Today I want to try a new way of presenting cases: conventional PA and lateral radiographs will be shown on Monday, followed by additional images on Wednesday. Hope this approach will have more educational value. If it works well, I will do it more often.
Today’s radiographs belong to a 74-year-old woman with mild respiratory infection.
As promised, here are two additional images of the enhanced CT. Are they of any help?
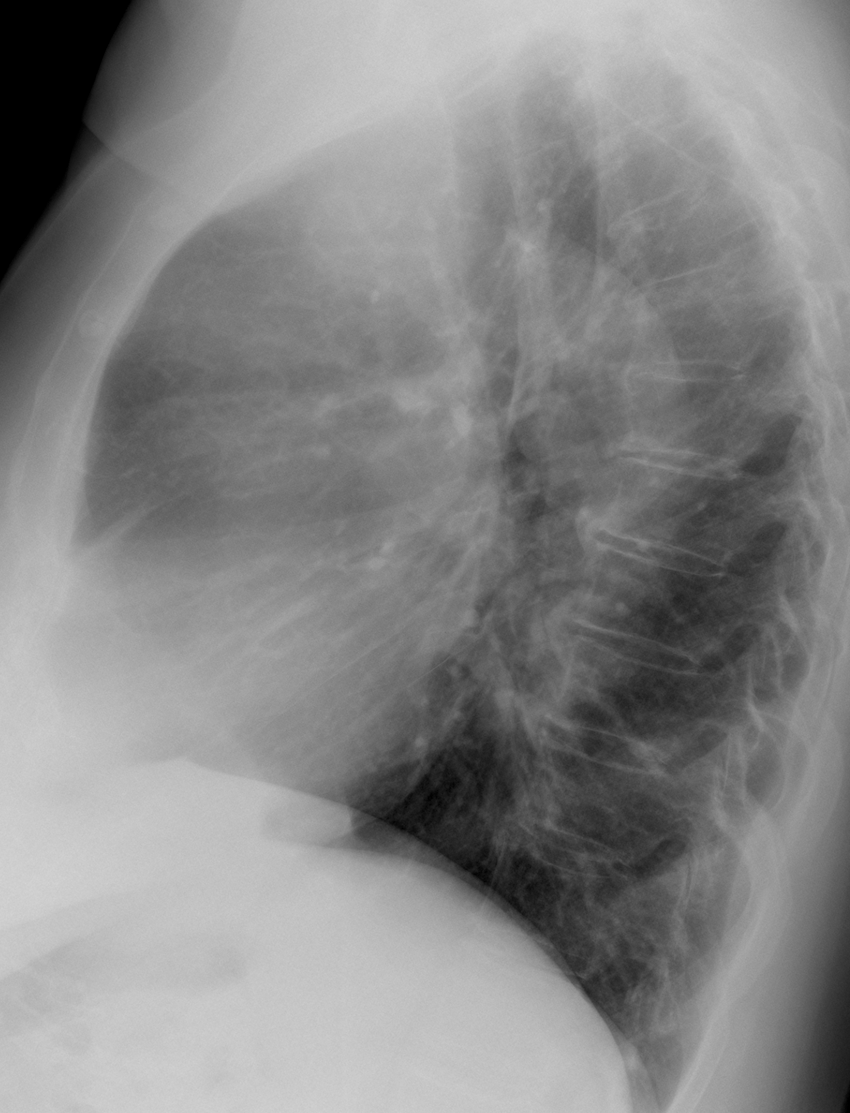
Findings: chest radiographs show a superior/anterior mediastinal mass projected over the aortic knob (A-B, arrows).
