Dear Friends,
Muppet and I are going to Mexico for a week. When back, we expect all of you to have clinched the diagnosis of this 58-year-old male with chest pain.
Leave your thoughts and diagnosis in the comments section below and come back on Friday for the answer.
Diagnosis:
1. Metastatic disease
2. Pulmonary infarct
3. Mesothelioma
4. None of the above
Click here for the answer to case #84
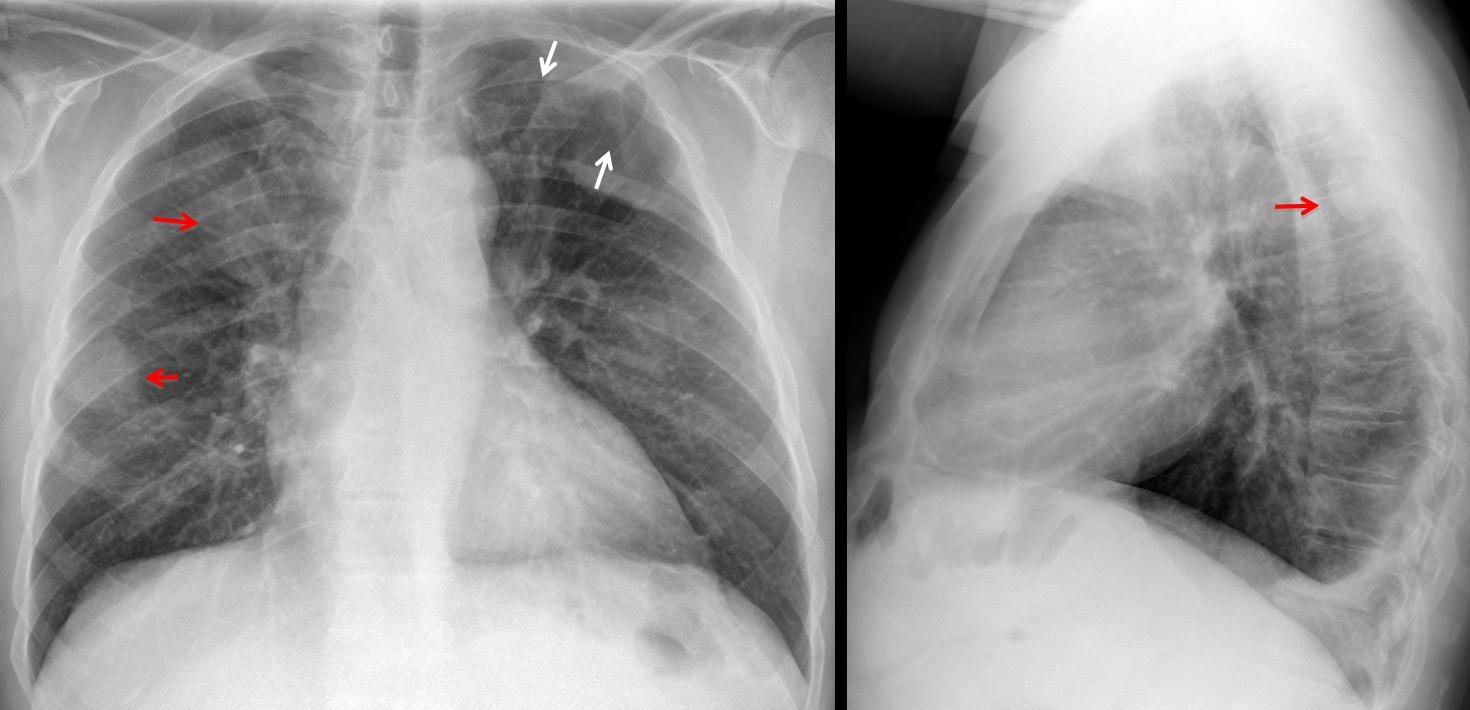
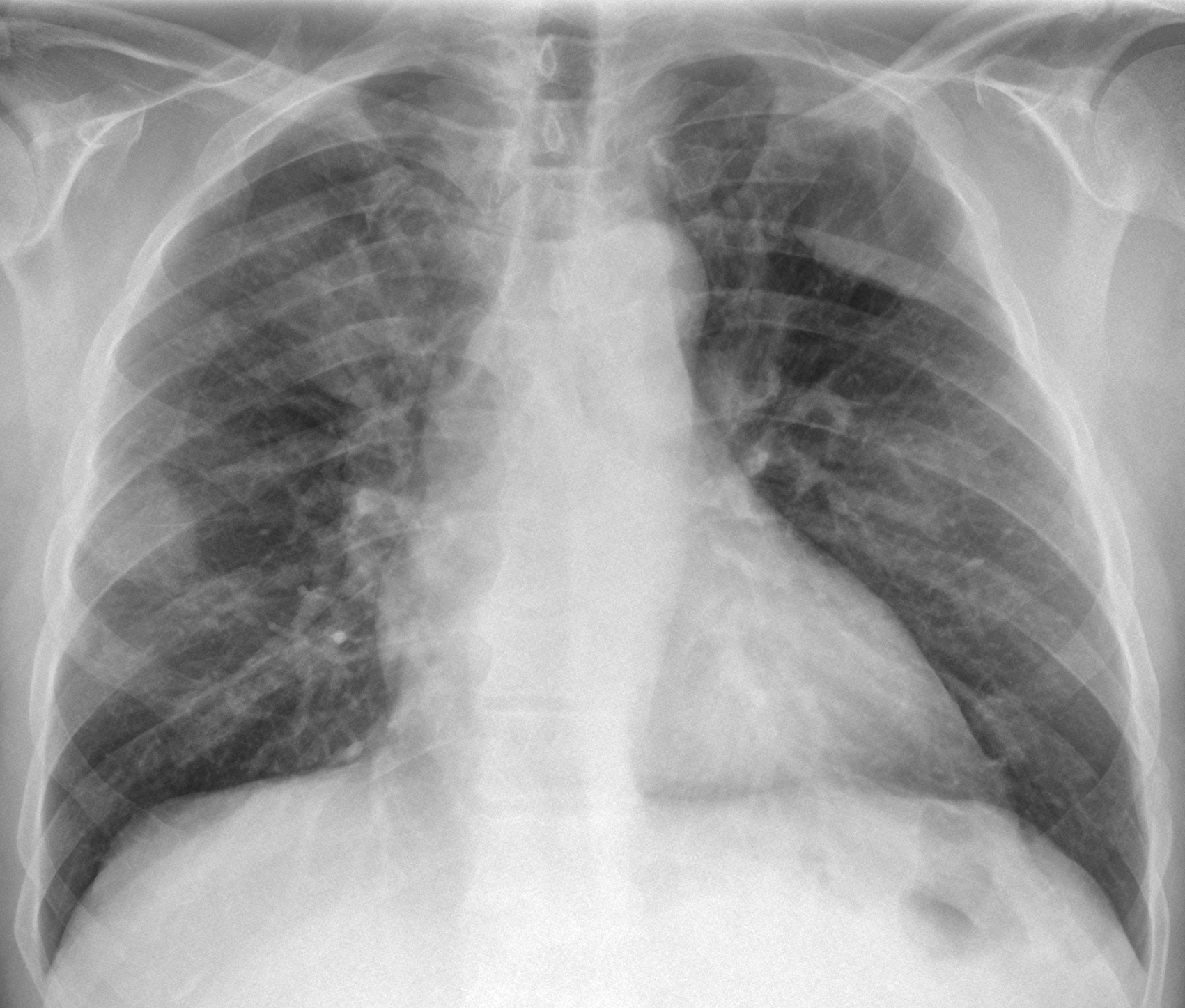
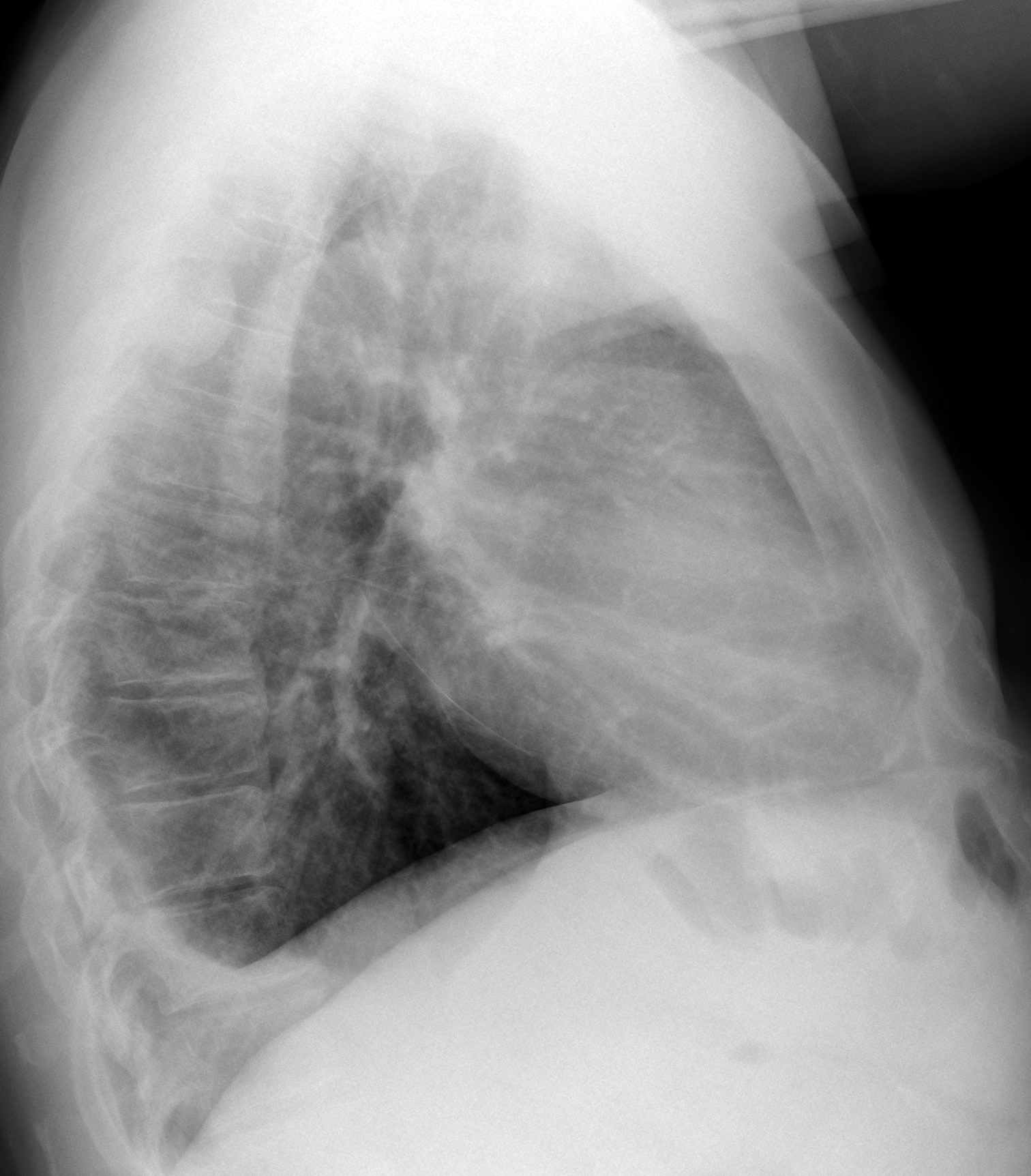
Fig. 1
The main findings are lytic lesions of the posterior arch of the left fourth rib and the proximal left clavicle, with a pathologic fracture (arrows). There are ill-defined opacities in the right lung (red arrows). The lateral view shows a definite extrapulmonary mass (red arrow) and a small pleural effusion. CT shows diffuse skeletal involvement with accompanying soft tissue masses (arrows). The differential diagnosis of this pattern in an adult rests basically between metastatic disease and myeloma.

