This week Muppet and I are going on a dangerous trip abroad. Forgive me if I answer your comments a little bit later than usual; the locals may be hostile and refuse to share their WiFi.
Radiographs belong to a 73 y.o. male with fever and symptoms of acute prostatitis.
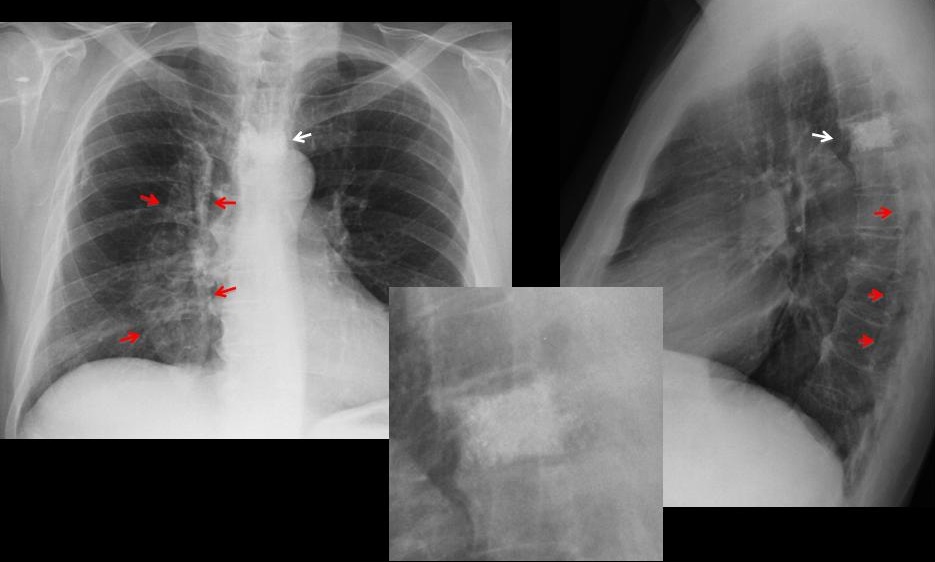
The obvious finding is the increased density of the fifth dorsal vertebra (Fig 1, arrows). The vertebral body has ragged borders with metallic opacities within and it’s smaller than the ones above and below (insert). The initial impression is osteoblastic metastases, supported by a clinical history of prostatic disease. However, the metallic opacities and the shortening of the vertebral body suggest a previous surgical procedure. Review of the clinical history revealed that surgery for a vertebral hemangioma had been performed several years ago (probably vertebroplasty).
There is also a right paramediastinal calcified ovoid opacity in the PA view, barely visible in the lateral view as a posterior dense line (Fig 1, red arrows).
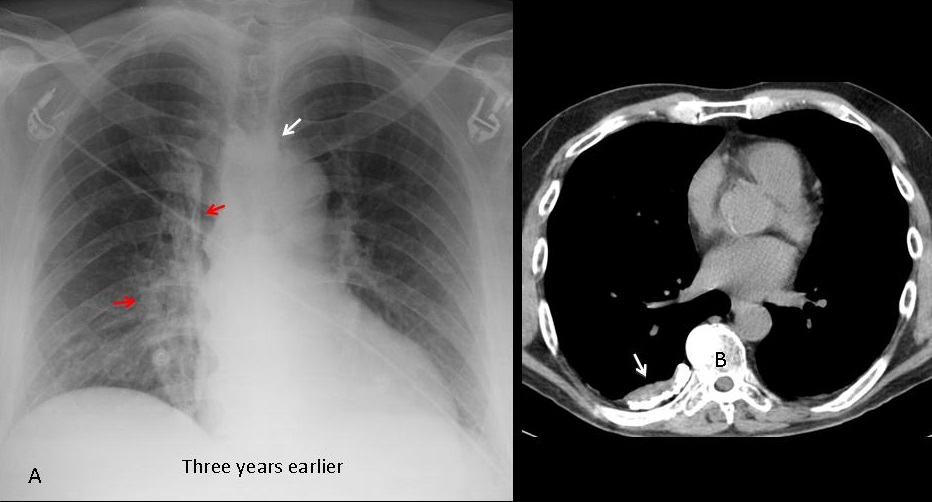
It has the appearance of pleural calcification, confirmed by upper slices of an abdominal CT performed at the time of admission (Fig 2B, arrow). Patient had a history of pneumothorax in his youth.
A previous AP radiograph three years earlier confirms that the pleural opacity and the dense vertebra were present and unchanged (Fig 2A, arrows).
Final diagnosis: Iatrogenic dense vertebra (probable vertebroplasty). Unrelated pleural calcification.
Congratulations to Katherina, who was the first to make the correct diagnosis.
Teaching point: always remember that iatrogenia may cause any type of finding, especially when metallic opacities are visible. And remember that all visible findings do not have to be attributed to a single disease.




Sclerotic appearance of TH4 vertebra with normal appearance of TH3 and TH5 vertebrae.
The findings could be suggestive of ivory vertebra (D/d lymphoma, myelosclerosis, osteoblastic metastasis, Paget disease, fluorosis and osteopetrosis), but ….
– In the profil view there is a small reduction of the height of the vertebral body of TH4 and stenosis of TH4-TH5 intervertebral space
– In the AP view I think that the upper borders of TH4 are not well defined
– I think that I see some very radiopaque regions in TH4, which may be due to foreign material (vertebroplasty?).
