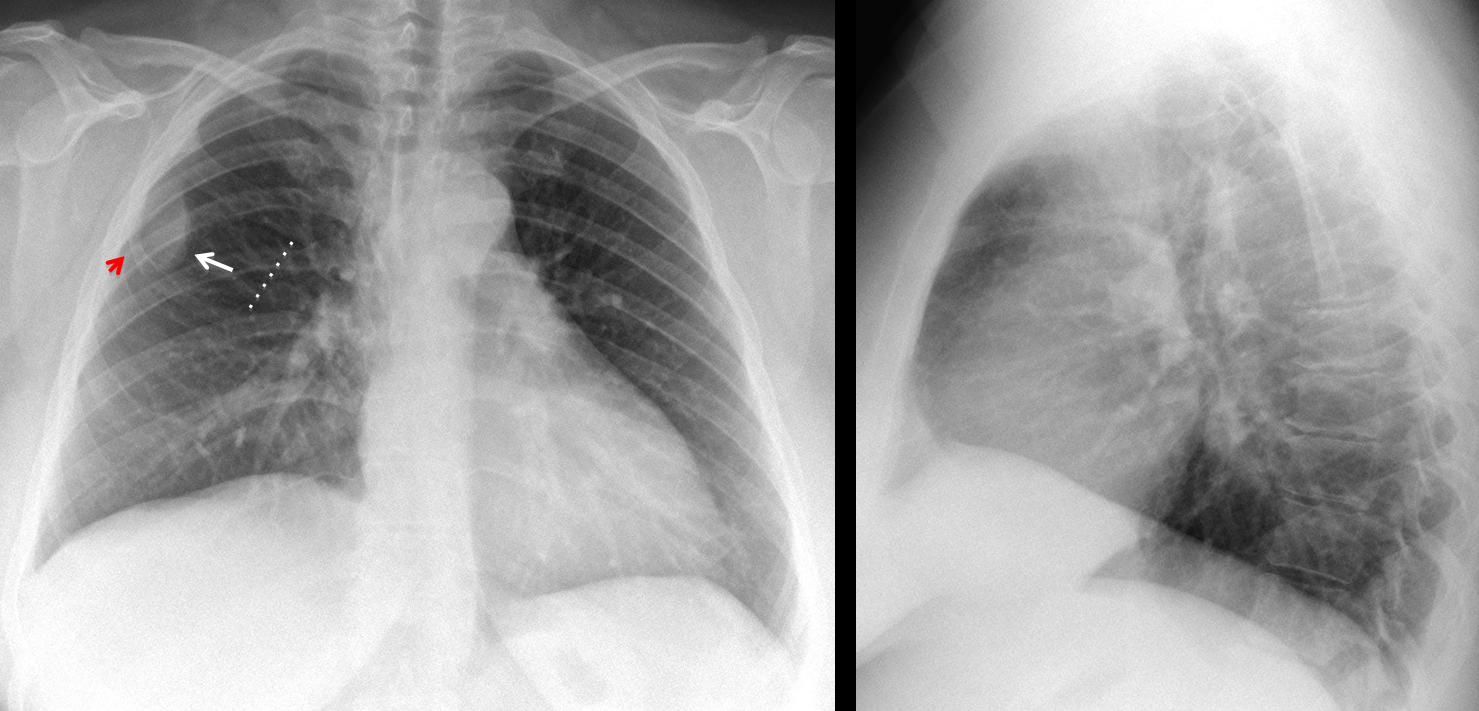
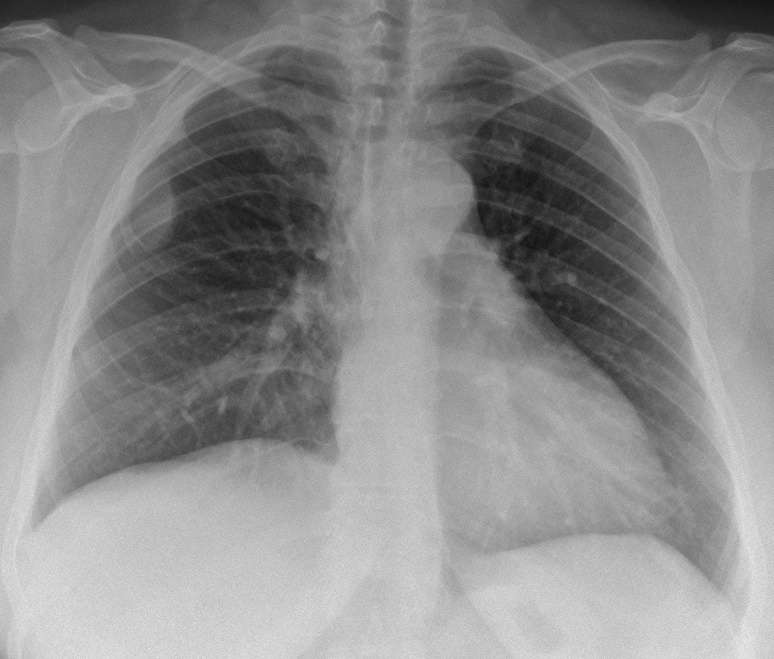
Muppet is concerned about the few responses in the last case. He wants to show an easy case to stimulate participation. Showing pre-op radiographs of a 41-year-old woman with rectal prolapse. The opacity in the right lung was not seen in the CT. What do you think?
