Dr. Pepe refuses to leave Mexico and I have to go there to bring him back. I have asked my friends Jose Vilar and Marisa Domingo to cover for me and present this week’s case. The radiographs below belong to an 18-year-old woman with recurrent haemoptysis.
Leave your thoughts and diagnosis in the comments section and come back for the answer on Friday.
1. Arteriovenous malformation
2. Hypoplasia of left lung
3. Vasculitis
4. None of the above
Figure 1 (PA and lateral radiographs):
a) the left lung has lost volume and there are few small vessels. There are no signs of air trapping or bronchiectasis. The right lung shows increased vascularity and a large vessel (
red arrow), b) in the lateral projection the left pulmonary artery is seen surrounding the left upper lobe bronchus (
blue arrows).
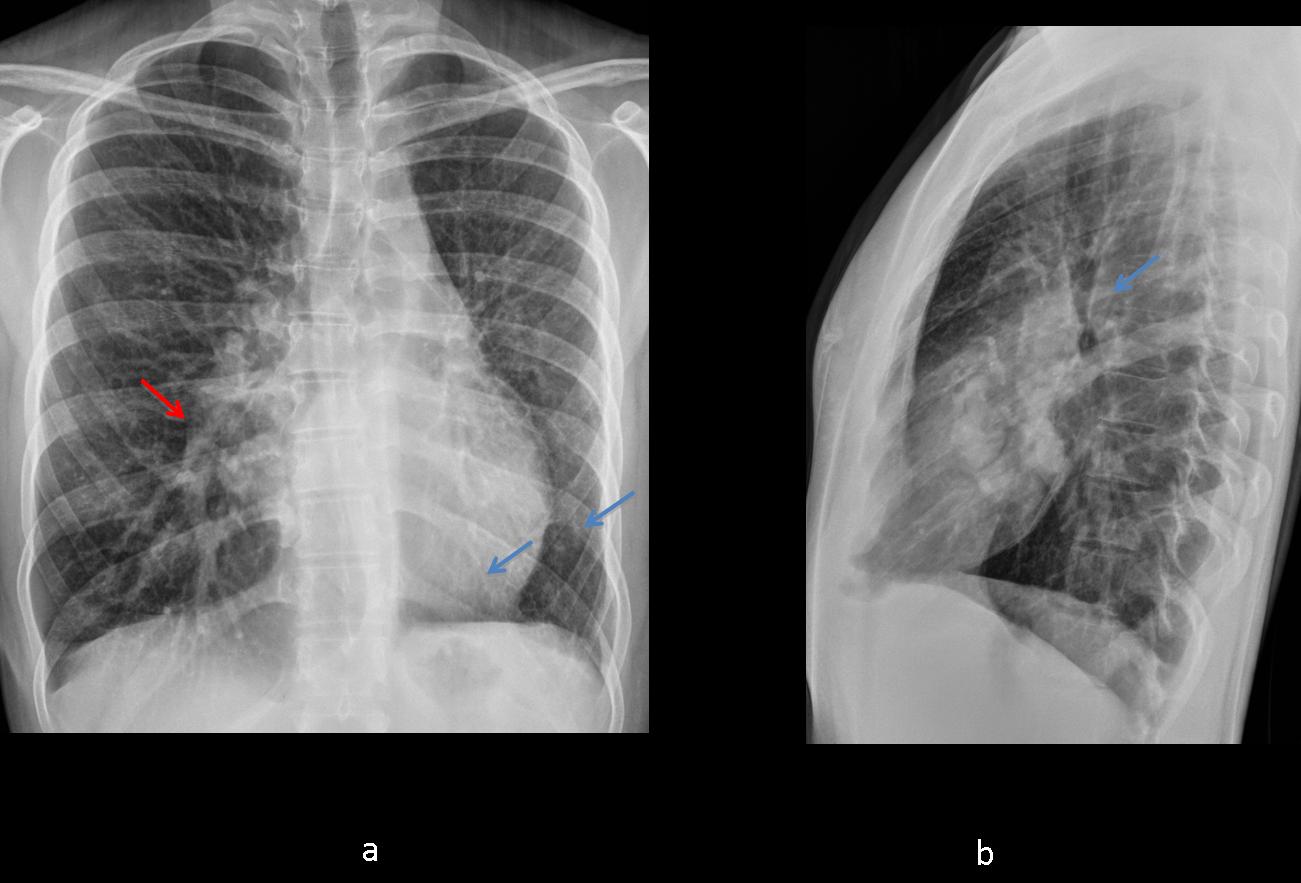
Fig. 1
Figure 2 (CT with contrast):
a) axial image shows a small left lung with thick septa (arrows) and absence of pulmonary veins, b) MIP coronal image shows large vessels in the right lung, small vessels and absence of pulmonary veins in the left.
