Dear Friends,
Muppet and I just returned from the RSNA meeting in Chicago (Muppet very happy after spending the week with Miss Piggy!). This week we’re presenting a straightforward case to make you happy as well. Images belong to a 63-year-old man with vague chest complaints.
Where is the abnormality and what do you think it is? Leave yout thoughts and diagnosis in the comments section and come back on Friday for the answer.

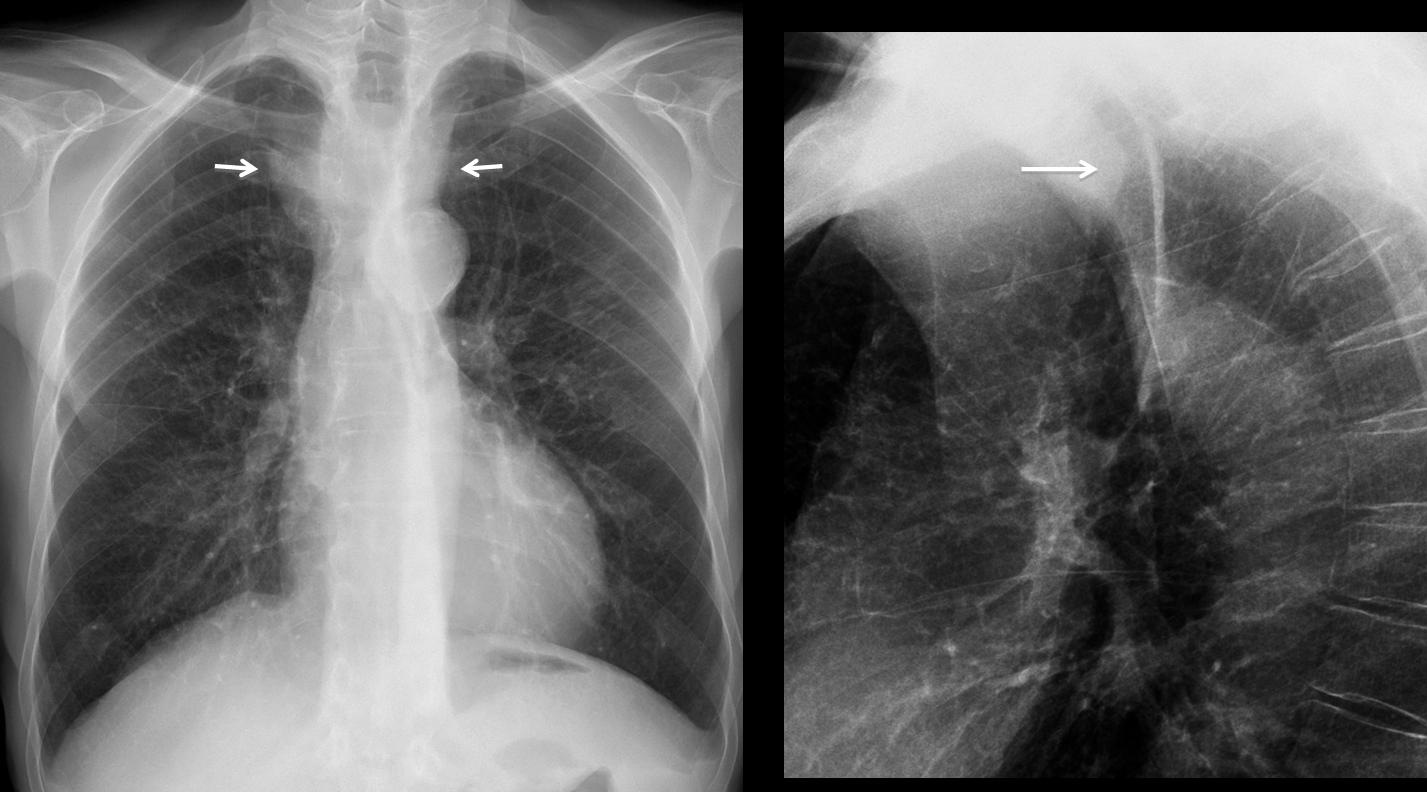
63-year-old man, PA chest
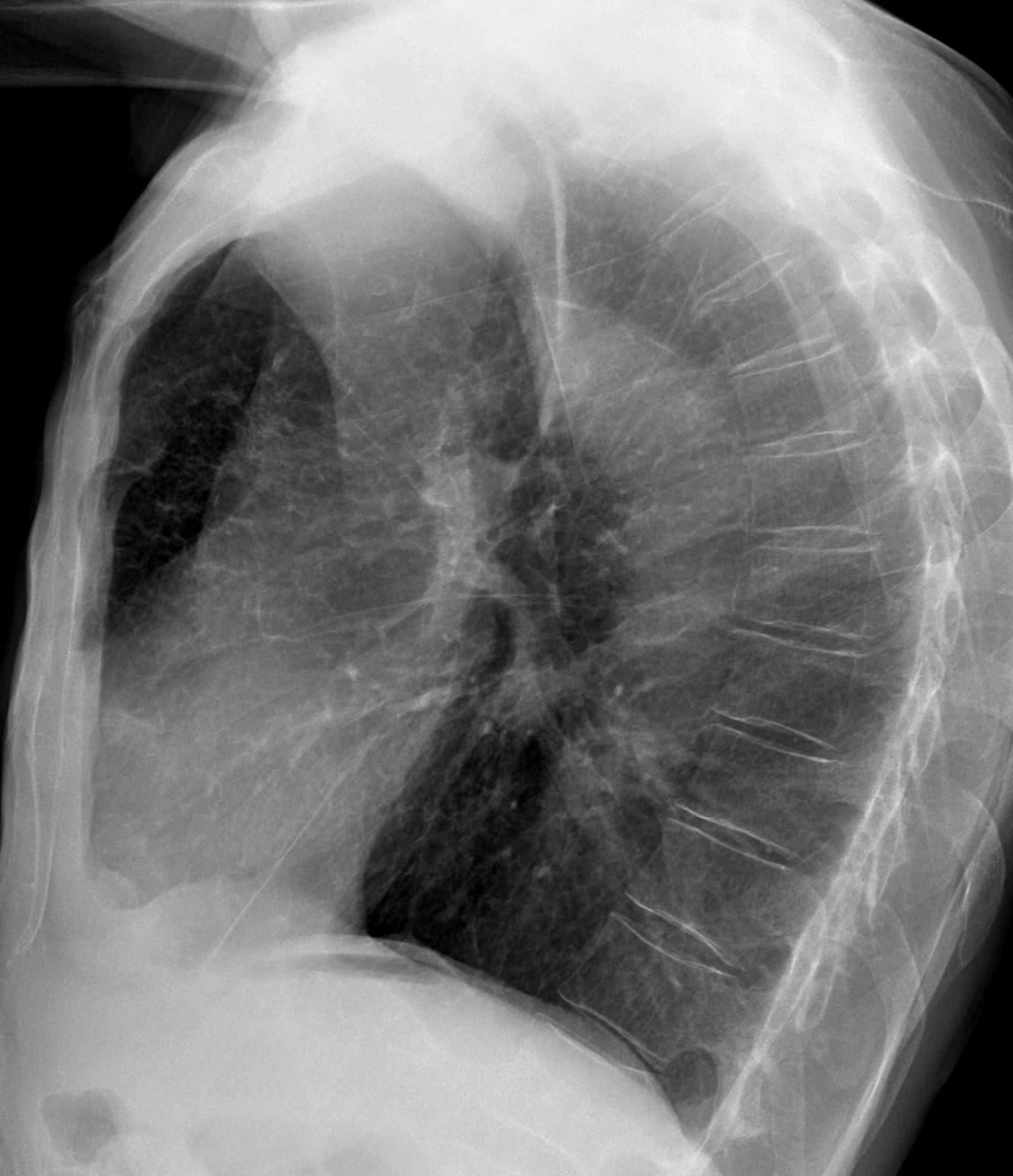
63-year-old man, lateral chest
Click here for the answer to case #81
Findings: PA chest shows an ill-defined increased density in the superior mediastinum (arrows). The lateral view shows narrowing and posterior displacement of the trachea (arrow), indicative of an anterior mediastinal mass.
