Today I am showing a case from my good friend Jordi Andreu. Radiographs belong to a 52-year-old man with chest pain.
What do you see?
Check the images below, leave your thoughts in the comments section, and come back on Friday for the answer.
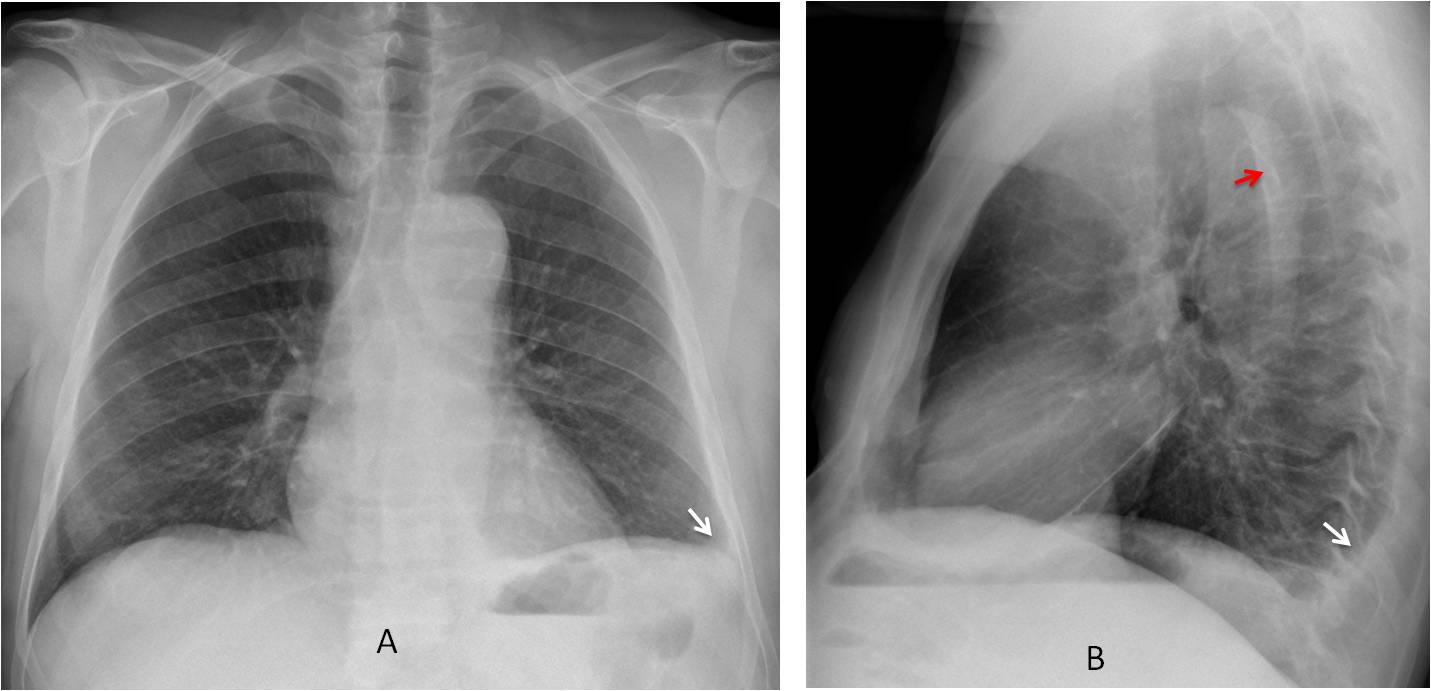
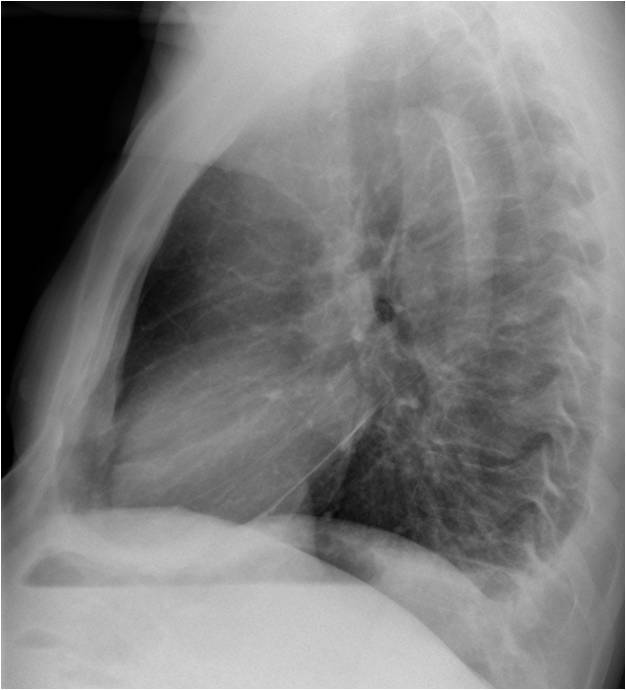
Findings: PA and lateral radiographs show a small left pleural effusion (A-B, arrows). Curvilinear intimal calcium within the aortic lumen is seen in the lateral view (B, red arrow). This finding is highly suspicious of aortic dissection.