Fig. 2
Final diagnosis: multiple myeloma. Follow-up chest film after treatment shows regression of the soft tissue masses (Fig. 3).
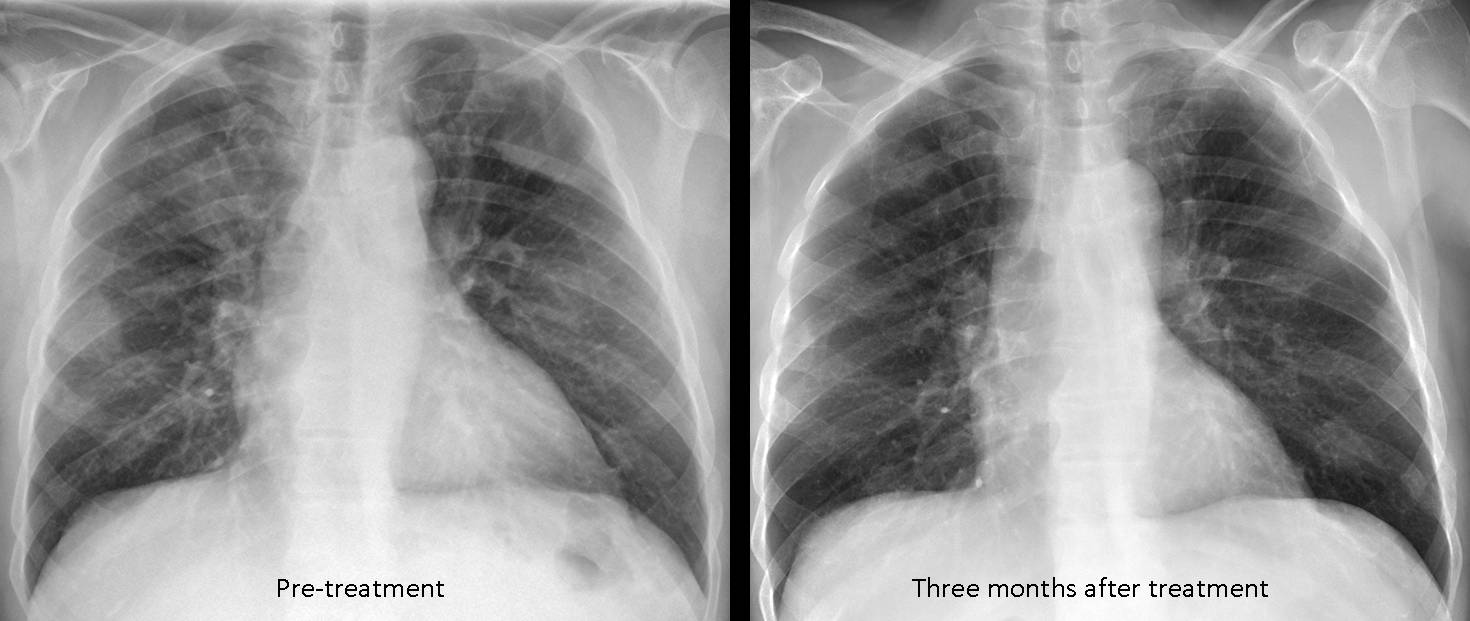
Fig. 3
Congratulations to Genchi Bari, who suggested the correct diagnosis.
Teaching point: remember that haematologic processes (mainly myeloma) should be included in the differential diagnosis of widespread lytic lesions.


Metastasis
I can see some focal translucence in the ribs (posterior part of IV and IX in the left, anterior part of the II and VI in the right) and anterior Th11 body- that suggests osteolytic lesions and matastasis. In the PA and Lateral viev there two round external shadings- masses in the right lung/pleura?