Because of the tracheal displacement, intrathoracic goiter would be my first choice. A midline cystic lesion should also be considered. Thymoma and teratoma are less likely. As always, a vascular lesion cannot be ruled out.
Coronal and sagittal enhanced CT demonstrate an aneurysm of the innominate artery, displacing the trachea backwards (arrows).
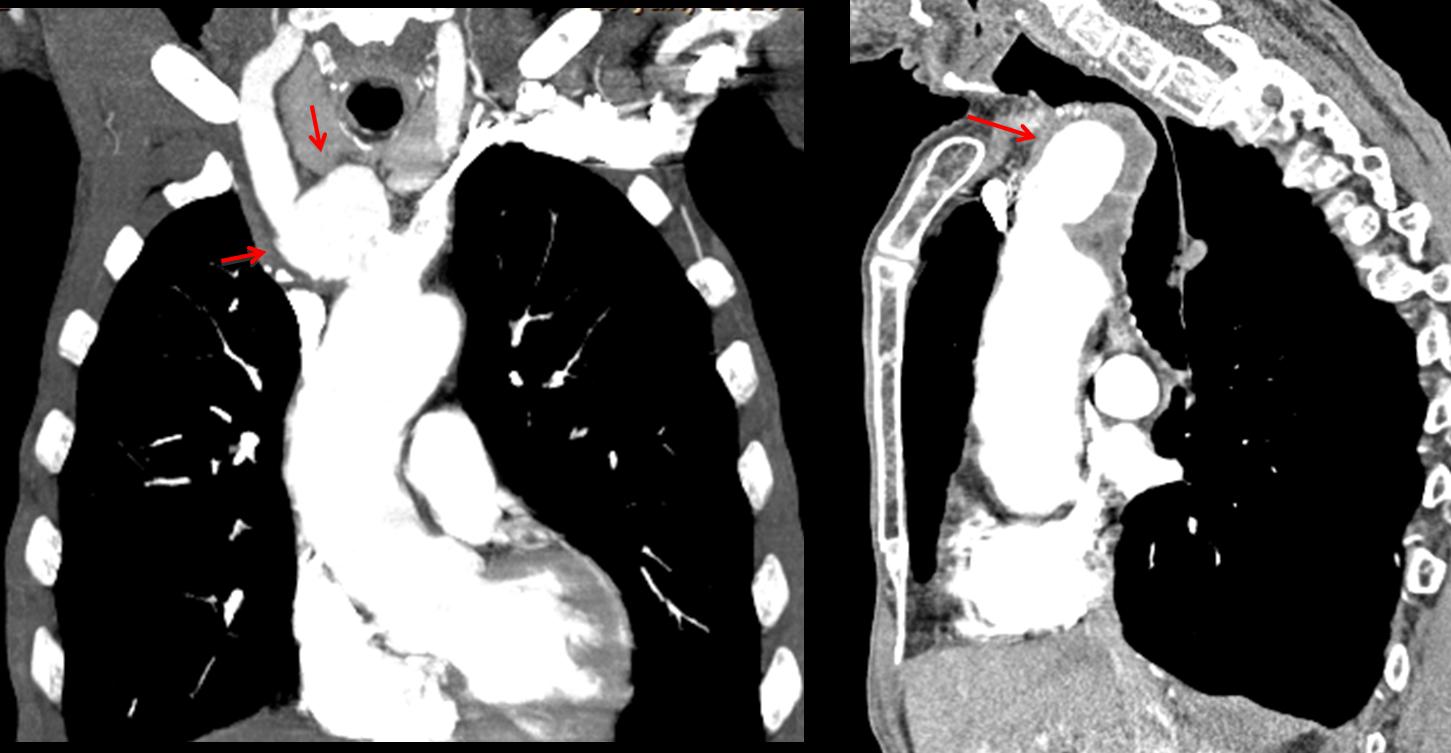
Final diagnosis: arteriosclerotic aneurysm of the innominate artery.