Examine the images below, leave me your thoughts and diagnosis in the comments section, and come back on Friday for the answer.
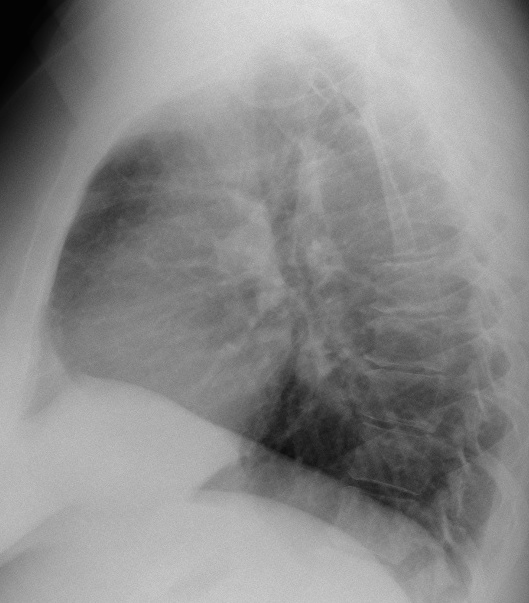
Findings: PA chest shows a right extrapulmonary opacity, accompanied by thinning of anterior right rib (red arrow). The intercostal space is widened (broken line). The lateral view is unremarkable.
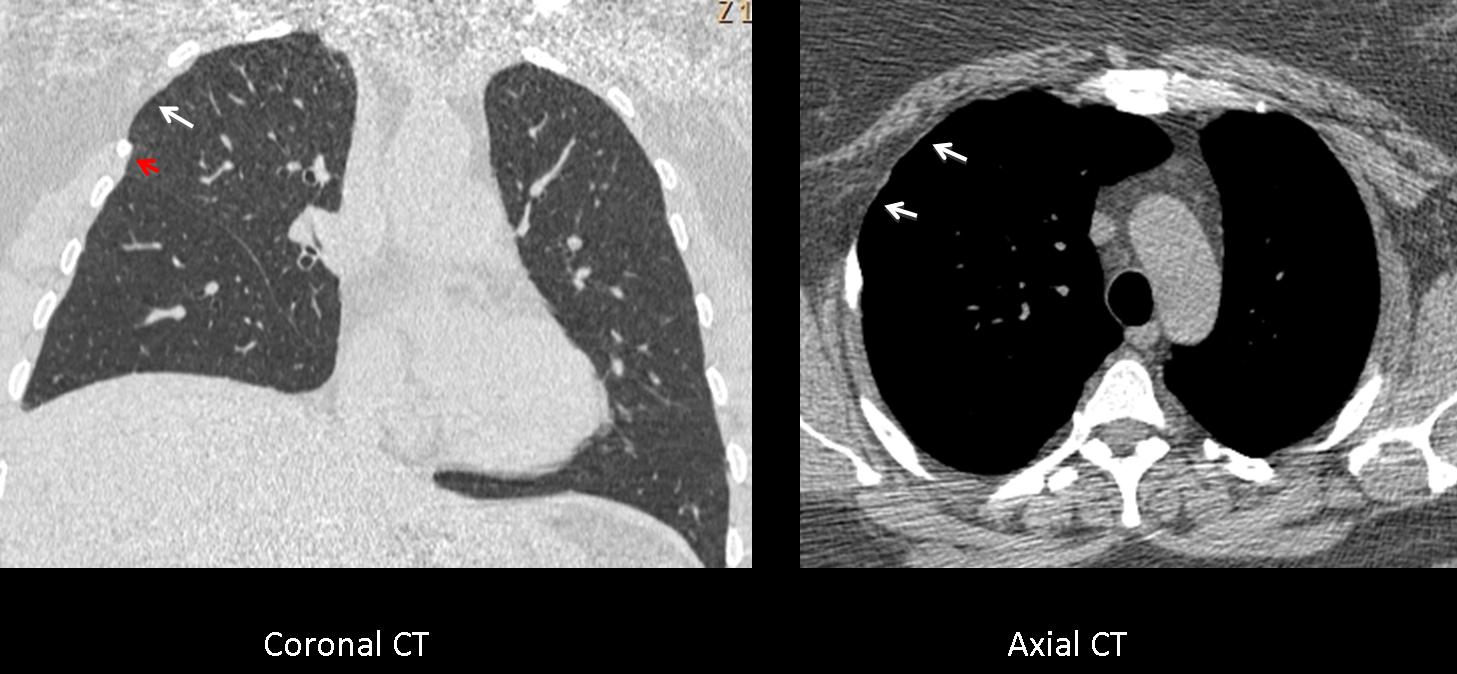
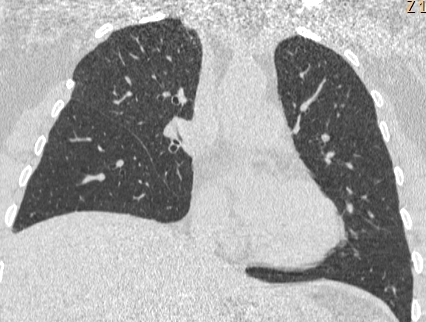
Coronal CT confirms the slender rib (red arrow) as well as the widened intercostal space (arrow) and atrophy of the intercostal muscles, confirmed with the axial CT (arrows).
