Spring is here and it makes us want to present easy cases. Today we are showing preoperative radiographs for ankle trauma in a 47-year-old woman.
What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
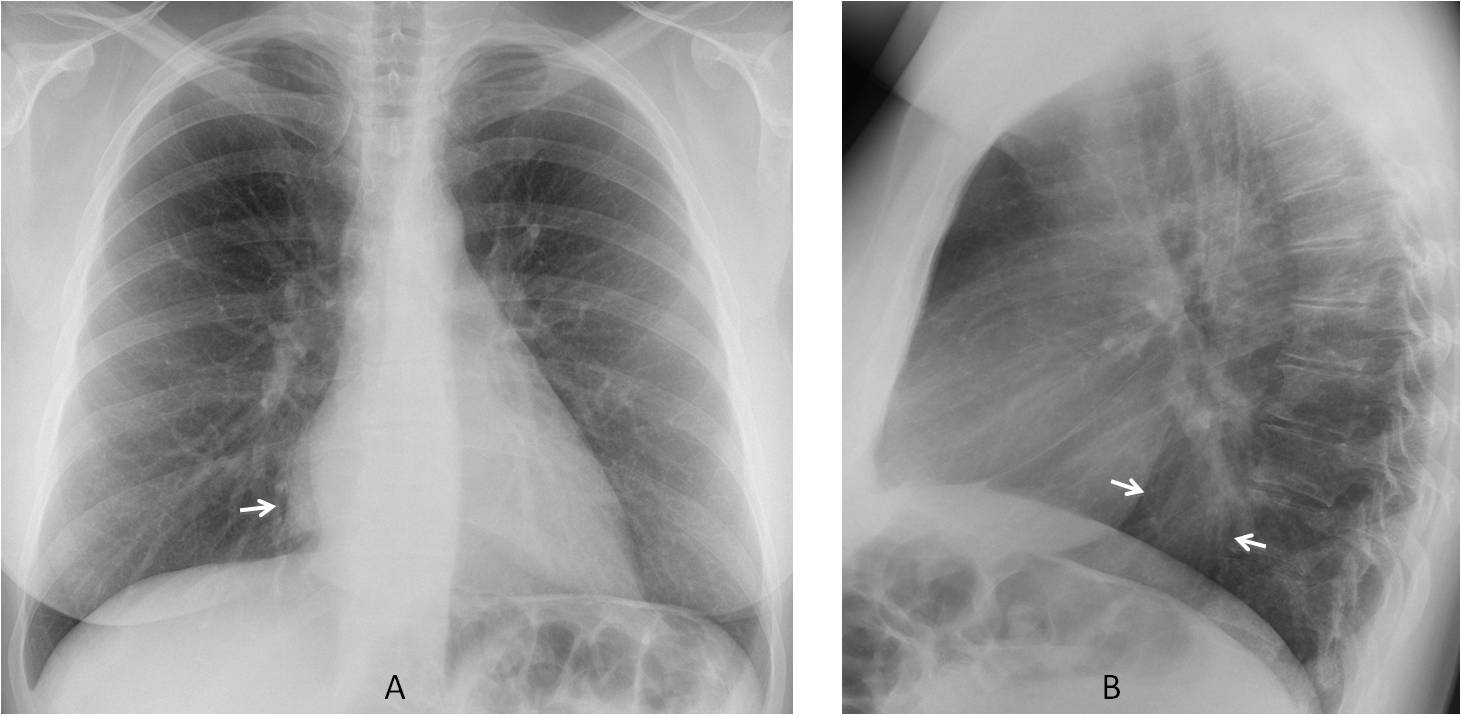
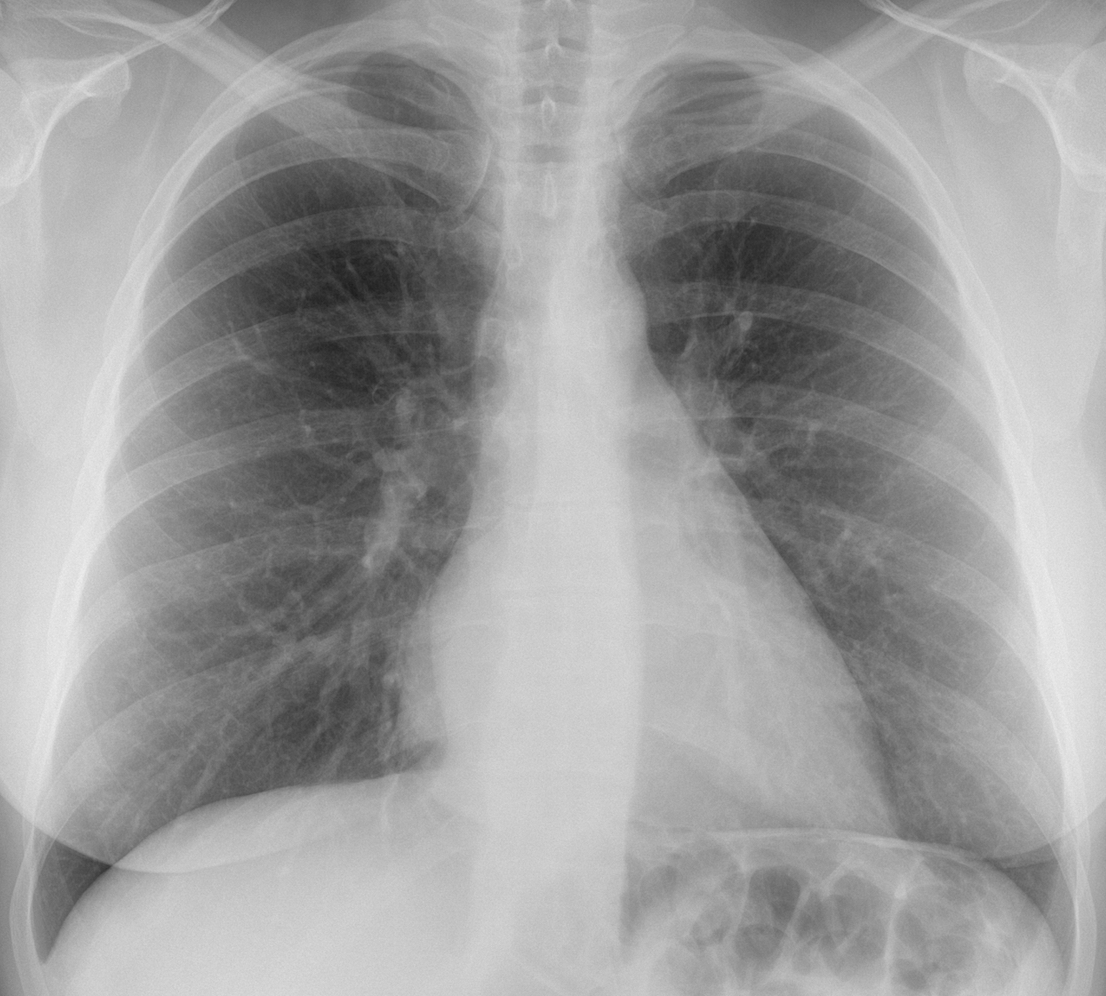
Findings: the PA radiograph shows a well-defined line (A, arrow) paralleling the right heart border, suggesting a mediastinal mass. The lateral view shows occupation of the retrocardiac space (B, arrows), locating the mass in the lower middle mediastinum.
