
Dear Friends,
To compensate for the subtle findings in the previous case, I am presenting an obvious one in a 69-year-old man with chest pain. What would be your diagnosis before CT?
Check the images below and leave your thoughts in the comments section. The answer will be added on Friday.
1. Endothoracic goiter
2. Aortic aneurysm
3. Thymoma
4. None of the above

69-year-old man with chest pain, PA chest
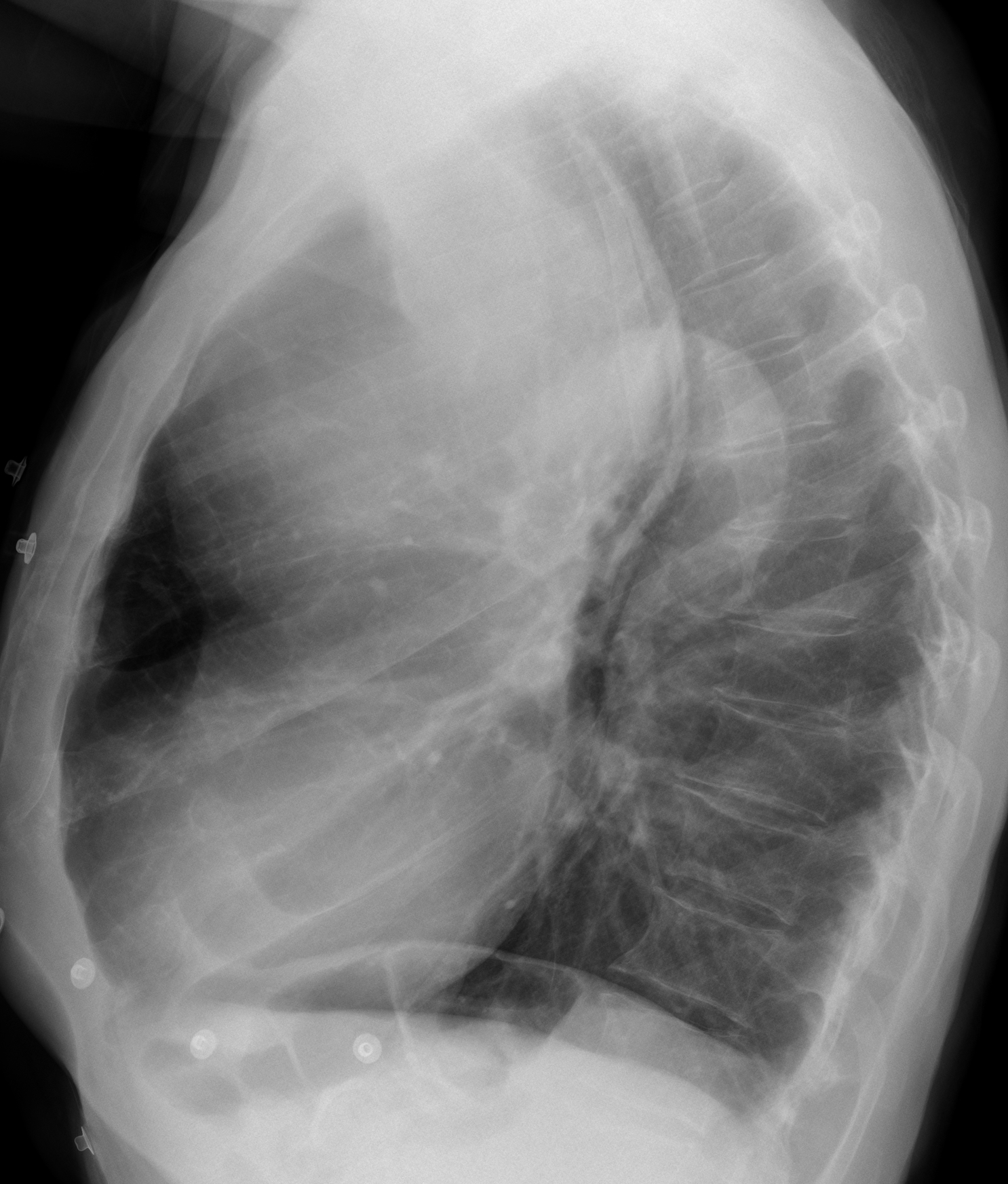
69-year-old man with chest pain, lateral chest