Congratulations to Dr. Sameh Khodair who discovered the tracheal narrowing and Dr. Maria S. who suggested the vascular origin of the mass.
Teaching points (repetition):
1. Remember to look at the trachea on the lateral view.
2. Always consider a vascular origin of any mediastinal mass (see Diploma Casebook case no. 41)


Upper mediastinu- right contour-may be expansion- lymphnodes or thyroid gland for example or lobus venae azygos and some solid structure in trachea.
thickened retrotrachial line! Suspicious!
RUL partial atelectasis maybe!
The retro-tracheal stripe may measure up to 2.5 mm in thickness. I don’t think it is thickened in this case.
A small left pleural effusion; antero-superior mediastinal mass(cervicothoracic sign), broadening of the right paratracheal stripe, unsure about blood flow redistribution, have no idea about the radiodense line coarsing along the left and posterior wall of the trahea, diagnosis, I fail to see the big picture.
There`s widening of the right upper mediastinum in PA radiogram and signs of the segmental RUL athelectasis (ex. S letter sign) in lateral- growing tumor in the RUL bronchus?
In RUL collapse wouldn’t you expect upward displacement of hilum and minor fissure?
Hi Prof, I hope that you enjoyed your time in the RSNA, and I hope that we will spend a nice time in the next ECR also I hope that I meet you, it will honer to me
About the case, I see a well define superior mediastinal opacity having smooth bordered , however its upper borer is faded toward the base of the neck, in the lateral film I see that the mass displace the trachea posteriorly , A retrosternal goiter is considered
also the left costo-pherenic angle is blunted ? pleural thickening Vs minimal effusion
There is widening of the right paratracheal line and increased density projecting on the trachea at Th3 level and caudally.
On the lateral view, there is an indentation on the anterior wall of the trachea. I believe that there’s an aberrant vessel in the upper mediastinum, such as an aberrant left brachiocephalic vein.
Hello Professor,
There is blunting of the left costophrenic recess, which may indicate some pleural effusion. On the left, at the height of the upper third of the hilum transparency is decreased at an area roughly the size of my palm. As for the upper mediastinal shadow on the right with a sharp edge, that fades away above the clavicule, might be an abberant blood vessel.
Impression: left sided pneumonia with effusion, and mass/abberant vessel in the right upper mediastium.
Increased density in the superior mediastinum, obscuring part of the trachea anteriorly and displacing it posteriorly on lateral projection.
Upper vessels are same size as the lower vessels, equal perfusion of lung zones suggestive of decrease ventilation in capillary bed with increase demand on oxygen.
Mural aortic calcifications.
No hilar lymph nodes, left hilum higher than right.
Left retrocardiac paravertebral triangular opacity projecting anterioly on lateral radiograph paralleling the chest wall.
Blunting of the left cost-phrenic angle.
Normal upper abdomen.
Lingula atelectectasis.
Will try to make the long history short:
Isn’t it ostoporosis responsible for pain? There are hyperlucent vertebral bodies, ribs and sternum.
Blunt left costo-phrenic angle may result from minor pleural effusion, but as long as we do not know anything about respratory and cardiac disfunctions I wouldn’t panic.
Opacity near right parasternal line is most probably accessory azygos vein lobe, with fissure clearly visible on lateral CXR.
Increased interstitial pattern and calcifications in aortic wall – without significance.