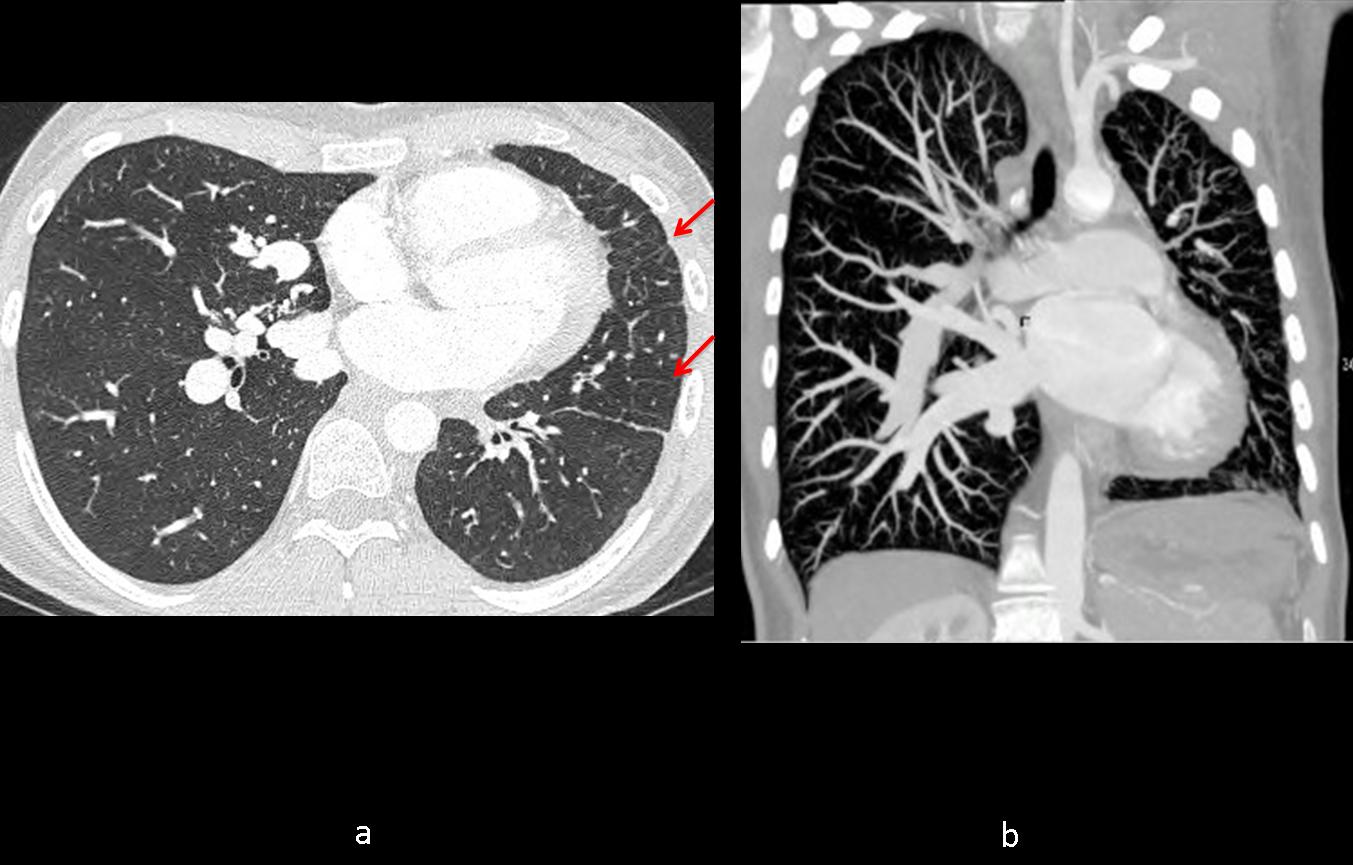
Fig. 2
Figure 3 (CT with contrast, reformated images):
a) coronal 3D image demonstrating absence of pulmonary veins in the left lung and a large unique vein in the right (white arrow), b) MIP coronal image shows tortuous (meandering) vein in the right lung (yellow arrow), absence of pulmonary veins in the left and enlarged bronchial arteries in the mediastinum (red arrows).