Click here for the answer to case #79
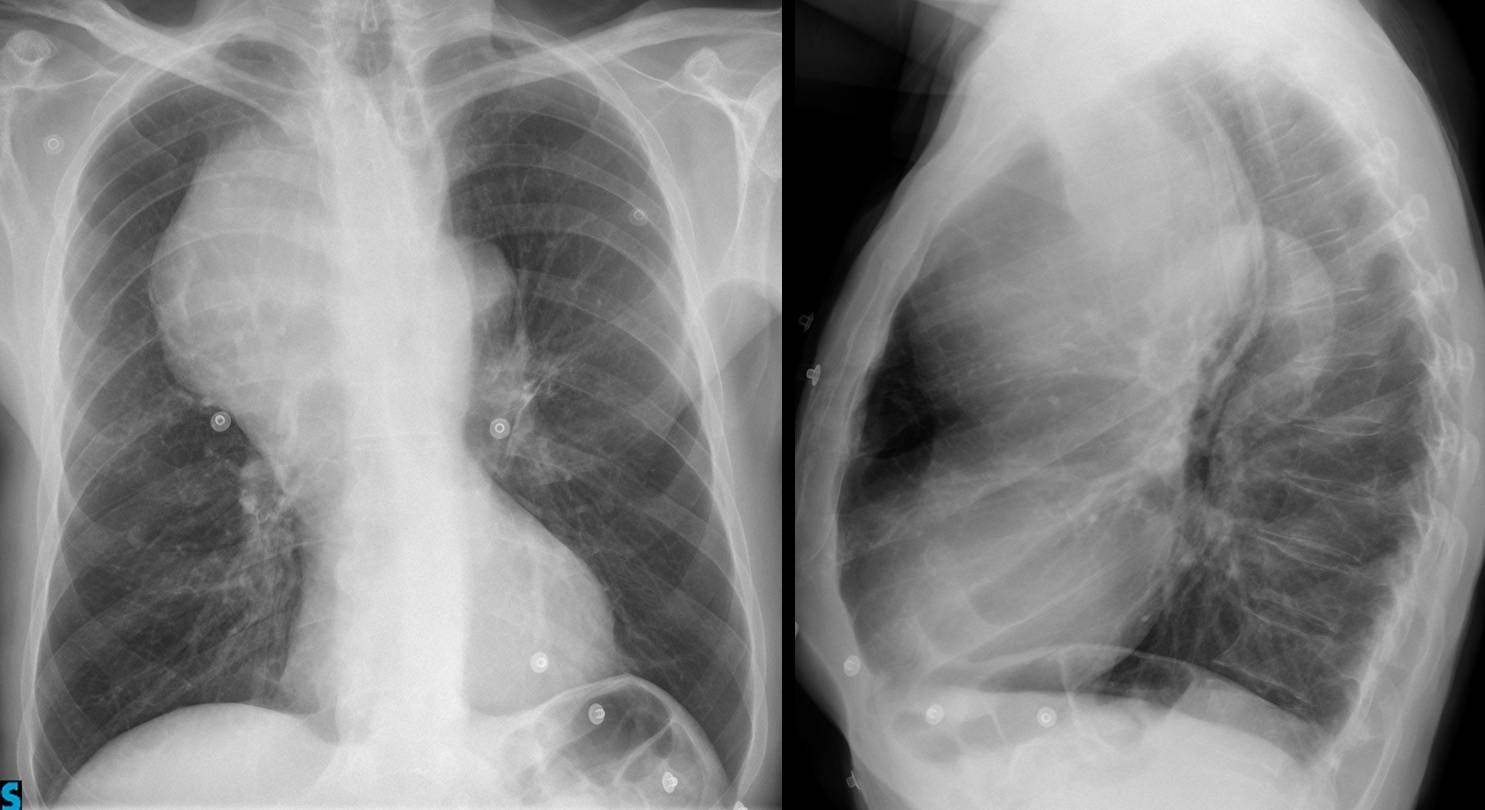
Fig. 1
Findings: chest radiographs show a large anterior mediastinal mass displacing the trachea posteriorly. The mass does not fit the usual pattern of thymoma and it is too anterior and unilateral to think of intrathoracic goiter. Lymphoma could be a good possibility. The etiology of the mass is obvious in the enhanced CT, which shows a large saccular aneurysm of ascending aorta that is not altering the aortic contour.
