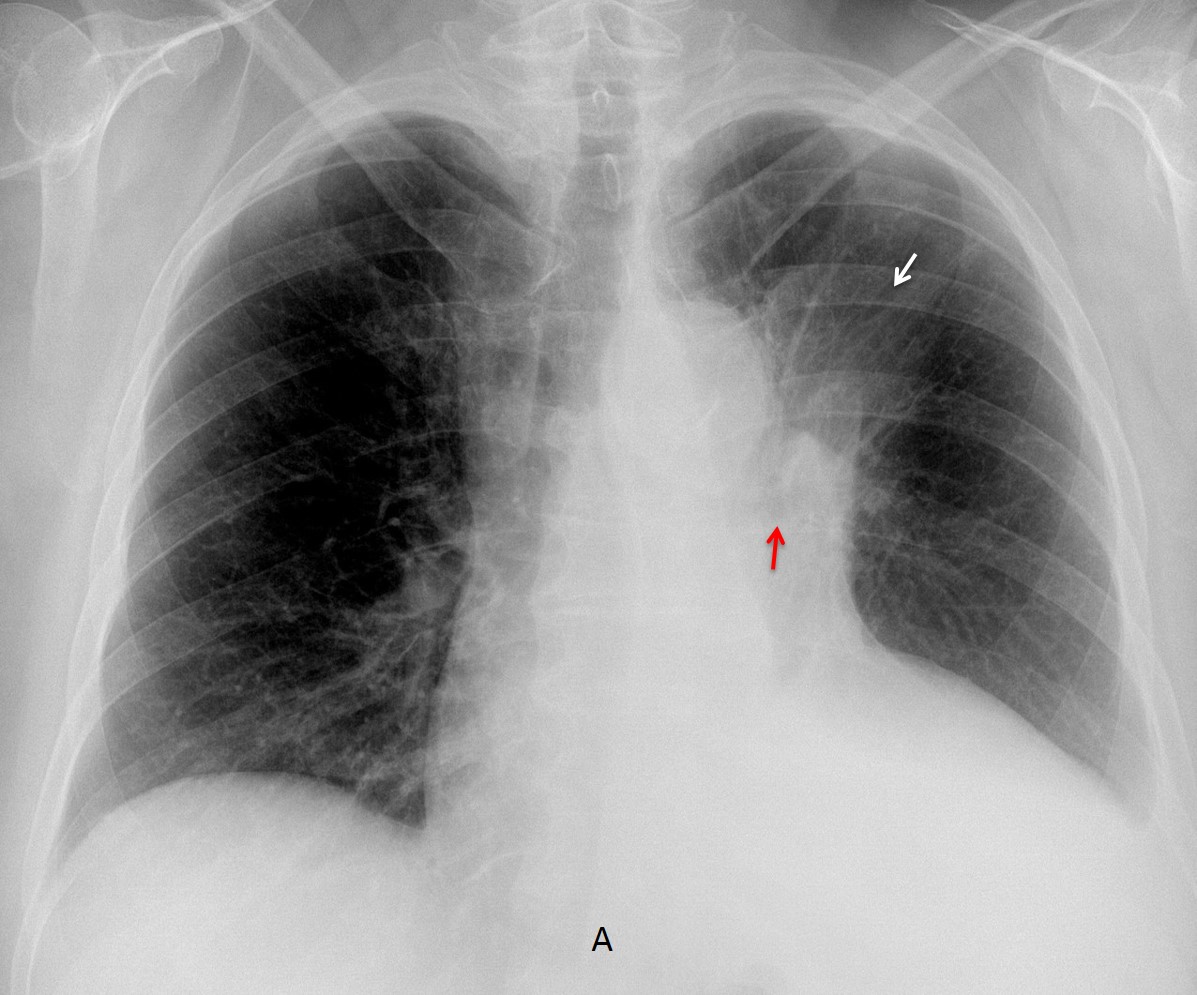
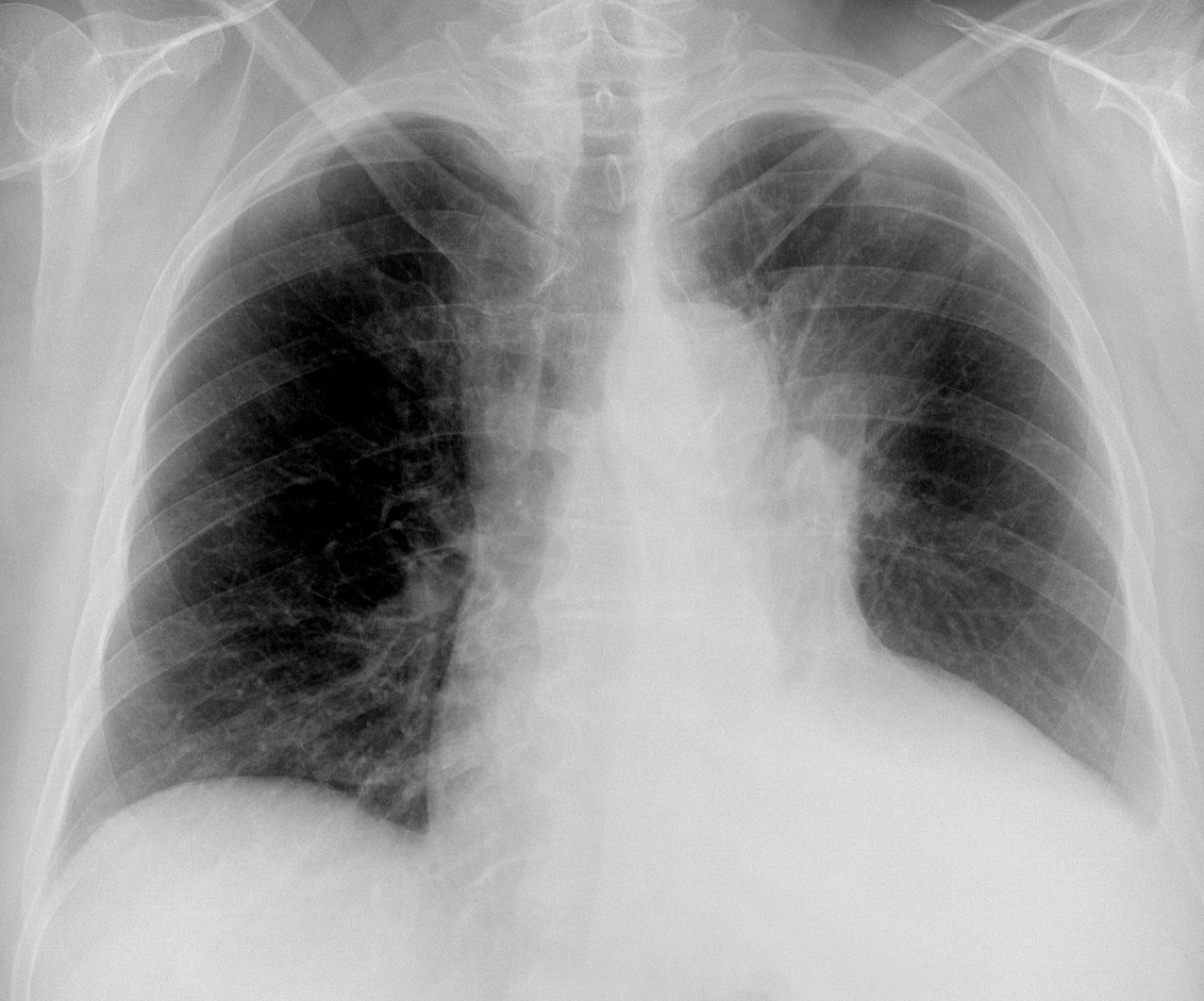
Today I want to test your prowess in plain film interpretation. The PA radiograph belongs to a 79-year-old woman with a cough and haemoptysis. What do you see?
