Today I am showing chest radiographs of a 47-year-old man with fever and moderate dyspnoea. What do you see?
Check the images below, leave your thoughts in the comments section and come back on Friday for the answer.
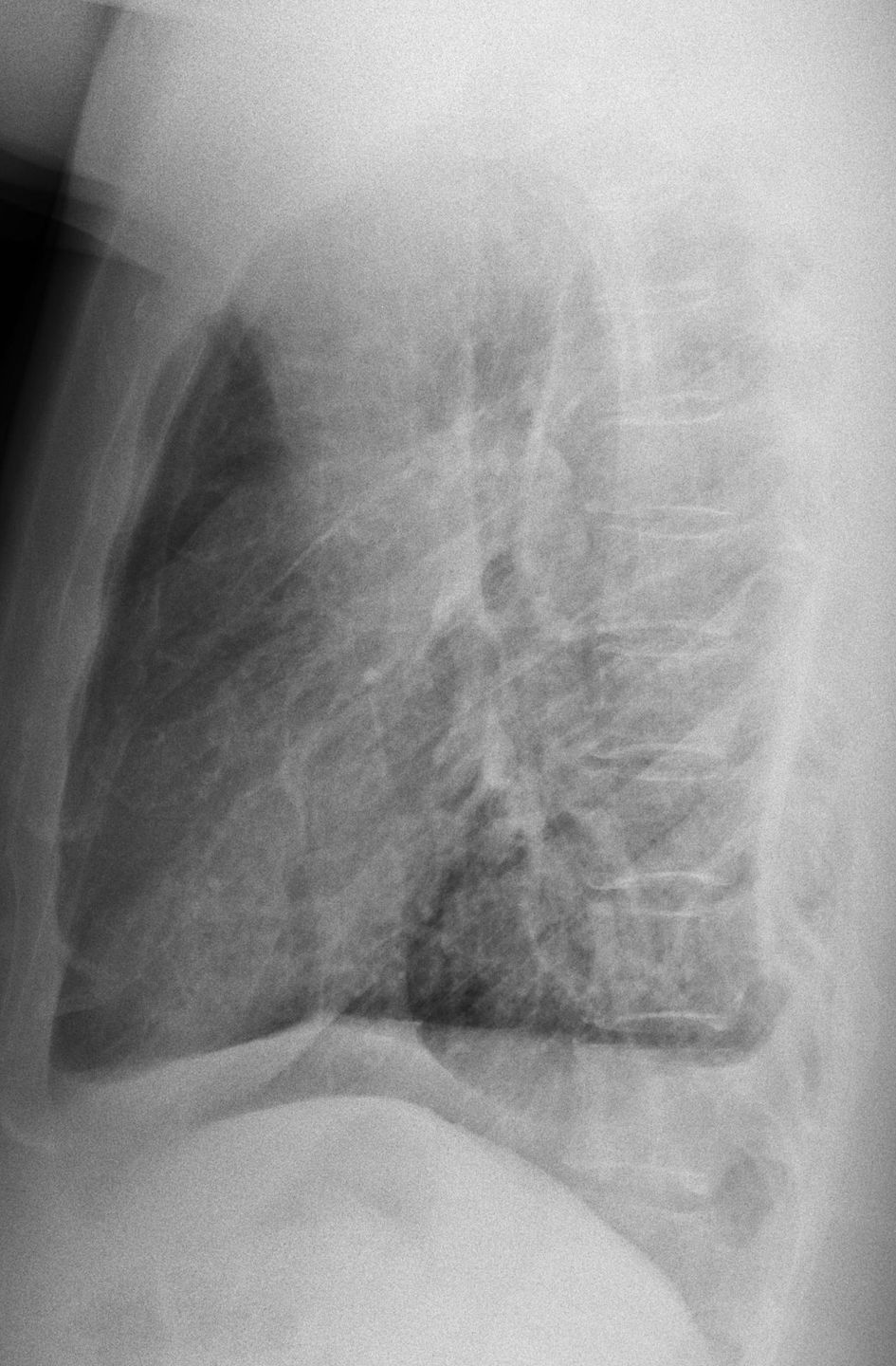
Findings: Chest radiographs show a small right hemithorax secondary to chronic calcified pleural thickening (A-B, arrows). The lower aspect of the pleura is split (A, red arrows), with air between both pleural layers. The appearance is pathognomonic of a bronchopleural fistula. There are pulmonary infiltrates in the left lung (A, circle).