In lateral viev right posterior costo- phrenic angle is shallow- pleural adhesions? Little amount of fluid?
I don`t know what are these lines in the hilum in the lateral viev- artifacts? feregin bodies?
Mesotelioma benigno.
– In right upper field and right midle field ther are round ill define lucencies. They are confirm on the lateral view, where one of them is adjacent to posterior part of the chest wall. Its look more metastatic becouse of sharp adjacent angle.
– Bilateral lungs have signs reticular luciencies, perhaps becouse of fibrotic changes; perhaps he is a long time smoker
– there is a billateral define cephalisation of vesels
– the heart looks mild enlarge more with the left ventricle
– on the lateral view is also seen the shallow posterior costofrenic angle – effusion?
– osteopenia
– degenrative changes of the endplates of vertebral th bodies
– anterion arch of right VIII rib is discontinuous – osteolityc leasion ?
– discontinous shadow of sternal end of left clavicula – lityc leasion?
I ll recomend to read clinical history contact the phisician of this patient and after that dicede to CT scan of thorax and eventualy scintagraphy to localise bone metastais.
answer : Metastatic disease
these osteolytic lesions in the medial border of the right scapula, the left clavicle and left upper ribs appears to be bone resorption rather than destruction ( brown tumor ), I seen also posterior mediastinal smooth well define lesion opacity, so I think about parathyroid cyst associated with hyperparathyroidism
….stimatissimo professore….vi è una frattura patologica scomposta al 3° interno della clavicola sx, nonché riassorbimento, osteolitico, dell’arco posteriore della 4 costa sx; altre alterazioni costali, di tipo addensanti, a carico della 5 di sx e della 5 e 6 costa dx.Vi è poi una opacità , di tipo extra-pleurico, a livello del soma di D5-D6 di dx….ispessimento della pleura posteriore dx con obliterazione del seno vertebro-somatico… non mi piacciomo i somi vertebrali di D7-D8-D9 ……tutto questo deporrebbe per malattia metastatica.
Any alternative?
….quello che sin dall’inizio non mi ha convinto è la “coesisenza” di lesioni litiche e lesioni addensanti ossee costali….quale è il valore della fosfatasi alcalina nel siero e quello della idrossiprolina nelle urine?l’anamnesi è muta?
….mitico…. “l’alternativa” ad una disseminazione metastatica ossea, può essere , per spiegarci l’interessamento “poliostotico”, è quello di una malattia “ematologica” maligna: leucemia, linfoma, mieloma “multiplo”…con cointeressamento della pleura….Grazie Professore!
METASTATIC DISEASE
on the frontal view we can see osteolytic destruction of the 3-5 rib on the left and pathologic fracture of the left clavicle with thoracic wall opacity.
opacity’s also is sub right scapula and above the right hilum.
also we can see a reticulonodular pattern of the lungs.
on the lateral view we can see well the pleural effusion on the right and the two opacity’s(as pleural thickening (plaques?)) one sub sternal and the other posterior paraspinal.
i can’t see hilum lymphy nodes. i can’t see calcifications on the pleural masses or on the diaphragm (asbestos exposure).
there is not shift of the mediastinum (but we have a small pleural effusion)
definatly we need CT!!!
i can’t exclude mesothelioma but my first thought is metastasis.
We, old codgers, used to be good diagnosticians before the CT era.
What do you need the CT for?
good !!!! 🙂 respect 🙂
I think it is going to mesothelioma. I see the coin lesion on the right, the rib destruction of the 4th left rib, and a veil-like opacity over the left apex (pleural plaqing?).
CXR (PA and Lateral):
1. multiple lytic rib and Lt clavicular lesions (destructive).
2. at least a rounded mass in the right missile zone, overlying the inferior Rt scapular angle.
3. Reticulonodular changes bilaterally on the frontal projection.
4. Blunting of the posterior Rt Costo-phrenic angles on the lateral view (pleural effusion).
Impression: metastatic disease.
1. Metastatic disease
None of the above