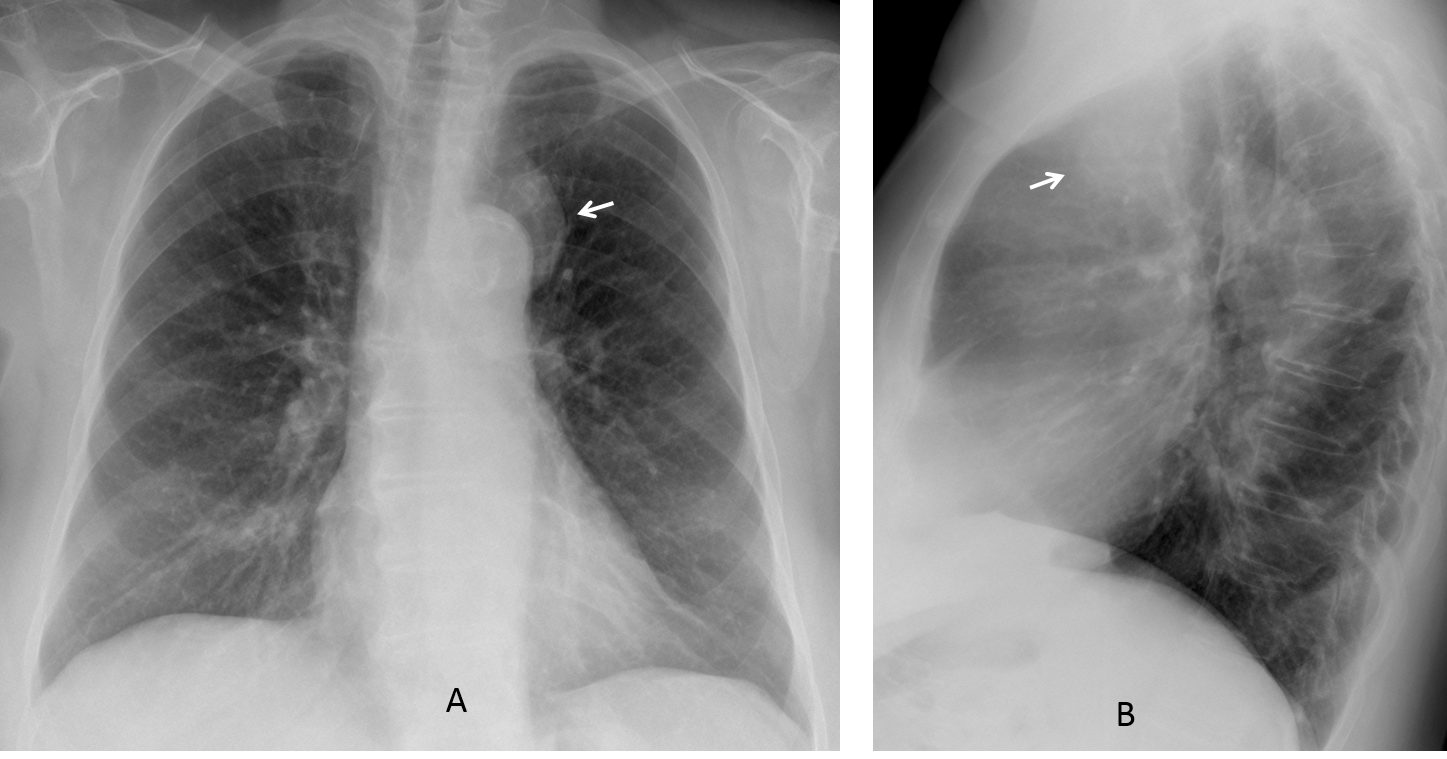
The classic differential diagnosis of a mass in this location lies among thymoma, embriogenic tumour and lymphoma (less likely because of the paucity of symptoms). Intrathoracic goiter would be unusual in front of the trachea.