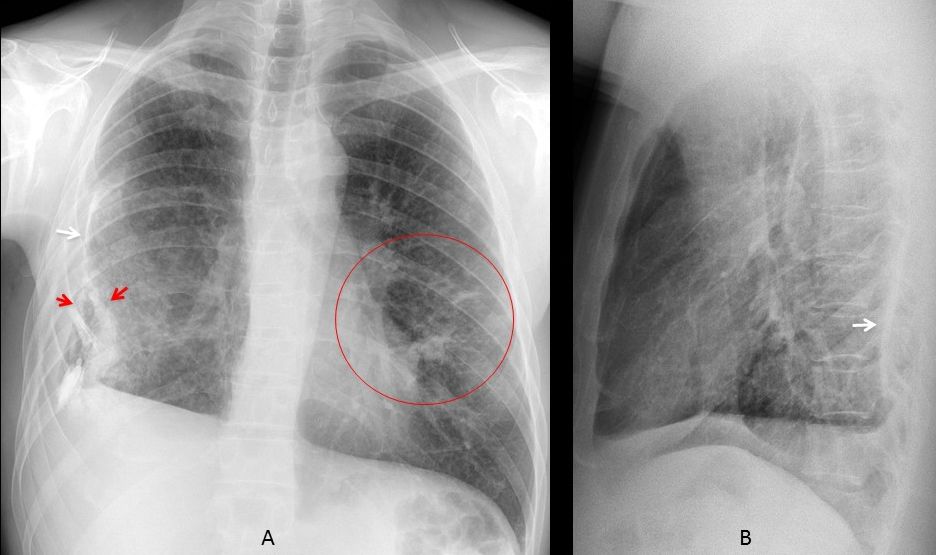
Cone down PA view taken six years earlier shows only calcified pleural thickening (D, arrow). Compare with the present radiograph (E) and the coronal CT (F).
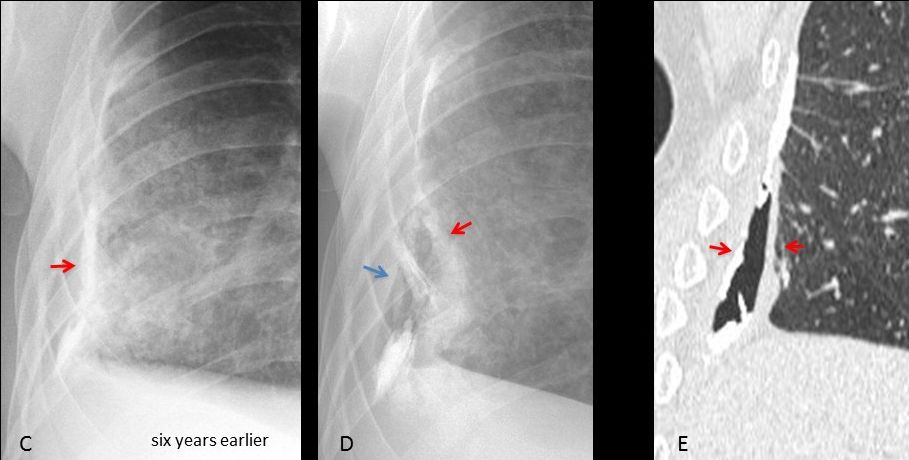
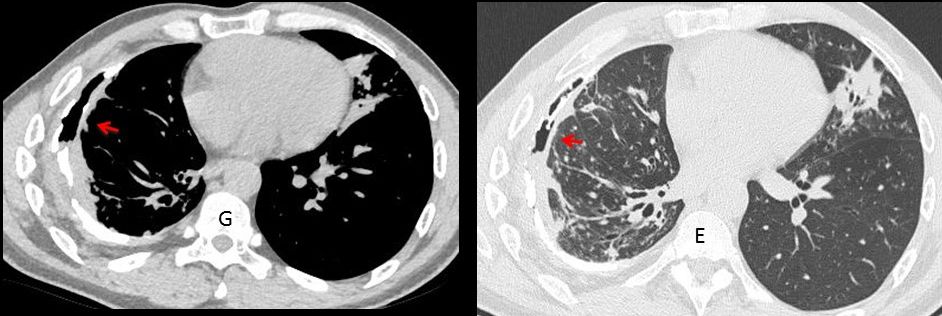
Unenhanced axial CT shows the global appearance of the pleura and B-P fistula (G-E, arrows) as well as the infiltrates in the left lung. BK was found in the bronchial lavage.
