Dr. Pepe is still in Mexico, drinking tequila and enjoying mexican hospitality. He refuses to come back and asked me to cover for him. Radiographs belong to a 59-year-old male with fever. Had a similar episode two years ago which cleared with antibiotics.
1. Reactivation TB
2. Pneumonia
3. Carcinoma
4. None of the above
Findings: PA chest in 2012 shows an infiltrate that occupies the RUL with elevation of the minor fissure (Fig 1, arrow) indicating moderate collapse. Similar findings were present in 2010. After treatment, the infiltrates did not clear completely.
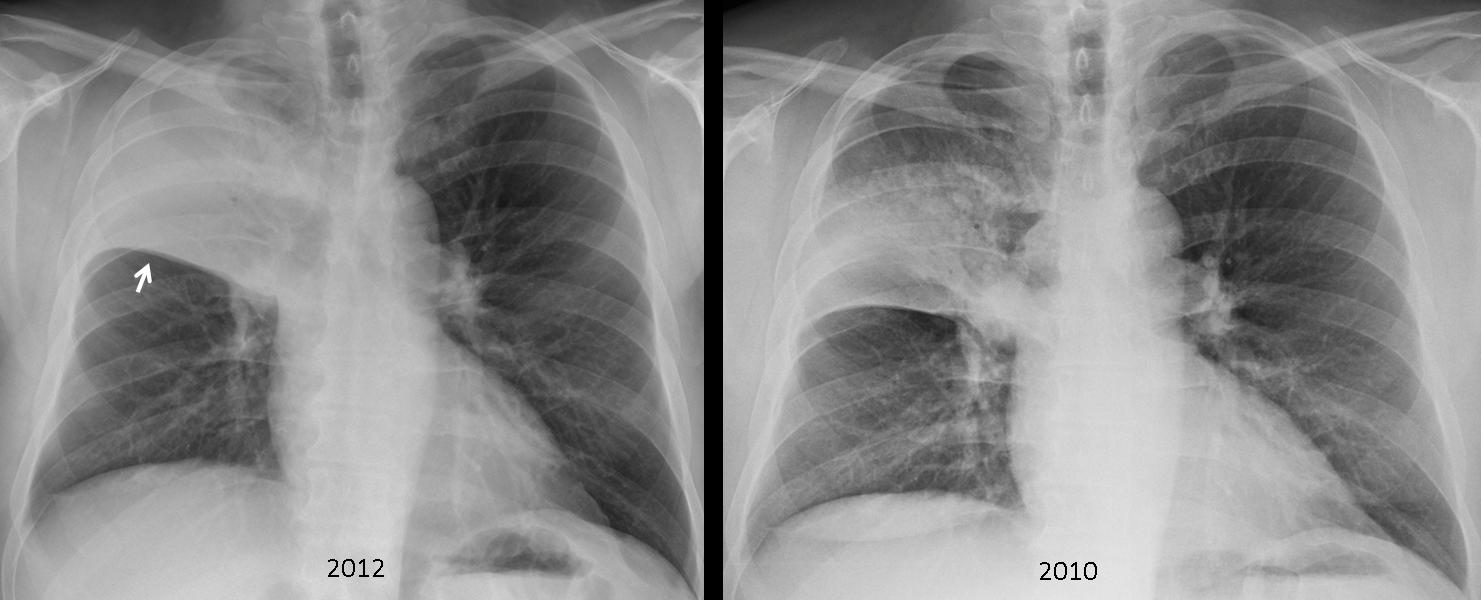
Fig. 1
The clue to the diagnosis lies in two facts: 1. Pneumonias that affect a whole lobe in adults (lobar pneumonias) should arouse suspicion of an endobronchial lesion; 2. Recurrent pneumonias in the same location should raise the possibility of an underlying condition, such as bronchiectasis, a congenital malformation or a lesion in the supplying bronchus. With this in mind, a CT should always be done. In this case, unenhanced CT shows an endobronchial lesion in the origin of the RUL bronchus (Fig 2, arrows). The time span (two years) goes against carcinoma. Surgery confirmed an endobronchial benign tumour.