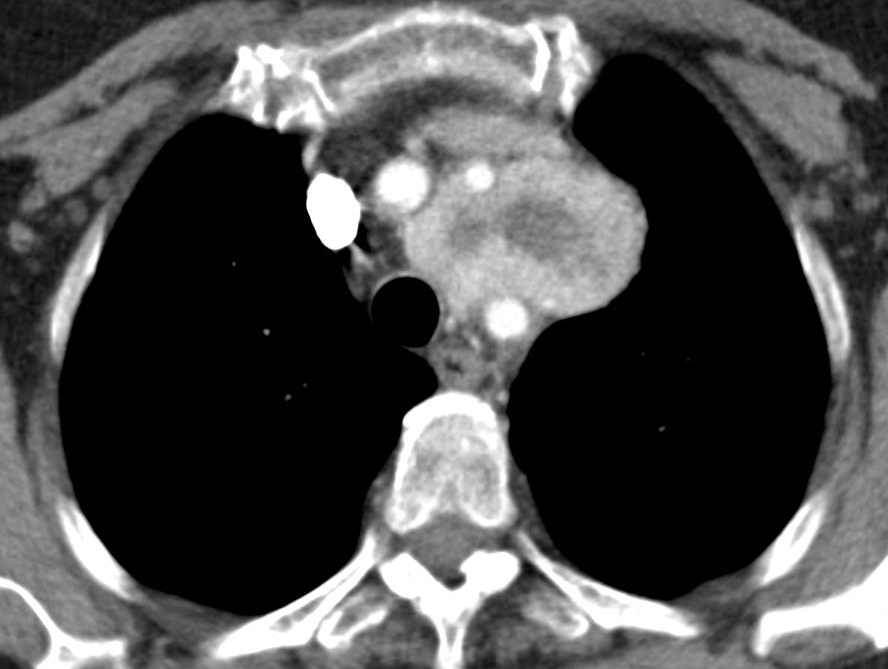
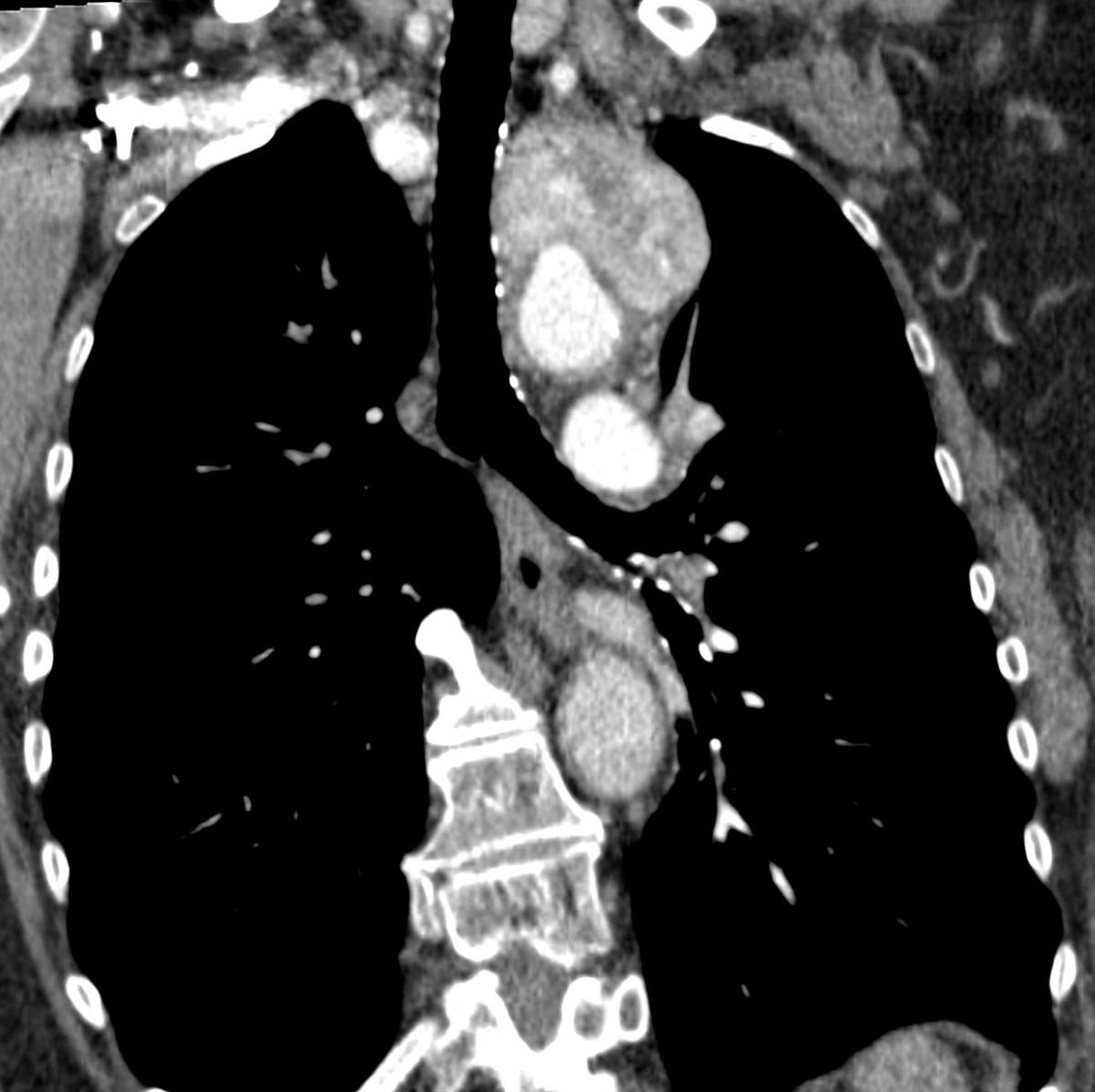
Enhanced coronal and axial CT show an intensely enhancing mass with necrotic center located between the supra-aortic vessels (C-D, arrows).