Final diagnosis: Bronchopleural fistula secondary to chronic pleural TB.
Congratulations to MK, who was the first to mention the correct diagnosis
Teaching point: air in the pleural space may come from the outside or the inside. If no invasive procedure has been performed, the most likely diagnosis is B-P fistula, excluding the rare occurrence of pleural infection by gas-forming organisms.



Hi! There is a loss of volume of the right hemithorax. There are thickened and calcified pleural plaques with an air density so hidroneumothorax is posible.
The right diagphragm is elevated because of the pleural and parenchimal changes.
In the right hemithorax there is a well defined high density that seems to be extrapleural.
In the left hemithorax there are some alveolar opacities.
Perhaps bronchopleural fistula? Any type of pleurodesis in the patient’s hystory?
Hi!
There is a homogenous radioopacity in the right hemithorax with silhoutting of right hemidiaphragm and a rising level along the lateral chest wall. A air fluid level seen suggestive of hydropneumothorax.There is thickening and calcification of pleura. most propably a chronic process.
Reticular and nodular opacities are seen in the right lung and few tubular and ring opacities in left lung. these could represent bronchiectatic changes with superimposed active disease.few nodular densities are seen in hila especially in lateral view, likely lymphnodes.
probably a sequaele of a chronic infection like tb with superimposed reactivation. right hydropneumothorax raises concern for bronchopleural fistula in the absence of any intervention
Hi.
CXR(pa/lat)show diffuse tiny nodular infiltration at right hemithorax and
pleural calcification at right costophrenic area with blunt costophrenic angle.
multiple small rings at left lower zone.
my impression is pleural calcification with thickening of right costophrenic angle due to old empyema or pleural effusion.
suggestive of miliary TB or Koch’s lung and bronchiectatic changes ar LLZ
….Pregiatissimo PROF. ….quello che maggiormente mi colpisce, a carico dell\emitorace dx è che nonostante la pachipleurite calcifica non vi sia perdita di volume, ma anzi esso sembra pìù espanso del sx…..quindi qualcosa lo riempie…..infatti aria libera è visibile all’esterno delle calcificazionie e sembra raccogliersi anche in sede retrosternale alta in LL….quindi…….Dybala “soffre” molto il marcamento stretto, con i tacchetti dietro i talloni….quindi il marcamento del Barca deve essere a” contatto”…..
Hi,
right pleural effusion with coarse calcifications in the posterior costal pleura. bilateral interstitial nodular infiltrates are noted.
DD: asbestosis, parapneumonic pleural effusion with underlying old pleural calcification.
Thanks.
Right pleural effusion , coarse pleural calcification posteriorly, soft tissue mass with an obtuse angle along the lateral chest wall. Differentials include malignant mesothelioma, asbestosis, or sequel of infective etiology.
Right pleural effusion , coarse pleural calcification posteriorly, soft tissue mass with an obtuse angle along the lateral chest wall. Differentials include malignant mesothelioma, asbestosis, or sequel of infective aetiology empyema. Ct chest suggested.