Dear Friends,
Presenting the last case before Summer vacation. Muppet needs quality time to replenish his energy (July and August) and will return in September with more interesting (and teaching) cases.
These radiographs belong to a 52-year-old male with a cough. The answer has now been added, but you can still leave your thoughts and diagnosis in the comments section, below, before you check it.
Diagnosis:
1. Mediastinal fat
2. Dilated SVC
3. Lymphoma
4. None of the above

52-year-old male, PA chest

52-year-old male, lateral chest
Click here for the answer to case #72.
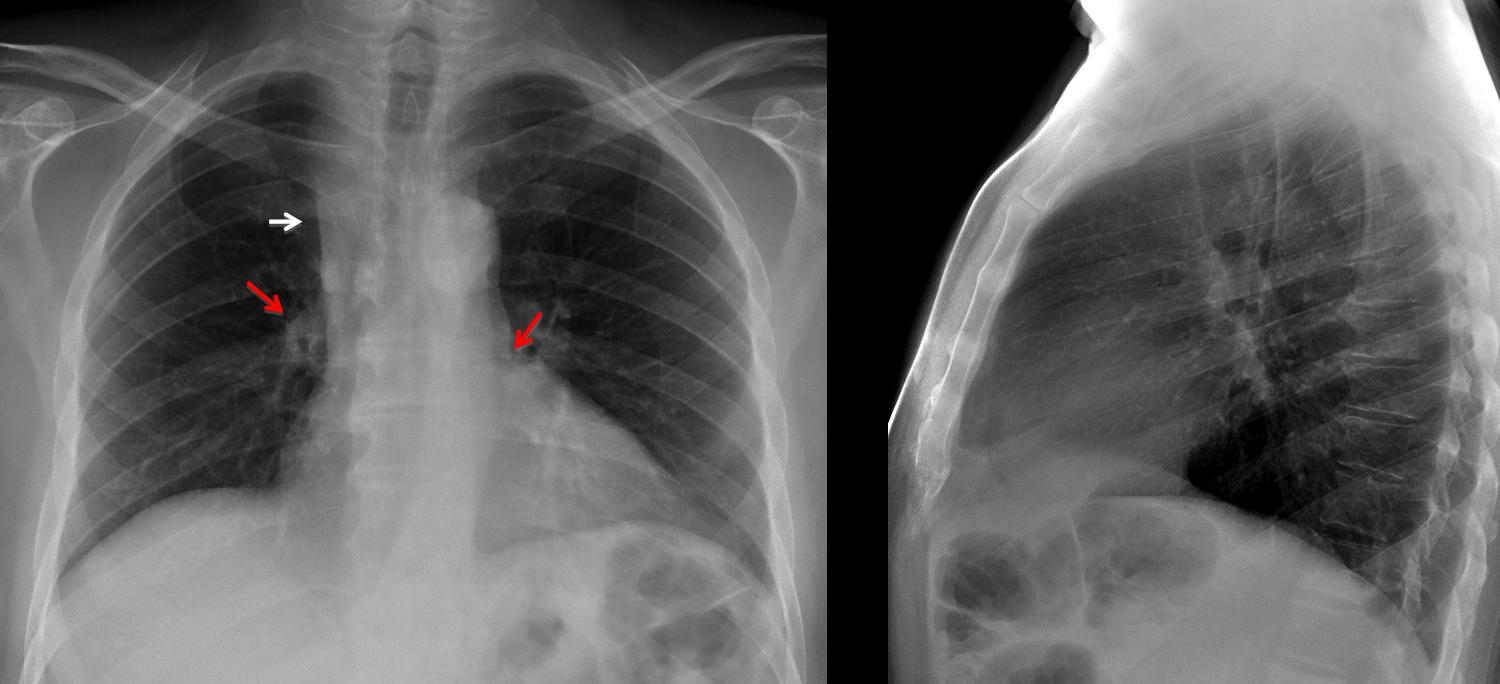
Findings: PA chest shows widening of the right upper mediastinum (arrows). The first diagnosis that comes to mind is enlarged lymph nodes. Other possible causes are an enlarged vena cava or mediastinal fat. The clue to the diagnosis lies in the right hilum, which is higher than the left (
red arrows).
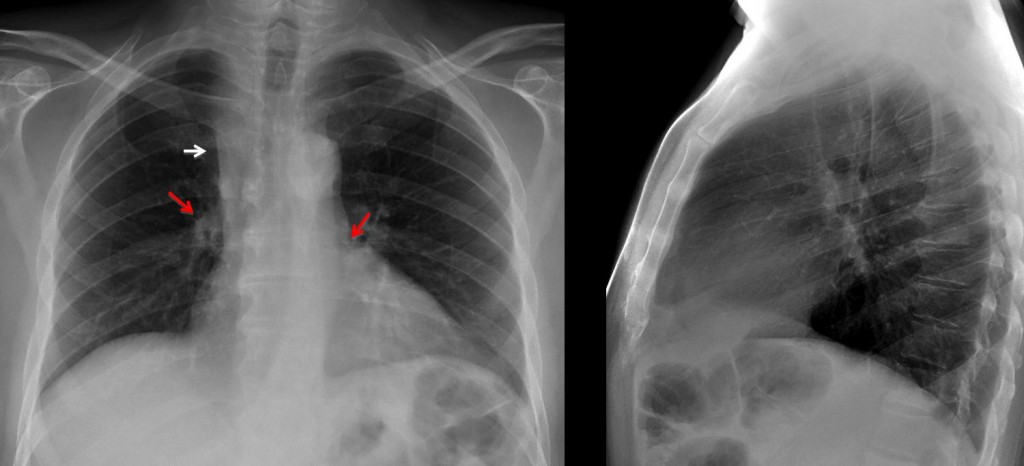
At no time should this occur, which raises the possibility of loss of volume of RUL pulling up the right hilum. Coronal CT shows marked collapse of RUL which is visible as a thin stripe apposed to the mediastinum (A, arrows). Coronal reconstruction shows the obstructed bronchus (B, yellow arrow) leading into the collapsed RUL (arrows).
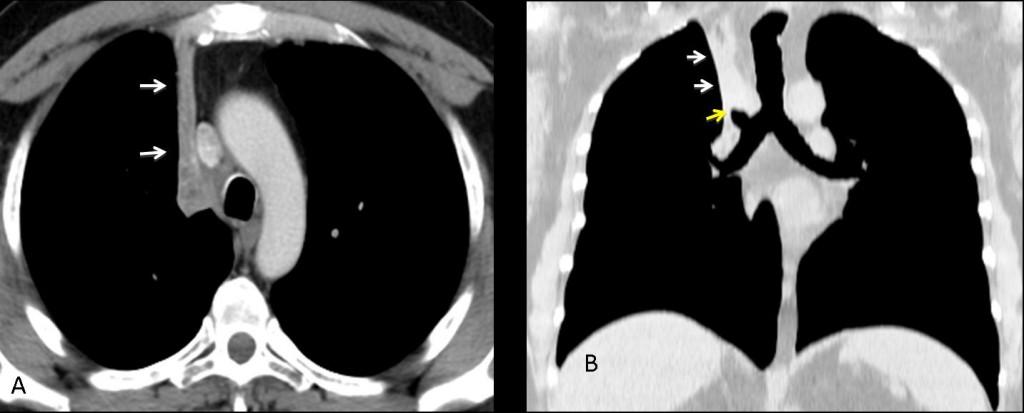
Final diagnosis: marked RUL collapse, secondary to bronchial carcinoma.
Congratulations to Alice, who suggested the correct diagnosis.
Teaching point: do look at the hila. They may provide important information.
Muppet wishes you all a pleasant vacation!