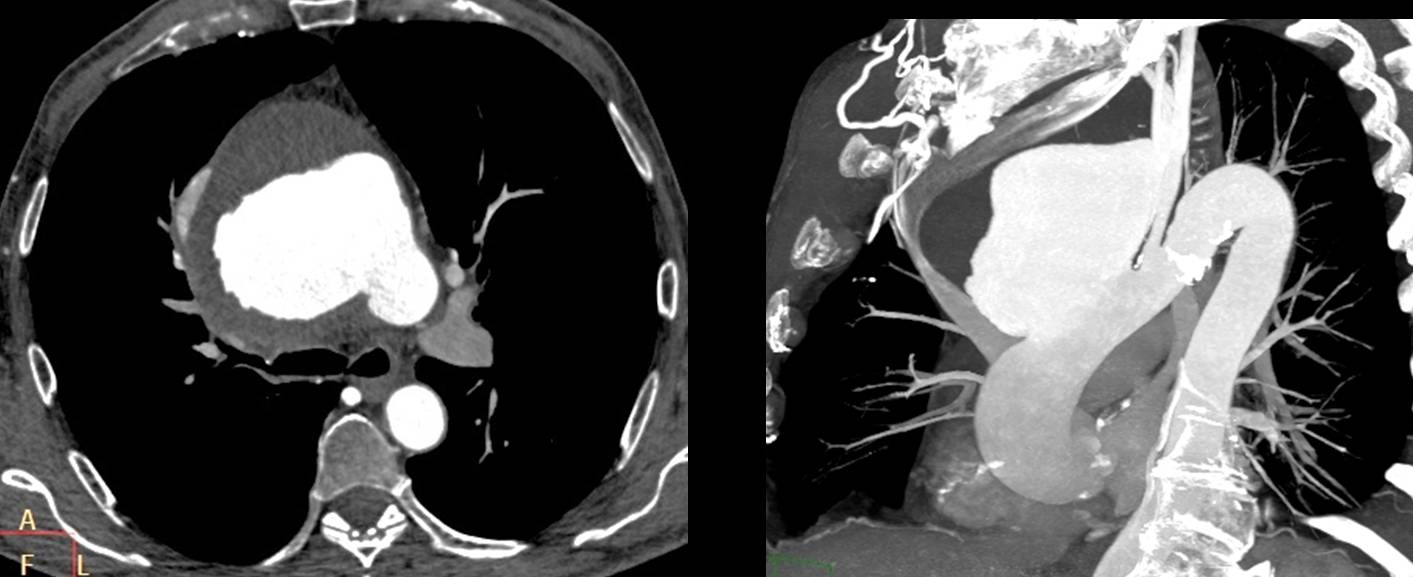
Fig. 2
This case is shown to emphasise that in any mediastinal mass, we should always consider a vascular origin and perform an enhanced CT.
Final diagnosis: large saccular aneurysm of ascending aorta.
Congratulations to Genchi Bari, who was the first to suggest a vascular mass.
Teaching point: always include a vascular lesion in the differential diagnosis of mediastinal masses.