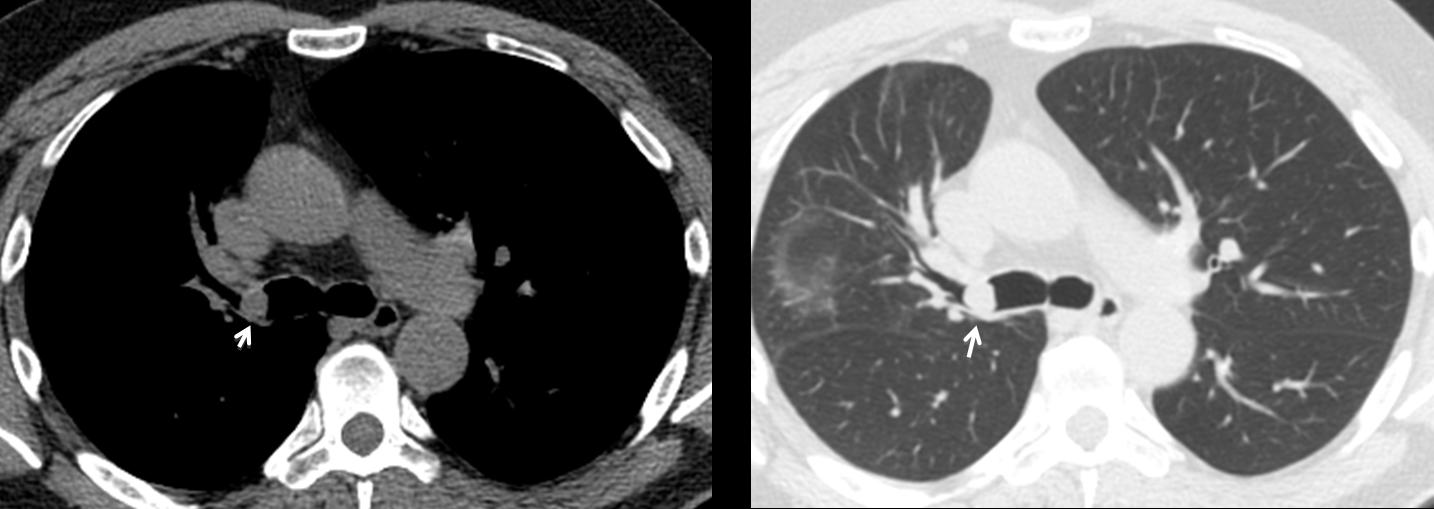
Fig. 2
Final diagnosis: Chondroma of RUL bronchus (possible chondromatous hamartoma)
Congratulations to Genchi Bari who offered an excellent discussion and suggested the diagnosis.
Teaching point: Lobar pneumonias in adults should clear completely after treatment. If not, an endobronchial lesion should be ruled out.



Dear Profesor Caceres,
I hope u are well in Mexico and spending a great time 🙂
In reffering to the case :
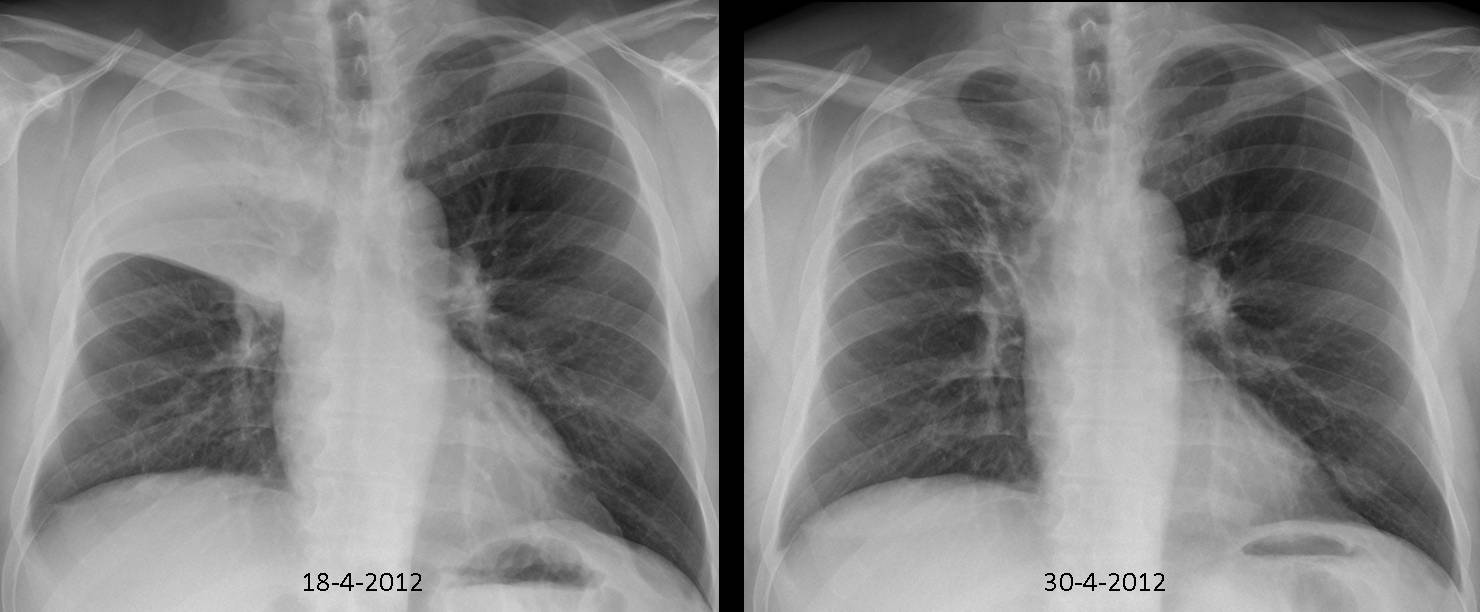
Images 18.4.2012
– Upper lobe of the right lung has homogenus consolidation oppacities with air bronchogram. They are sharply demarcated by bulged horizontal fissure.