The first diagnostic option should be an airless hiatus hernia, followed by oesophageal lesions such as duplication cyst, wall tumour or varices.
Coronal and axial enhanced CT shows a solid mass adherent to the oesophageal wall (C-D, arrows). Endoscopy confirmed an oesophageal parietal tumour with mild ulceration.
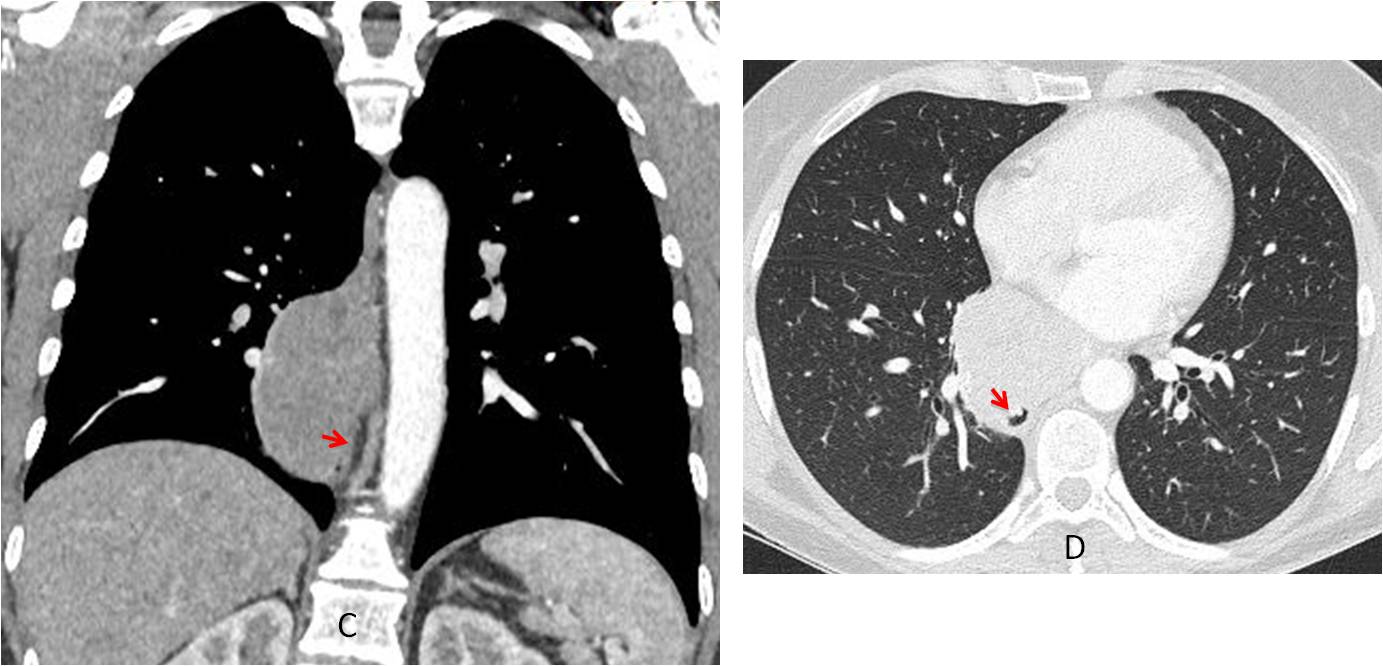
Final diagnosis: oesophageal parietal tumour (GIST)
Congratulations to all of you who placed the mass in the lower middle mediastinum, led by maurizio franz, who was the first.