Check the image below, leave your thoughts in the comments section, and come back on Friday for the answer.
Findings: PA chest radiograph shows an ill-defined pulmonary opacity in the left upper lung (A, arrow). The left hilum is elevated and the left main bronchus is arched upward (A, red arrow). This combination of findings is highly suggestive of LUL collapse. There is also blunting of the left costophrenic angle, indicative of pleural fluid and apparent cardiomegaly.
Enhanced CT confirms the LUL collapse (B, arrow), due to a mass at the origin of the LUL bronchus (C, arrow). An interesting finding is that the heart is of normal size (B-D, red arrows).
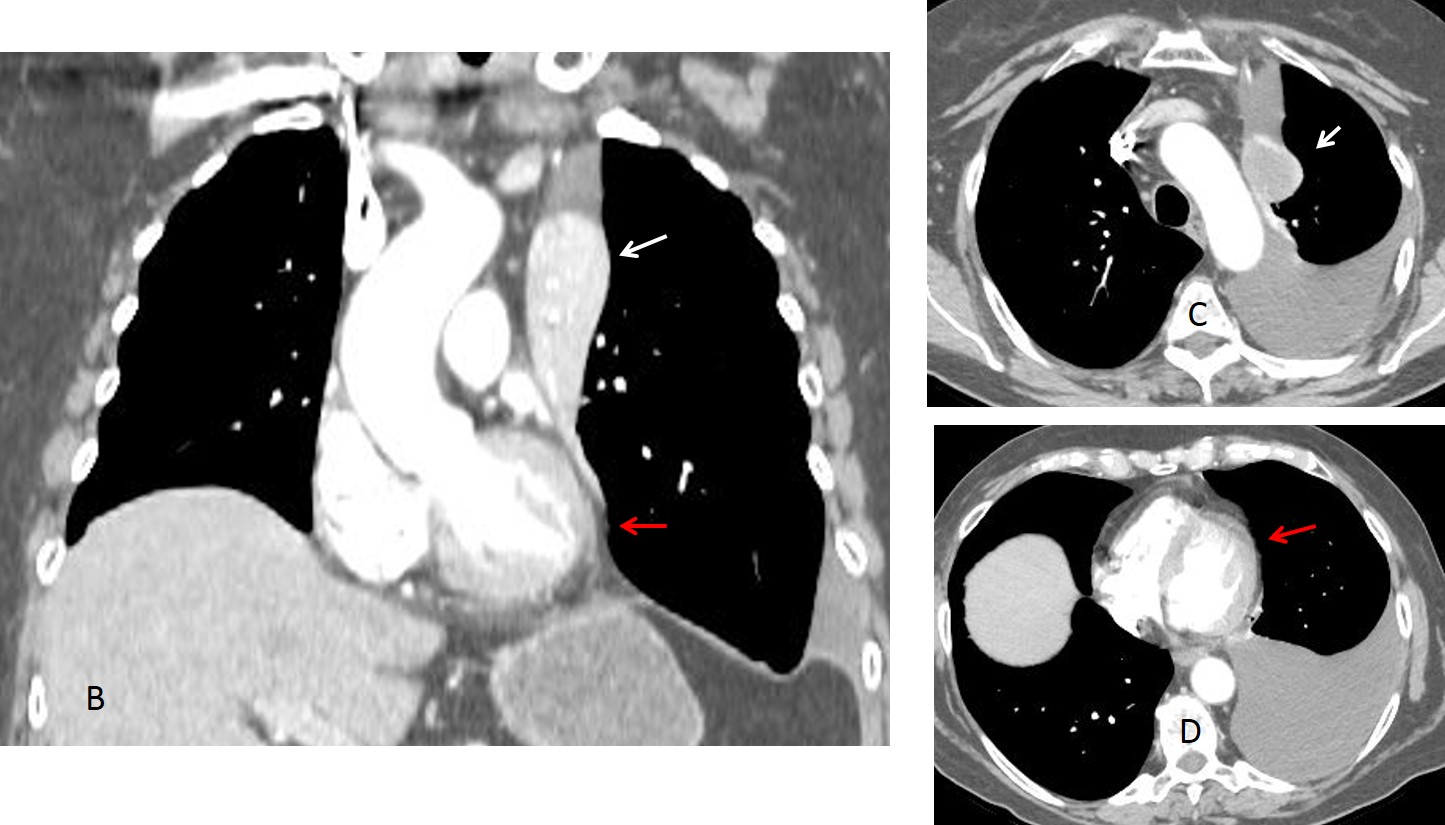
The apparent cardiomegaly is due to the apposition of pleural fluid over the cardiac shadow in the upright chest radiograph. This happens occasionally and you can see two examples in Diploma case 85. I don’t know if this has been reported in the literature.