– the dragged upwards ( scars,fibrotic changes ) right hilum looks enlarge becouse of enlarge lymph nodes
– the left hilum has no abnormalities
– there is no sign of fluid in pleura
– there is no sign of bone lityc leasions, vertebrea, ribs, and scapula. The only pathology is left curved scoliosis and right sided osteophytes
– there is no air under the left and right diaphragm
I will check the history of the patient – what kind of the antibiotics he was using last time.
I will check the morfology and his socioeconomical status.
Diagnosis : Right lung, upper lobe pneumonia (Streptoccocus,Klebsielle )
Control Image 30.04.2012 ( 12 days )
– the incomplette regresion of pneumonia changes of the right upper lobbe lung.
– now in right lung in the upper lobbe specially peripherally are patchy local oppacification and fibrotic scars dragging uppwards the horizontal fissure. This picture suggest superimposing the old and new fibrotic scars and also not fully cure lobar pneumonia
– In projection of the lower field of left lung there is a round oppacification not seen on the x ray look like shadow artefacts from the ribs.
– the right hilum and horizontal fissure is lifted by the old scars.
– the left hilum has no abnormalities
– there is no sign of fluid in pleura
– there is no sign of bone lityc leasions, vertebrea, ribs, sternum, and scapula. The only pathology is left curved scoliosis and right sided osteophytes
– the is no air under the left and right diaphragm
I will suggest to do a control xray after 7 days cmopare to the morfology.
Diagnosis : Right upper Lobbar Pneumonia
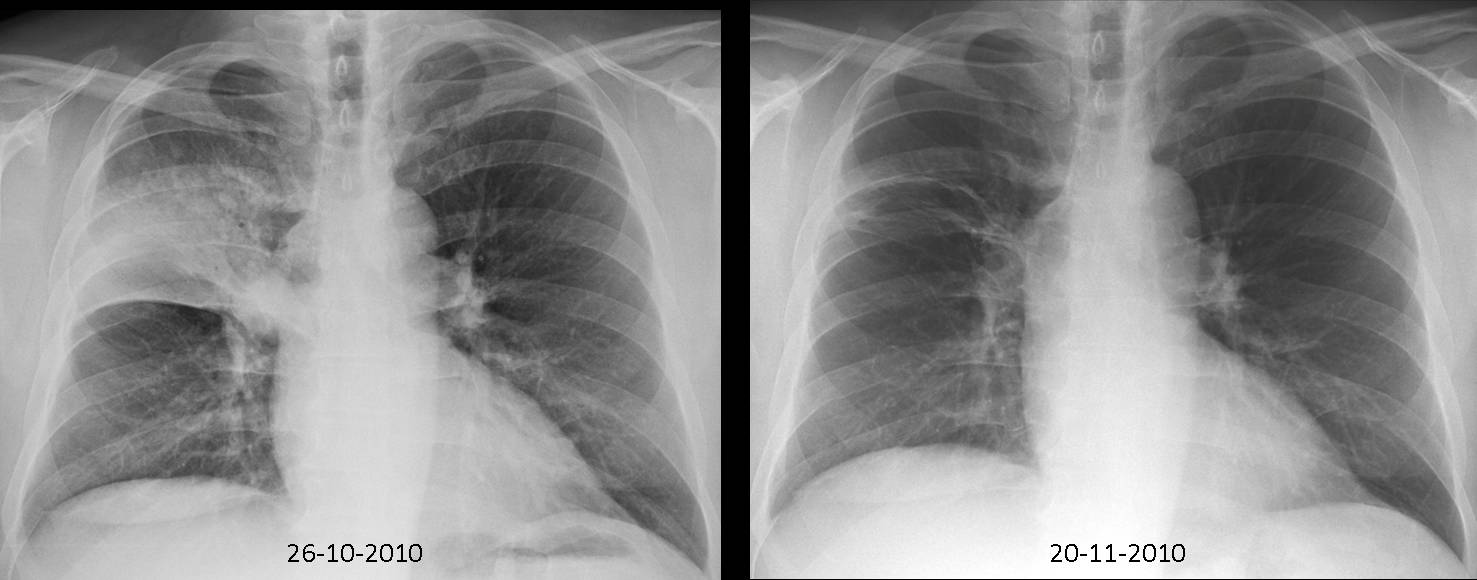
Yo forgot to mention the 2010 films
I was corelatting imagies from 2010 in this sentence “This picture suggest superimposing the old and new fibrotic scars and also not fully cure lobar pneumonia”
Sorry, jet lag.