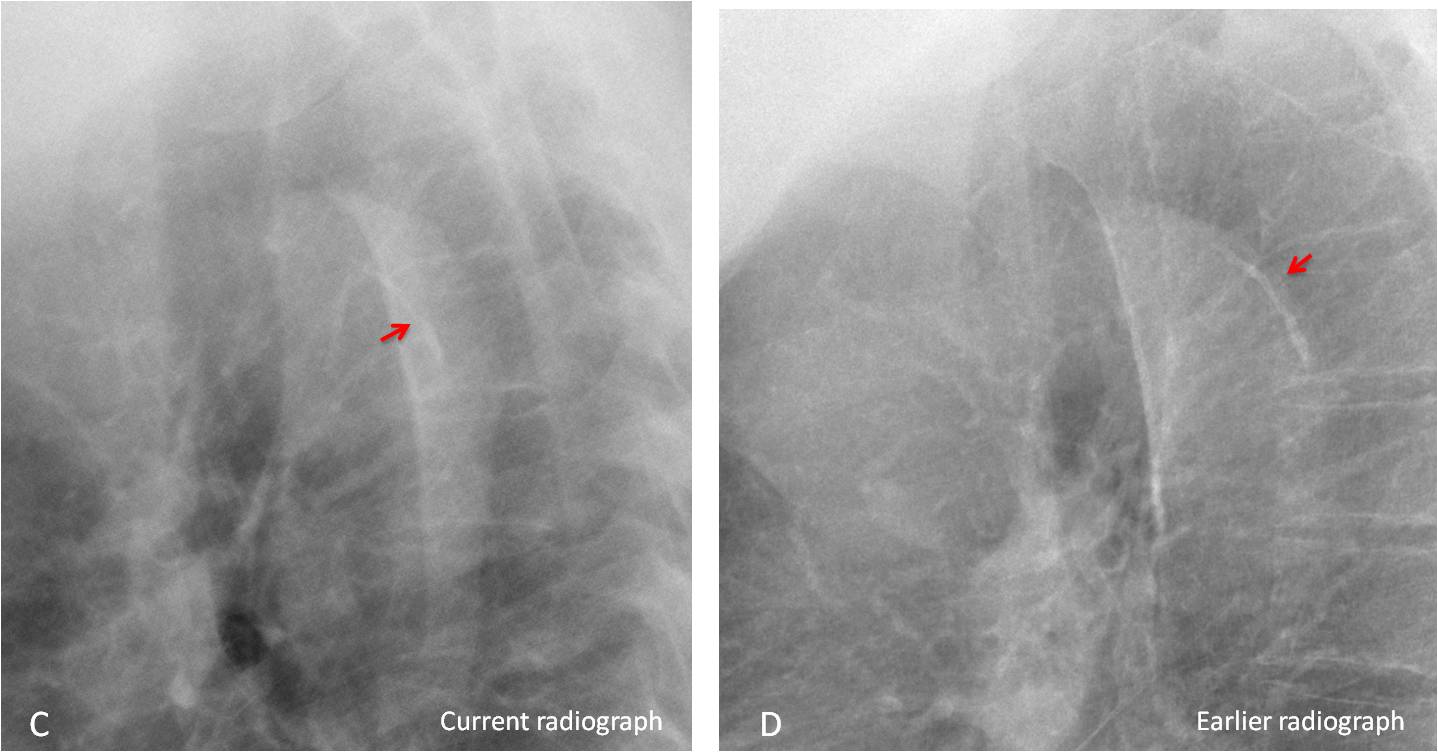
Comparison with a previous lateral view confirms the displacement of the intimal calcium (C, red arrow), which was located in the periphery in the earlier film (D, red arrow).