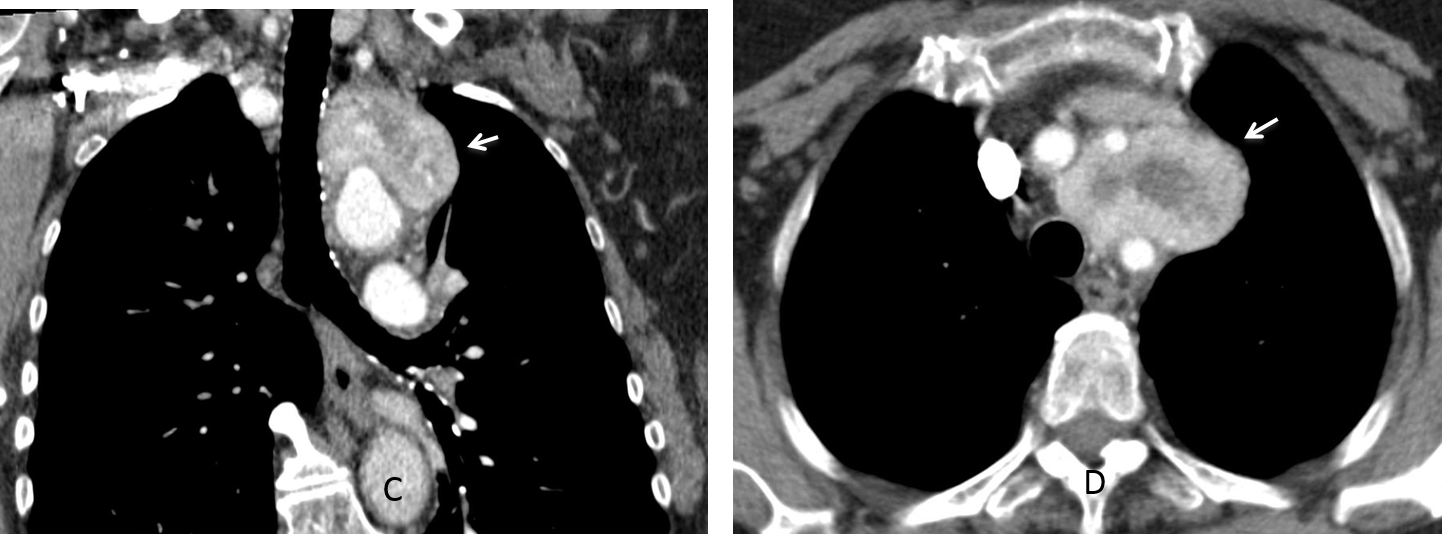
The differential diagnosis of avid enhancing mediastinal masses includes thyroid, paragangliomas and Castleman disease. In this particular case, the location between the vessels favors the diagnosis of paraganglioma.