Moreover, there is an extensive pleural calcification in the right lung, a small sclerotic lesion in the right humerus and syndesmophytes in the right side of TH5-TH11.
I can’t figure out how acute prostatitis can be related to all these findings. Still thinking ….
we can see erosion of the posterior ribs on the right too.
scoliosis of the thoracic spine
bone metastasis from prostatic cancer – osseous tb
Dorsarthrose et condensation globale T4 faisant suspecter une métastase , peut être prostatique en l’absence de vertébropalstie antérieure
Calcifications droites d’allure pleurale
Dorsarthrose et condensation globale T4 faisant suspecter une métastase , peut être prostatique en l’absence de vertébroplastie antérieure
Calcifications droites d’allure pleurale
Vertebroplasty
right mediastinum enlarged, too.
Mets from prostatic cancer
What about reduced transparency of mediastinal shadow on the right?
Pleural calcification on the right.
Vertebroplasty Th4.
What about that sequence?
Previous injury- thoracic vertebral fracture – vertebral body collapse- vertebroplasty?
Injury- hemothorax- pleural calcifications?
But if the patient had no vertebroplasty, I would still go for a metastasis.
What about reduced transparency of mediastinal shadow on the right ?
By using the Ivory Vertebra sign as a starting point, plus the presence of fever with genitourinary symptoms, I think that a sclerosing osteomyelitis derived from haematologic dissemination from genitourinary infection is good option. But if I must explain the pleural calcifications, I would pick TB as etiologic agent, with prostatic, vertebral and pleural compromise.
The prostate cancer with osteoblastic metastases is a good combo too, but I can not explain the fever nor the pleural calcifications.
Greetings from distant Chile!!!
By using the Ivory Vertebra sign as a starting point, plus the presence of fever with genitourinary symptoms, I think that a sclerosing osteomyelitis derived from haematologic dissemination from genitourinary infection is good option. But if I must explain the pleural calcifications, I will pick TB as etiologic agent.
The prostate cancer with osteoblastic metastases is a good combo too, but I can not explain the fever.
Greetings from distant Chile!!!
There is something in the retrosternal space: is it a non calcified pleural thickening?
Those bilateral pleural calcifications indicate an old TB, or more unlikely asbestosis.
Sclerotic, slightly height-diminished T4 vertebra indicates either an osteoblastic prostate metastasis, or a vertebroplasty.
Therefore the most likely diagnosis: those findings don’t have anything to do with the acute prostatis and you tried to trick us 🙂
But we should check the patient anteriority to confirm that T4 underwent a vertebroplasty and that it’s not an osteoblastic disease.
I cant believe that is vertebroplasty. So good fill up with cement all over vertebral body… (to good to be true;)
but a sclerotic vertebral is not always a metastasis from a prostatic cancer or hematogenic spread from prostatic tb(rare) or something else. It is necessary the combination of these two findings in our case? Could be two separate pathologies?
Good Trip professor and Muppet!
Besides the Ivory vertebrae and pleural plaques, there are post-surgical changes in the posterior left arch of the 8º and 9º ribs. There is also high-mix density imagen projected over the right hemithorax (paravertebral), which some of his margins are well defined, and in the lateral view seems to be interposed to the aorta silhouette. Any more information about this patient?
Bilateral pleural calcification indicate an old TB.
Ivory, slightly height-diminished T4 vertebra indicate either a vertebroplasty, or an osteoblastic metastasis.
A little extra pulmonary opacity stands in the retrosternal space: is it a focal pleural thickening?
Stimatissimo professore, è chiaro che un esame anamnestico farebbe di per sé la diagnosi( il radiologo è innanzitutto un clinico):in mancanza di tali dati possiamo fare solo delle ipotesi sulla base della semeiotica x-grafica. in LL vertebra sclerotica, le cui cause sono molteplici, insieme ad interventi di radiologia interventistica , di cifo-plastica( in questo caso si è ripristinata anche l’altezza vertebrale.Vi è poi un “cage” a densità metallica sulla testa omerale, espressione di intervento di stabilità capsulare.Questi due dati potrebbero riferirsi ad evento traumatico pregresso.Vi è poi una opacita” a guscio di seppia” con calcificazioni in paraliare dx, espressione di pachipleurite calcifica;erosioni sul margine inferiore della 9 e 10 costa dx:questi due dati possono riferirsi ad altro evento patologico, con reliquati in tali sedi.Ripeto l’anamnesi aiuta.
Good trip sir
I think that there is a right middle zone pulmonary opacity with air bronchogram denoting consolidation masking the right cardiac border ( middle lobe pneumonia )
One of upper thoracic vertebrae shows vertebroplasty
Good trip sir I think that there is a right middle zone pulmonary opacity with air bronchogram denoting consolidation masking the right cardiac border ( middle lobe pneumonia )One of upper thoracic vertebrae shows vertebroplasty
May be a pulmonary embolism material vertebroplasty.
Muppet and I are safe in Vienna. Missed you all! See that you are becoming smarter by the day. Answer tomorrow. Promise I will never leave you again.
Pregiatissimo professore, ma vertebroplastica non è la stessa cosa di cifoplastica, che presuppone una prima fase di “riepansione” del corpo vertebrale, come in questo caso? La vite metallica sull’articolazione scapolo-omerale? Ripeto una “semplice” raccolta anamnestica ha fatto la diagnosi.
I could not be sure of the procedure. It was not specified in the clinical history. All I know is that the patient had a surgical procedure in the vertebra several years ago and thah the previous radiograph was unchanged