Final diagnosis: carcinoma with collapse of LUL and pleural effusion simulating cardiomegaly.
Congratulations to TR, who was the first to suggest the diagnosis, although the rest of you did very well too.
Teaching point: it is important to recognise the signs of LUL collapse in the PA view, because carcinoma is the most common etiology. An added bonus in this case is remembering that left pleural effusion may simulate cardiomegaly in the upright PA view.


Greetings,
-poor inspiratory effort
-Enlarged cardiac silhouette.
-blunting of the left lateral recess.
-oblique vertical line over the left side of the mediastinum giving an impression of a triangular retrocardiac opacity, it might be a deviated anterior junctional line.
-deformed appearance of the left hilum with hazy illdefined opacity above it, and looks mildly superiorly displaced.
-Aortic konb margin is clear.
-no mediastinal shift.
Impression: the findings are quite confusing, and i suggest left upper lobe collapse with associated left pleural effusion, and compensated cardiomegaly.
No lateral? 🙂
Left hilus slightly enlareged and irregular with increased vascular markings in lul, and possible left sided effusion.
Slight ipsilateral mediastinal shift to the left.
Could be a mass obstructing bronchus for apicoposterior segment of lul.
No lateral view was taken. But you didn´t need it to make the right diagnosis 😉
There is a loss of volume of the left hemithorax and an increased density proyected over the LUL. The left bronchial is horizontalized and elevated, perhaps thinner than the right one. I think that endobronchial/hiliar lesion is a good option with secundary atelectasis.
I can see an abnormal line that is proyected over the aortic knob and goes down…
The prominent aortic knob desplaces the trachea to the right side.
Probable cardiomegaly in spite of the poor inspiration.
The left hemidiapghram is not visible (sillhouete sign). Something happens with the LLL.
I believe the left hemidiaphram is obscured by the pleural effusion.
Left side volume loss with elevated diaphragm and elevated hilum, hilar opacity without clear upper margin, hazy opacification in the left middle and upper zone – all point to LUL collapse.
We think there is left side loss of volume with an opacity of LUL, that can be an partial collapse. There is also left side effusion. Allergic bronchopulmonary aspergillosis and lung mass are diagnostic possibilities.
Rotation toward left side results jazzy left co angle
Despite rotion t would suggest presnce of subtle mass lesion in left hula
Ct suggest for confirmation
Rotated image.
Left upper lobe collapse.
Left sided pleural effusion.
Cardiomegaly possibly due to mitral valve disease.
Calcifications in the aortic knob.
Degenerative changes of the spine.
LLL collapse (sail sign?) due to central mass that obstruct the the left main bronchus which is not clearly visible.
Cardiomegaly.
Left pleural effusion.
The patient rotated a little bit to the right.
LLL collapse would be not compatible with an elevated hilum, unless you are thinking of a torsion of the lobe.
Interesante como siempre 😉
cardiomegally (ventricular ) , pulmonary hypertension with left upper lobe collapse