Teaching point: remember that any abnormality should be properly evaluated and placed. Once this is done, the differential diagnosis is easy. This is a simple case and some of you made it complicated. Don’t forget the KISS method!



Good morning,
There is an increased density next to the right cardiac border that doesn´t blured it. There is not sillhoutte sign, (different density or no medial lobe location). The retrocardiac space is occupied (pathology on the inferior lobe).
Right paravertebral line is ok.
Any clinical symptoms?
Patient is asymptomatic. It is a preop film.
Duplication or pericardial cyst?
Which one blurs the cardiac border?
Perdicardial cyst doesn’t blurred
Sorry, I think it depends on the density and the exactly location of the lesion, so I can´t give you an exactly answer.
Hi
There is an opacity in the right paracardiac location not silhouetting the cardiac border and localized to the retrocardiac location in the lateral chest X-ray. The vessels are not obscured and the lesion has a relatively well defined contour suggesting it not of lung origin. Differential in this case would be hiatal hernia ,aortic aneurysm and sequestration
If you believe the lung is not affected, the sequestration has to be extrapulmonary
….piccola ernia di Bohckdalek….
There seems to be no gastric bubble besides the meteoristic distended colon and a discrete opacification in the inferior middle mediastinum. There is also an opacity medial-basal on the right side without obscuring the right heart border and of sharp demarcation.
DD: Hiatal Hernia without air-bubble?
Hiatus hernia should be the first diagnosis in this type of lesion. It was not in this case.
.. ec Morgagni
Hi,
there is a density adjacent to the right atrial border not obscuring it. on the lateral view i can see splaying of the most anterior inferior part of the major fissure merging with the diaphragm, and possibly a small density over the anterior costophrenic recess, the density possibly represents a small major fissure effusion or a small consolidation in the anterior costophrenic recess.
another confusing finding is the triangular shape of the lower right atrial border/IVC?, I cannot explain it! (variant, artifact?.).
thanks
There ıs density in right paracardiac location and it ıs not silhouette sign. Pathology might be at azygoesophageal racers. Probably Bochdalek hernia
Sorry. Recess
Bochladek hernias are posterior and in this case the abnormality is located in the middle mediastinum
Chilaiditi syndrom may be.
Chilaiditi syndrome is anterior transposition of a loop of colon between the diaphragm and the liver. No such thing here.
LAtrium and LVentricular enlargement signs, mild RV dilated suggests heart problem.
Dorsal primary arthrosis if age related.
Trauma history and surgery indication thorax x-ray
don’t exclude pulmonary thromboembolism.
chilaiditi’s syndrome
It can’t be Chilaiditi; for explanation see my reply to Dimitrova.
I agree with you
Cardiophrenic fat or pericardial cyst
Both of them occur in the cardiophrenic angle. Are you sure o your diagnosis?
Lt upper lobe loss of volume
Right paracardiac radiopacity of defined borders, with signs of the negative silhouette, which corresponds to a middle mediastinal lesion, later discarded in lateral incidence. Would I play for a lipoma? Or an adenopathy ?.
You reading is correct. You cannot go any further without CT. Airless hiatus hernia should be the first diagnosis, but it isn’t.
Hi,
the lesion is located either anterior or posterior to the heart, and since it cannot be seen on the lateral view anywhere in the lungs or mediastinum, i suppose it should be a chest wall lesion.
thanks.