In my opinion, it is difficult to see osteoporosis in the chest radiograph, specially with digital films. I try to avoid the diagnosis, unless the vertebral bodies are diminished in height.
Strie di Kerley. Opacizzazione seno costofrenico anteriore dx.
there is emphysimatous lungs with left costo-pherenic angle blunted and substernal pleural thickening.
there is widening in the upper mediastinum.
thoracic aorta wall calcifications,
ok, another thinking , that it may be a thymic tumor , I see that it must be more anterior , but in this case I seen emphysematous changes with widening of the retrosternal space, also the previous case with aortic aneurysm learnt me that vascular lesion must be but in consideration
there is two thinks i can t understand, we cant see well the trachea and the pulmonary artery’s.
and second there is radiolucency along aortic arch ,
I believe these two findings are technical.
There is widening in superior mediastinal with opacity like mass lesion occupied anterior aspect of superior mediastinum, that could not be separated well from ascending aorta, These finding suggestive of ascending aortic aneurysm, advise CTA for further evaluation
Well done
Opacity near right parasternal line is accessory azygos vein lobe
Carissimo Professore, in AP vedo una slargamento ,Bilaterale, del profilo mediastinico alto , a livello dell’outlet toracico, nonchè una ridotta trasparenza della colonna d’aria tracheale.La bilateralità dello slargamento ed il fatto che l’ilo polmonare sia in sede mi fa escludere il RUL dx.In LL la colonna d’aria tracheale è spostata verso il dietro e sembrerebbe improntata anteriormente.Tu sai che sono molto fantasioso e vado sempre controcorrente, per cui azzardo per una mediastinite focale fibrosante.
Dear friend, you took a big risk! The diagnosis is simpler than that.
• Soft tissue density with smooth, well marginated outer border at junction of the trachea and right main bronchus
• Absence of the normal triangular shadow of the IVC posteriorly at the base of the heart on the lateral view
And the retrosternal area is clear ruling out retrostenal goitre and lympadenopathy
• Prominence of aortic nipple and blunting of left CP angle
Probable diagnosis is Azygos continuation of the inferior
vena cava
i would like to see the CT if available.
Your diagnosis is well reasoned, but it is not the right one. CT will be shown Friday.
nice case professor….thanx
Why not a goiter? It is usually a middle mediastinal mass.
Isn’t there a nodule on the LUL?
ok i will take the risk 🙂
i feel lucky today.
drop metastasis on thymoma.
This was a wild risk. Wrong diagnosis.
🙁
Are both his humerus elevated in profile image?
I don’t believe so.
In the lateral x-ray dimension of the chest is increased and i think lungs seem lusent. So i think it is emphysema.
We can also say interstitial pathology. Because i can see tiny tiny lines, spreading from hilum to periferally, i dont know to explain it in English:))
The white nodular thing in the mediastinum is aorta of course and patient has hipertansion.
There is a middle mediastinal mass compressing the trachea.
The proposed diagnosis is Bronchogenic cyst considered to be the commonest of foregut duplication cysts.
looks like a normal senile (with all those things like emphysema, osteoporosis, atherosclerosis and LV type of heart suggesting hypertension) chest, having some gastro-esophageal reflux disease or motility disorder (as the esophageal luscency is wide and wall appears thick)
Amazing teaching case , thanks Prof.
Nice one Prof. Cacere , thanks for the teaching!
great case professor.
Nice case!!!! Thanks!!
My diagnosis was the first right one and I wasnt replied. Have you some problem with radiologist from east?
Sorry, I interpreted that you were mentioning the findings in the PA view, when the most demonstrative findings were in the lateral, specially the narrow and displaced trachea.
I don’t know the nationality of the answers. Just the names of the participants. As a matter of fact, I do like people from the east: I have lectured there several times with the ESOR program and found them very participative and well prepared.
Remember that the case presentation is a game, geared to emphasize a few basic concepts.
could you explain please where to look in lateral view? i am ED doctor, i am new one with a X rays.
Greetings and Thanx!!