chest x ray frontal and lateral views .
expiratory view
widening of superior mediastinum with straight radial mediastinal border . extending above clavicle ,so it is middle or posterior mediastinal lesion.so dilated SVC , or excessive mediastinal fat .
however i will repeat the frontal view in full inspiration , then ct scan may be advisable
pericardial effusion
Posterior displacement of epicardial fat pad by effusion on lateral view.
Convendría una proyección en inspiración pero lo mas probable es que sea una vena cava superior dilatada
There is widening of the paratracheal stripe extending above the clavicle, suggesting (as Ashraf Abohadeed already mentioned)a middle or posterior mediastinal lesion, but I think there is also an retrocardiac opacity as well as an enlarged left hilum .
I cannot distinguish the major fissures in the lateral view, but I think that there is a downward displacement of the left hilum.
So, may be it is a LLL lung carcinoma with left hilar and right mediastinal lymph node metastases.
The lef hilum may be displaced downward or…
….. or the right hilum upward
I think the opacity is anterior obliterating the retrosternal space in Lat. view , it is homogenous with sharp Rt border in PA film , no tracheal shift , no other abnormalities …
so mediastinal fat may be the most likely choice.
Quello che colpisce, a prima vista, è lo svasamento mediastinico alto a dx, con lieve medializzazione della trachea.Inoltre , sempre in AP, attraverso l’ombra cardiaca, si vede una irregolare opacità, sotto l’ilo di sx , che pertanto è “slivellato”, rispetto al destro.In LL ,il profilo inferiore dell’ombra cardiaca è sfumato, mentre il bronco principale di sx non è altrettanto ben definito.Penso allora che Katarina ha visto bene, formulando la diagnosi di CR polmonare ilare sx, con linfoadenopatie mediastiniche.NB. Alice è già in vacanza?
no not on holiday -yet! 😉 cheers
What is that drop-like nodule at the right border of the opacity ?
Another dense azygos lobe ?
The opaque azygos lobe is less dense in its lowermost aspect. Answer tomorrow
This hyperlucent lesion retrocardiac in the base with the retraction of the left hilum could be a intralobar seqestation?
small segment of pulmonary vessel narrowing in left perihilar region most likely extrinsic along with distended SVC.
? pulmonary arteriovenous communication.
adding to my previous comment buldging right heart border seen in PA view ,and prominent IVC seen on lateral view reflect increased burden on right atrium
late again i am really busy right now
i will have to think some more one this one but could it be right upper lobe atelectasis?
there seems to be volume loss of right lung
right hilum seems to have moved upwards
Bravo! CT tomorrow
grazie “mitico” del suggerimento a Katerina( e faccio mia l’osservazione di Alice): e se il tutto fosse un mediastino “vascolare”?. Un doppio arco aortico,spiegherebbe lo svsamento mediastinico alto a dx, con lieve medializzazone della trachea e l’ilo sx più piccolo, ovvero uno “sling” dell’arteria polmonare sx.N:B. il dottor Ricardo Pruna(FBC Barcellona), il 27 settembre a Bari, per un convegno di ecografia sportiva.Buone vacanze a te ed a tutti i cari colleghi.
Bravissima Alice! Regola kiss è stata rispettata:pensare sempre alle cose SEMPLICI !Atelettasia lobo superiore dx, con ilo dx stirato in alto.