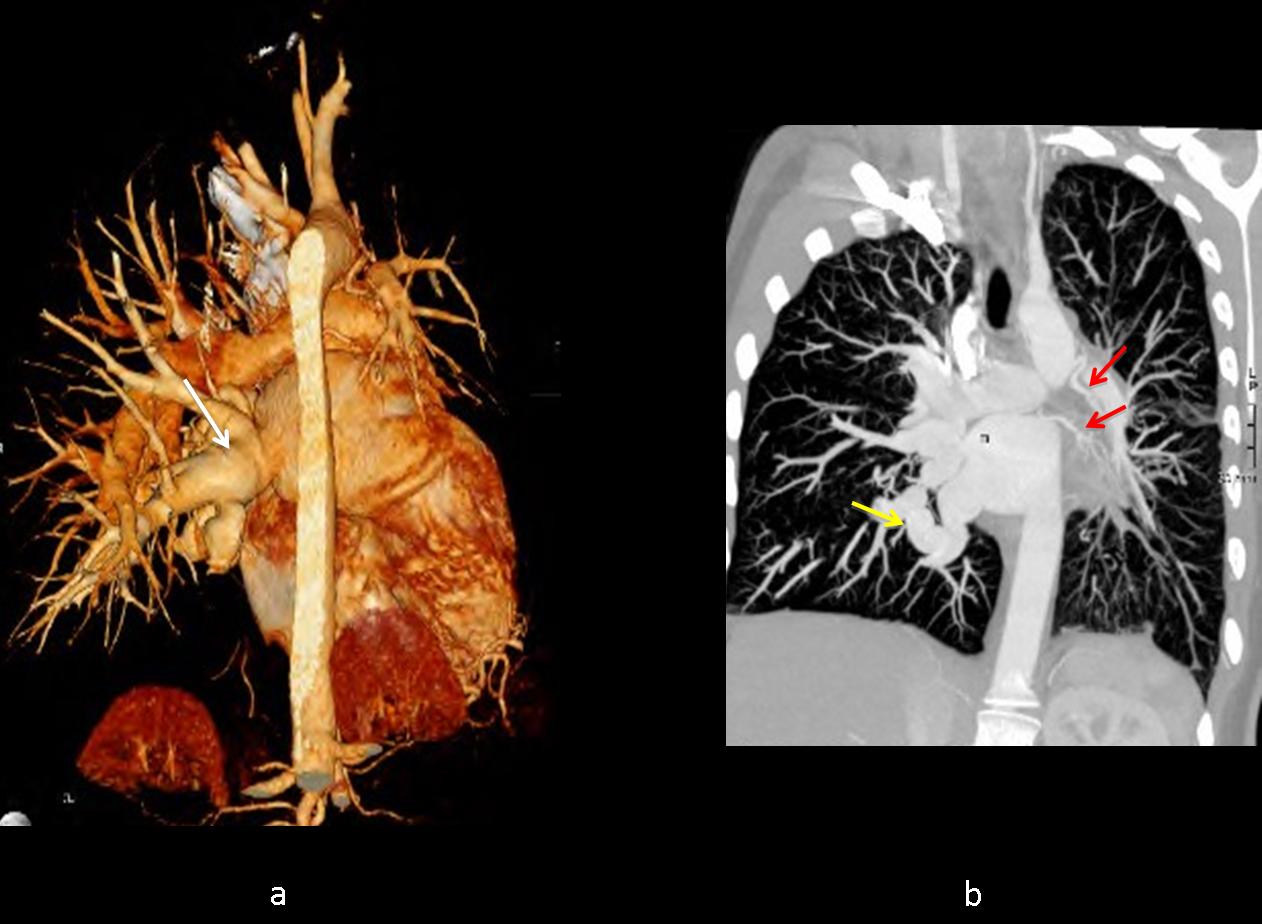
Fig. 3
Final diagnosis: congenital unilateral pulmonary vein atresia in the left lung and
large meandering vein in the right lung.
Teaching point: a small lung with a small pulmonary artery and septal lines is typical of congenital unilateral pulmonary vein atresia.