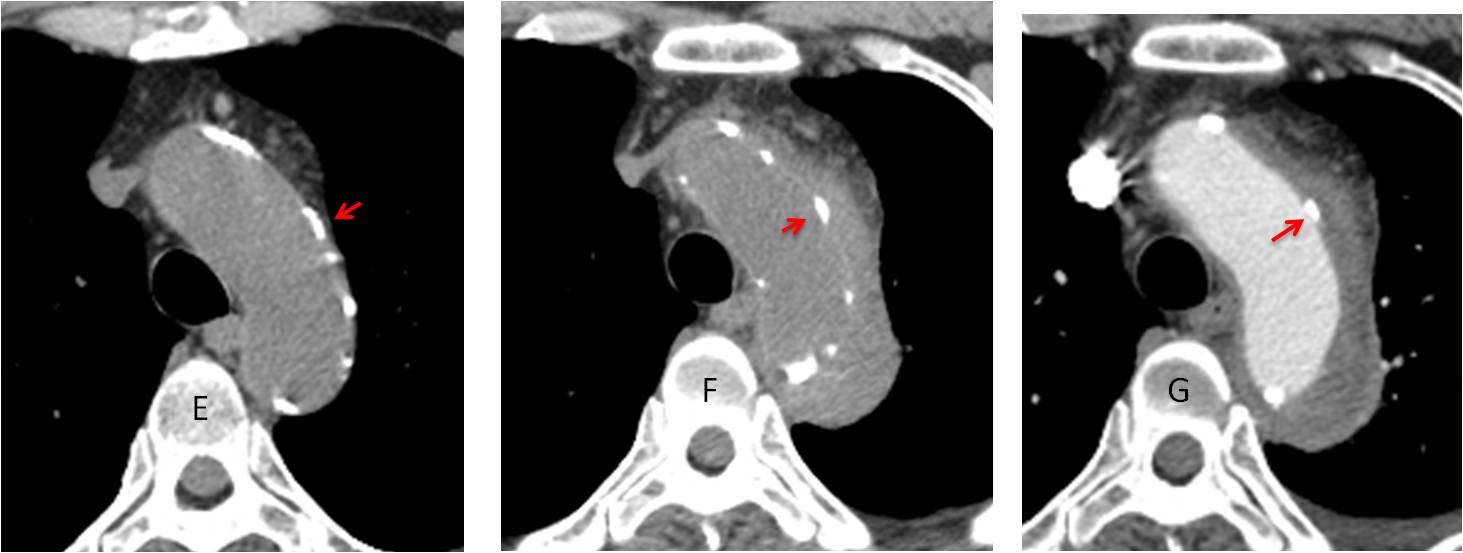
A previous axial CT shows the calcium in the aortic wall (E, arrow). Current CT shows the dissection surrounding the aortic lumen with the calcium displaced inward (F, arrow). Enhanced CT confirms the findings (G, arrows).
Final diagnosis: acute type B aortic dissection.
Congratulations to all of you who made the diagnosis, led by MK, who was to first to mention it.
Teaching point: this is a nice example of the value of the lateral view and of comparing with previous studies. This led to suggest the right diagnosis, later confirmed by CT.



Good morning!
There is an obliteration of the left costo-phrenic angle (pleural fluid and/or laminar atelectasi) and an enlarged calcified aortic arch (in the lateral view the calcium is displaced to the middle lumen). This arch seems to be larger than the aortic root so we have to do a CT to look for aortic pathology type disection.
I see a nodular lesion proyected over the right heart, but I can´t see it in the lateral view.
I believe the nodular lesion represents the confluence of the pulmonary veins.
Thanks
The aortic knob o the PA is widened with what appear to be calcifications. On lateral view the descending aorta is widened and irregular. A contrast CT of chest is needed to rule out a dissection given the patient’s symptoms.
The left costophrenic angle is occupied on the PA. On the lateral it seems like there might be a small pleural effusion or pleural adhesions in the posterior recess.
Agree with MP, aortic dissection. At the lateral view the calcifications on the posterior wall of the proximal descending aorta seem to be displaced inwardly. Nice!!
Lt CP angle blunted.
? Lt dome raised. Segmental collapse left lower lobe seen through heart on PA.
Unfolded aorta with mildly undulating posterior margin but not enough to be labelled coarctation. Hypertensive?
Effusion / thickening making visible inferior part of the oblique fissure.
Appearance of clavicle – ?anatomical variation or old healed fracture.
There is an obliteration of the left and left posterior costophrenic angle likely pleural effusion. Enlarged aortic arch with displacement of calcium to the middle lumenin lateral View aortic dissection to be ruled out
Hi,
flattening of the left hemidiaphragm with obliteration of the posterior costophrenic recess, apparently by a soft tissue lesion.
it does not look like effusion, i think diaphragmatic rupture is the main consideration.
thanks
No previous history of trauma
hi,
prominent calcified aortic arch with double contour of the upper descending aorta suggesting aortic dissection with associated left pleural effusion.
Better
Both lung zones are clear.
Frontal and lateral cardiac dimensions appear normal.
Obliteration of left CP angle may suggest left basal effusion.
Both hilum is normal in position and density.
Both hemidiaphragm appear normal.
Subtle hyperlucency with air shadow adjacent to the gastric bubble in the left hypochondriac region may suggest splenic abscess.
Soft tissues of thorax appear normal.
Bony thorax appear normal except for the old healed fracture of right clavicle.
Associated with unfolding of aorta.
…..stimatissimi colleghi…..il dolore toracico acuto, può’ essere causato da uno dei tanti organi nel torace…..esclusi il polmone, la pleura(esiti) a Sx, il cuore e le coronarie, l’esofago, non rimane che la patologia aortico…..nel caso in esame , oltre ad un aumento di calibro dell’arco, ed un “doppio ” contorno dell’ arco in. AP, vi è ‘ un segno patognomonico per dissezione tipo A….la dislocazione “mediale” delle calcificazioni ateromasiche che ci indicano la dissezione……Prof. il Bari ha terminato il campionato con un fallimento totale…..ricorda la Iuve., bloccato Dybala, e’ in estremo affanno, …..Bari ed il G 7 ti salutano….
As a Spaniard I want Real Madrid to be champion.
Sorry about Bari…