SPECT-CT with (111)In octeotride shows marked uptake of the mass (E-F, arrows).
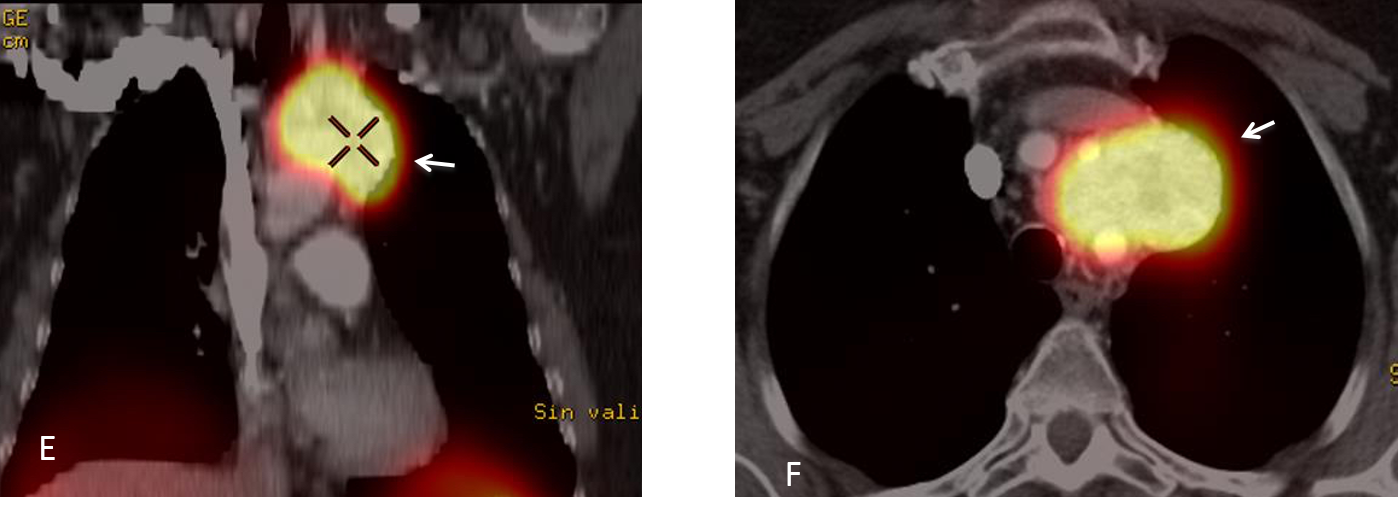
Final diagnosis: paraganglioma of upper mediastinum.
Contratulations to TR, winner of the first phase, and MK who made the correct diagnosis.
Teaching point: Remember that an avidly enhancing mass in the mediastinum, suggests endothoracic goiter as the first possibility, followed by paraganglioma and Castleman disease.
My heartfelt thanks to Dr. Eva Castañer, who provided the CT and SPECT images.



Good morning,
There is an anterior mediastinal lesion, nex to the aortic knob. There are anomalous calcifications displaced into the aortic lumen. I am between aortic pathology (disection-pseudoaneurysm) vs mediastinal lesion.
There is an increased density in the anterior clear space
Left Subclavian artery pseudoaneurysm, better than aortic….