Io penso che la “chiave” di lettura sia la LL del torace:la massa si proietta verso il mediastino anteriore ma penso che nasca posteriormente a livello dell’esofago:infatti vi è una fascia opaca che rappresenta la parete esofagea collabita a causa della ostruzione causata dalla massa che ha caretteristiche di benignità( leiomioma-GIST esofageo?).La trachea è improntata e dislocata mentre in AP sembra ossevarsi un esofago cervicale dilatato.Frattura posteriore della 6 costa dx.
I think is difficult to tell someone were is the origin in a big mass but i believe the mass is located in the anterior -middle mediastinum because we have posteriolateral shift o the ascending aorta and posterior displacement of esophagus and trachea.
it doesn’t look like aneurysm(we dont see aortic wall calcifications….blablabla)
it doesn’t look like goiter we can’t see conection with thyroid
A big esophagial mass like these with out dysphagia? with out obstuction with out dilatation and fluid level?
The mass has smooth well defineted borders predispose a benign mass or lymphoma.
i don t know what is that radiopaque line on the lateral view on trachea.
is tracheal wall thickening? prior study barium in esophagus?
I think is harder if something we can see,but we dont know, to know but we can’t see.
I don´t believe it possible to make the diagnosis of a mediastinal mass without CT. All you can do is make a good differential diagnosis, as you did. I think the location of the mass goes against esophageal origin.
Mitico professore, ho notato dalla risposta a Gus, che hai escluso l’origine esofagea della massa. Allora io penso ad un’altra diagnosi, visto che parliaMO DI MEDIASTINO MEDIO e che la massa sembra fare corpo con l’aorta ascendente , da cui non si nota nessun piano di clivaggio e che inoltra comprime ed impronta la stessa:un ematoma intramurale, visto anche la clinica di dolore toracico?Troppa fantasia?NB: alla ripresa del “campionato 2013-2014 , non vedo gli altri”moschettieri(cioè Maria, Albert,Katarina ed Alice), cosa è successo? Li hai spaventati?Forza Bari! Messi 2 mesi di stop!
Based on the tumor’s location (anterior mediastinum), size, and age of the patient (69 years old), my first thought would be a tumor of thymic origin. Differential would be benign thymoma versus invasive thymoma/thymic carcinoma. CT would be helpful for visualizing fat planes and determining heterogeneity of the mass, presence of calcifications, and associated lymphadenopathy (although, the left hila does look slightly widened to me).
Antrenior mediastinal mass Mostar likely endothoracic goiter
In my experience, endothoracic goiter do not appear in the anterior mediastinum. They may go there, but it is unusual.
A superior mediastinal mass located anteriorly to the right side , thymic tumor is considered ( thymoma, thymolipoma, thymolymphoma, …..) . It is never to be retrosternal goiter extension as there is no FADING sign in the AP view , as well as not aortic aneurysm as it lies anteriorly
Aortic aneurysms may arise from the ascending aorta, which is an anterior structure
Ok, but its extension will be into the middle , superior or posterior compartment so the main bulk of the mass ( aneurysm ) will not in the anterior compartment, but in this case the main bulk of the mass is anteriorly
the trachea is displaced to the left and posterior between the mass and the aortic knob (on the frontal view)
the right hilum is shifting inferior displaced from the mass too.
if we had a ascending aorta aneurysm the trachea should be despaced to the right and back.
the only way these mass to be vascular origin is the right limb aneurysm of a double aortic knob(very rare) and superior vena cava aneurysm or right pulmonary artery aneurysm (very very rare):)
I will think something better tomorrow 🙂
The fact that the mass partially occupy the anterior mediastinum and displaced laterally the trachea , makes me think that the mass is not confined to one mediastinal compartment. I would say that Lymphoma could to it, as well as a big thymic mass( which tend to mold itself to the anterior thoracic wall and go to one side of the chest, in this case to the right,and produce mass effect)
There is a huge mass in the anterior Mediastinum with displacemant of the Aorta and trachea.
Tumor of the anterior Mediastinum are the 4 T´s – Teratome, Thymome, thyroideal tumor or terrible Lymphoma.
Atypically, because of that size, but could also be a aneurysmatic widening of the V.cava superior