I think the description of the opacity is complete.
But on the first film 26-10-2010 i see reticulonodular interstitial pattern.(miliary tb?)plus i believe there in lymph nodes of the rihgt hilum.
on the 18-04-2012 film plus there is a small pleural effusion on the right costophrenic angle.
on the 39-04-2012 film i see sclerotic appearance of the first rib on the right.
I think is Post-primary tuberculosis
– In reffere to post primary TBC in the history of the patiennt is written that the patient was cure by antybiotics. The TBC patient use chmioterapeutics and antibiotics. So this is a contra argument for TBC
– The radiology imagies from 2010 and 2012 may suggest that is the post primary TBC with no cavitation leasion which are rather seldom.
but the patient treatment history doesnt
Keep thinking
keep thinking means it is not a right answer:)
do we have any right lateral image.
i would like to focus more on the right hilium. there is well rounded rim with central with low density…
it doesnt look typical.
See Genchi Bari response
it s in foregin language…
but there is google translator:)
dgn: Tracheal bronchus associated with recurrent pneumonia ? Rare case but the problem almost concern uper lobbe of right lung…
Lung carcinoma is highly suspected (especially if patient is smoker), chest CT indicated.
Chest CT was done. You will see on Friday.
The second right rib profile is not defined in the 2012 x-rays…it sounds like a neoplastic flag! So i vote for pneumonia as epiphenomenon of a lung cancer.
What about the time interval? Don’t you think is too long for cancer?
Could it be scar carcinoma?
Very unlikely
How about his CD 4 it’s ok?
It’s a HIV patient?
CD 4 OK. HIV negative
…”galactico”””…il dottor Pepe è in Messico…ma io non ti lascio solo!….Due polmoniti , allo stesso sito(lobo superiore dx)sono sospette per un sottostante difetto di ventilazione bronchiale….inoltre la scissura interlobare è convessa verso l’alto ed il bronco principale dx sembra deviare omolateralmente:questa può essere una polmonite post-ostruttiva, la cui causa, escluso un tumore dopo 2 anni, deve risiedere in una anomalia(bronchiectasica?) del bronco lobare superiore,…d’altronde si nota una opacità densa a livello ilare, nel radiogramma iniziale del 26 10 2010…altra area disomogenea(da “mucoid impact”?) alla base polmonare sx nel radiogramma finale del 30 04 2012…..va bene come “calcio d’inizio”? NB: anche i “blau-grana” qualche volta perdono!!!!
Even the Sun has spots and Barça players are human…
is something like mass on the right hilum when the patient is sick the density is high after tratment the density is low.
That means it is fill up when he is sick.
bronchogenic cyst with infection after bronchial obstruction?
It looks like a mass, but I believe is pneumonia superposed to the hilum. CT did not demonstrated any mass.
Think of simple explanations. Why does the patient have two pneumonias in the same lobe?
Accessory bronchus ?
I believe there is a bronchus wall problem. bronchectasia? bronchomalacia? maybe a mucus producing adenoma with mucus plugs? broncholith?
Good thinking
Mounier-Kuhn syndrome?
bronchus diverticulum. k
…..GRAZIE GALACTICO!!!!!
Penso ad alterazione del bronco lobare superiore, con polmonite segmentaria prima, lobare nella stessa sede successivamente. Fibroscopia risolutiva penso, eventuale TC.
one differential is Asthma… repeated attack of mucous plug and clearing lead to resolving and newer collapse…
From what i see ( as a 1st year resident), i think it’s a recurrent pneumonia in right upper lobe, due to a “corpus alienum” in the lumen of right bronchi ( seen in CT, i it would be nice to see the date when CT was finally made ).
A good a/b treatment resolves the pneumonia, but unfortunately doesn’t resolve the foreign body.
As dif. diagnosis it could be a calcified lymph node, which “ulcered” itself through the bronchi wall, but i don’t see any signs of tbc in the X-rays.