Don’t you find strange that the aorta is calcified and the aneurysm is not?
Yes, but not atherosclerotic causes are possible… Something that does not fit with the vascular diagnosis is the opacification of the anterior clear space…
I think I have to wait until wednesday…
greetings,
left superior mediastinal opacity seen on the PA view with preserved outline of the aortic arch, and on the lateral view located anterior to the trachea. aortic arch calcification noted.
Impression: anterior mediastinal mass, the main differential diagnosis:
Thymoma, germ cell tumor, T-cell lymphoma, and intrathoracic thyroid.
Greetings,
I would like to add the false aortic aneurysm to the differential diagnosis.
thanks
I agree with MK and TR that there is a soft tissue density projecting to the left of the superior mediastinum. The margins of the aortic knob are sharply visible indicating the aorta and lesion are separate. Lateral confirms an anterior mediastinal density. Given the clinical information provided, I would be thinking of thymoma or germ cell tumor as suggested by TR. Lymphoma also needs to be considered until ruled out with further testing.
Considering the respiratory infection, there may also be some mild alveolar infiltration in the right lower lung zone on the PA, but my eyes may be playing tricks and these are only pulmonary vessels 🙂
I believe your eyes are playing tricks 😉
Greetings,
I would like to say that since the lesion looks clearly well-defined/oval on the lateral view, I think it is appropriate to consider the pulmonary lesions also, anterior segment of LUL.
So the differential diagnosis would be: the 5Ts of the anterior mediastinum and the LUL/anterior segment mass.
thanks
When I saw the case I considered a pulmonary lesion as well, but I discarded it. The appearance in the lateral view suggests a pulmonary lesion because the outer portion of the mass is surrounded by air.
Hello, in here there is a superior mediastinum opacity near aortic arch. Differential Ds: bronchogenic cyst, lymphoma.
There are also bronchiectases at the right lower lobe.
According the chest x-ray and comments above I propose mediastinal type cancer. Lesion has both signs so mediastinal mass with obtuse angles and is surrounded by lung parenchyma on lateral view
When I saw the lesion I was not completely sure that it was not in the lung. I agree with your comment.
CT will be shown today.
In addition, I thought also about the mediastinal lesion for differential diagnose
….Magico PROF…..linfoadenopatia di Castleman…
There is a solid lesion with necrotic center between subcalvian and left carotid artery. Perhaps paraganglioma?
I can not support Castleman lymphadenopathy while it is more associated with immunocompromised patients (mainly HIV) and this patient is 74, in this case this is focal lesion, and mostly this lesions have homogeneous intensive enhancement (the differential feature), – but, due to the only two demonstrated CT images, I should ask whether there were multifocal changes find or not?
Mass has well defined contours but not smooth (somewhat spiculated?), heterogeneous enhancement like a thick ring with central hypoattenuation – necrosis and mass effect on the surrounding vessels – shifting left common carotid artery to the front and left subclavian artery backwards – I agree with MK, it is most typically for paragangliomas – is there any information about pheochromocytoma?
I do not know whether my eyes are playing tricks but it seems the mentioned vessels and brachiocephalic artery though are enhanced but have irregular inner contours?
Still top differential:
1. Paraganglioma
2. Lymphoma (additional information needed – other probable extramediastinal lesions?)
3. As sad, mild infection in anamnesis – bacterial (non specific/specific – tbc ) etiology – abscesse?
4. Other: germ cell tm
Oh! And metastasis
Greetings,
avidly enhancing mass with central hypodensity between the left CCA and the left subclavian artery, and abutting the aortic arch.
I think the most likely diagnosis is paraganglioma/neuroendocrine tumor, and secondly the intrathoracic gioter.
This is a tough one but I am thinking invasive thymoma vs paraganglioma.
I would say that the marked enhancement points to a paraganglioma
….quasi goal….nessuno aveva pensato a Castleman…grazie sempre PROF!!!!