dear Profesor Caceres,Jose Vilar and Marisa Domingo,
thank you for interesting case.
about x ray……
-bilateral pulmonary fields are normal
-policyclic nodular mases with egg shell like calcification in projection of the right hilium
-the left hilium is not well seen and its hard to examine
-the trachea is shiftet slightly to the left-i’ll sugest becouse of enlarge nodular masses
-there is an abnormal shadow of left main bronchus-shadow superimpose?
-the heart is slightly shifted to the left- pectus excavatus
– there is no pneumomediastinum,pneumoperitoneum or pleura effusion.
My suggestion is sarcoidosis in early stage I and pectus excavatus becouse:
– female gender of the patient – predylection
– age
– 1,2,3 sign – right paratracheal, right hilar and left hilar nodes enlargment
– egg shell calcifications
– hemoptysis
– heart shadow shift to the left – becouse of chest deformity.
what about swayer james syndrom…
is usually shows a unilateral lucency of the lung with no hilar nodule enlargment
what about avm….
avm usually are more peripherally, unilateral but they can be anywhere. The egg shell calcifications doesnt fit to me with avm..
vasculitis like Behcet ? bu what about calcification…
Arteriovenous Malformation.
I can see hyperinflation of the right lung, as well as abnormal blood vessels next to the hilum and at the hilum itself.
The left lung could be hypogenetic but ribs and diafragm are normal.
So we have the combination of a probable arteriovenous malformation, like Rendu-Osler pulmonary varices, etc., and the hyperinflation.
Unfortunately, my knowlegdge is not enough to match this two findings into an only diagnosis, sorry.
Sweyer James syndrome.
I see dilatation of left bronchus and narrowing of the distal part of the trachea (on lateral). I can think of inflamatory disease- Wegener`s granulomatosis?
uplift of horizontal fissure
intussusception posteriorly of RLL to the contralateral hemithorax.
shifting of the trachea and heart to the left.
that mean’s we have lost of volume to the left
we can see clearly the right hilum on the latera view but not the left.
i see something (on the same density) anterior
of the right hilum like second hilum.
i think is a kind of congenital anomaly of the left lung and the left pulmonary artery.
intussusception posteriorly of the right upper lobe to the contralateral hemithorax . sorry
Interruption of the left pulmonary artery?
hey Gus,
do u thing it is unilateral absence of the pulmonary artery? but what about the calcification on the right side in hilium projection?
could be unilateral absence of the pulmonary artery. i think we see collateral vessels.
OK. You are right: the left lung is small. Do you see the left pulmonary artery in the lateral?
….no in location that expected to see normaly.
may be is not exist. i think we see dilatations of collateral vessels in lateral view.
….Mitico professore….hai cercato “rinforzi” per battere il “piccolo” Bari?…Il polmone dx è iperespanso ma non dimostra cause da intrappolamento aereo….il polmone sx è piccolo con l’omra cardiomediastinica e la trachea scivolati a sx( ma non ci sono fenomeni atelettasici)…è solo meno sviluppato….il circolo polmonare è congesto e non si vede l’arteria polmonare sx, ma solo grossolane immagini vascolari come da circolo di compenso ….infine mi sembra(!) di vedere delle irregolarità sul bordo inferiore della 8 e 9 costa di sx…..infine la clinica e la giovane età….tutto depone per una probabile agenesia dell’arteria polmonare sx, con circolo di compenso, congestione del piccolo circolo ed emottisi!!!!Onore al Barcellona….rispetto per il mio BARI!
Some of you are getting close. A small left lung with small vessels and hemoptysis without bronchiectasis…Keep thinking.
There is definitely left pulmonary artery agenesia or hypoplasia. I dare to say that maybe there is agenesia of the entirely left lung because I see ectopia of the inter lobar fissures.
Think of other other cause of decreased perfusion and a small lung aside from agenesia or hypoplasia of the pulmonary artery.
….in anamesi, in epoca neonatale, sono riferite manovre di cateterismo della vena ombelicale….e possibile complicanza trombo-embolica dell’arteria polmonare sx?
1 The etiology of unilateral decreased lung perfusion can be divided into an isolated congenital branch PA stenosis and branch pulmonary artery (PA) stenosis seen in many CHD patients, such as TOF with right or left PA stenosis, transposition of the great arteries (s/p arterial switch operation) and truncus arteriosus…
2 Mediastinal fibrosis, Aortic dissection, Pulmonary embolism
Centrally obstructing mass,one of them? 🙂
Think that the less flow the smaller the arteries.
WOW:-)