammatory pseudotumour, which was confirmed by lung biopsy.
An interest fact is that yesterday I searched in Google: “localized calcified chronic pulmonary infiltrate in right lower lobe” and got an article about unusual lung tumors in which the pseudotumor was mentioned (RadioGraphics 2002; 22:601-619).
Final diagnosis: inflammatory myofibroblastic tumour a.k.a. inflammatory pseudotumour.
Congratulations to all of you who fought bravely against insurmountable odds. I saw this case two months ago (see the date in the CT) and thought that you might appreciate it.
Teaching point: although this case is tough, an accurate interpretation of the findings leads to a short differential diagnosis that includes the final answer.




Hamartoma
rather well defined opacity involving the posterior aspect of the right lower lung lobe and shows multiple calcifications at its upper portion, mostly hamartoma
Hello,
lesion in right lower lobe connected by broad base to posterior pleura. If is it hard case I suppose round atelectasis – CT confirmation needed.
I hope you do not consider rounded atelectasis a hard case! And there is an element missing: pleural thickening.
Take a second shot 😉
I may be over the line here…
It seems like two lesions overlapping:
1. Background smaller hamartoma
2. More apparent nodular opacity with peripheral atelectasis which could indicate lung cancer
Ingenious!
I really hope that’s a compliment and you’re not just being sarcastic with me Professor..
😉
It is acompliment! It would explain the calcium (hamartoma) and the poor definition of the lower part.
A sarcastic teacher is a poor teacher
Thank you,
i am releaved…
Hamartoma
Two opacities in the right lower lobes draining together not homogeneous with slightly ill-defined contours
There is pleural thickening well seen on PA view on the level of middle clavicula line. And on lateral view there is pleural thickening in great fissure.
On PA view there multiple small nodules on the level of the III rib, III intercostal space, IV rib and IV intercostal space, small nodules are also seen on the upper part of opacity more laterally. Some of that nodules looks “old” – they have slight increased attenuation.
The differential diagnosis should be done between relapse of tuberculosis and neoplasm with MTS dissemination in the right lung
But mostly suggesting tuberculosis
He didn’t lost weight?
No, she didn’t
Tubercolusis Granuloma
sequestration of the lung
Very unusual with visible calcium in the radiograph
hamartoma
oval shaped opacity is seen at the apical segment of the right lower lobe.
There is linear vascular structure extending from the hilum to the lesion.
There is no evidence of bone erosion.
There is serpiginous density seen within the lesion.
Hamartoma is highly suspicious, CT is needed to look for any fat component.
In my experience, hamartomas have sharper borders
So I think one of the possibilities could be arterio venous malformation
With calcium?
There are two lung dnodules that coalesce in the RLL one of them with a serpiginous calcification. The key point for me is the calcification.
Serpiginous calcifications like this can be seen in some parasit disease such as filariasis in the breast. I was wondering if this could be a possibility in this case. Lung filariasis.
A gossibipoma can also show serpiginous calcifications but there are no features suggesting previous thoracic surgery. If this had been the case a foreign body would be a possibility
Lung cancer is infrequent ammong young adults and does not show this calcifications.
Hammartoma and tuberculous granuloma calcify but not this way
So I would go for none of the above
Intelligent discussion. Patient was a Spaniard, no foreign travel. I agree with your opinion (none of the above). So what is it?
Soft opacity right lower lobe with serpiginous calfifications and a small round lucent area inside.
Hamartoma.
Ddx – vascular malformation
– TB
See answer to M A Fahmy, above.
“None of the above”
The only differentials for that calcification I can think of:
– parasite (but that’s usually in the skin)
– vascular malformation
– occupational lung disease (but she is only 38y)
…magico Professore…..Bari risponde: probabile cisti idatidea con calcificazione degli scolici e/o della membrana, rotta ed accartocciata….minute altre piccoli esiti calcifici nodulari omolaterali…..
Dear friend, in my opinion, calcification goes against hydatid cyst. Analysis of the abnormality:
1. Calcification goes against malignancy and suggests a chonic process
2. Minimal symptoms. Non-specific pain
3. Definitely an ill-defined pulmonary process This information narrows down the differential diagnosis before biopsy
…sempre grazie magico Prof., perchè ci aiuti a riflettere con i bei casi che ci proponi….
Granulomatous disease secondary to inflammatory process or infectious disease, maybe vasculitides? Tuberculosis or fungal disease?
I believe those are sensible diagnosis. Wait for the answer tomorrow
Calcified hydatid cyst in a lung?
“None of the above”
The only differentials for that calcification I can think of:
– parasite (but that’s usually in the skin)
– vascular malformation
– occupational lung disease (but she is only 38y)