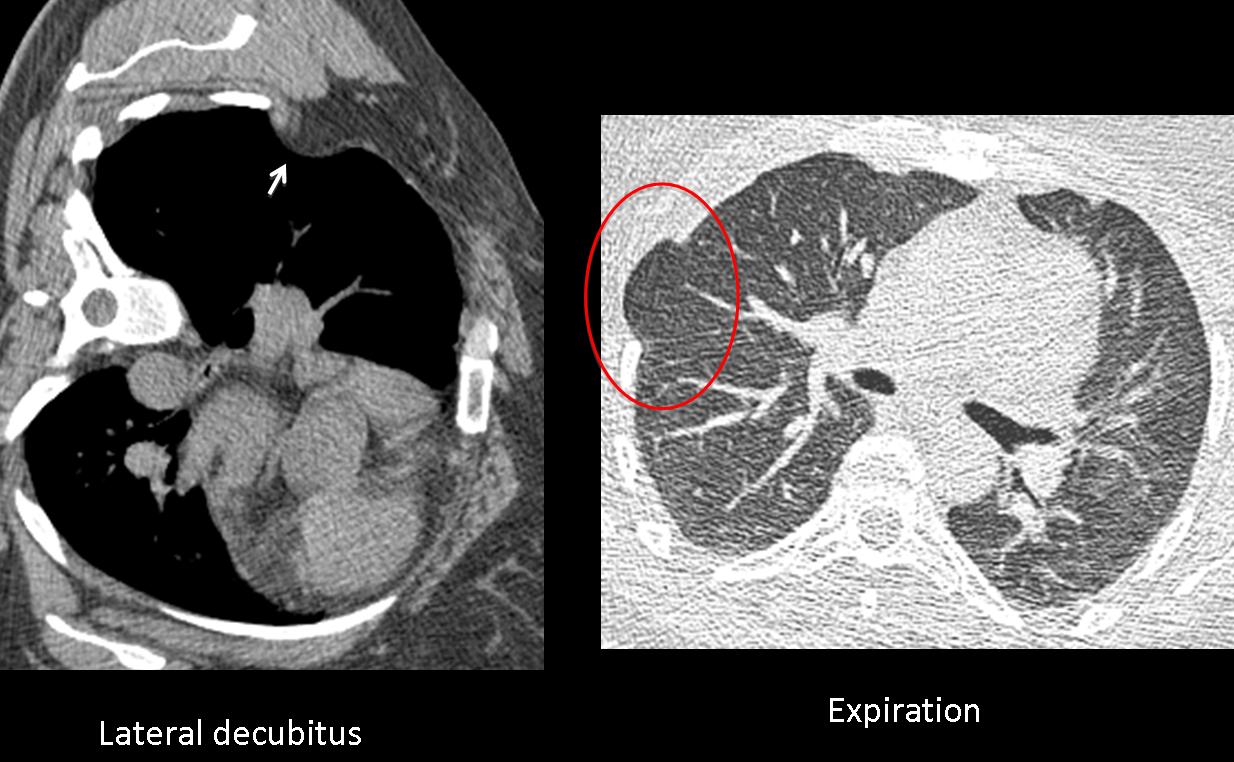
The striking finding is that the extrapulmonary opacity is not visible. Given the atrophic intercostal muscles, a good explanation is that the chest wall fat is herniating into the chest cavity. This theory was proved by placing the patient in the left decubitus position, which confirmed the fat herniation (arrow). An expiratory CT showed lung herniation in the same weak spot (red circle).
Interrogation of the patient discovered that she had surgery in childhood for complications of a pneumothorax.
Final diagnosis: herniation of chest wall fat into the thoracic cavity.
I want to congratulate Genchi Bari, Murzin and specially Gus, who made the definitive diagnosis
Teaching point: sometimes it is good to use our imagination to confirm suspected diagnosis. A little creativity can carry us a long way!


….la lesione è , per ragioni di semeiotica radiografica, extra-polmonare ed extra-plerica….orginadal margine superiore della 3 costa( assottigliata), ha margini regolari non aggressivi ed opacità omgenea….essa allarga lo spazio tra 2 e 3 costa e si dimostra convessa verso l’esterno…..potrebbe trattarsi di una complicanza di una costotomia.Data la sede superficiale, io avrei fatto per prima cosa una ecografia , per stabilirne la natura solida o liquida….. NB: bene il Barca contro il Real e Messi 3 goals….il Bari è fallito ma si salva in serie B.
Can you explain why the lesion is visible in the radiograph and not in the CT?
….cosmico Professore, hai fatto una domanda ma non mi hai risposto perchè hai fatto una TAC e non una semplice ecografia, come esame iniziale…se la massa fosse “vera”, gli US avrebbero già chiarito le cose, penso…c’è un nesso con la relaxatio diaframmatica? il torace è fatto in ortostasi….la TAC supina….
TAC was ordered by her doctor. How would you prove the “relaxatio diaframmatica?
….Galactico…”pitfaill”diagnostico?…Nella mia prima diagnosi ho parlato di esiti di costotomia della 3 costa, che tu hai confermato,”aggiungendo” resezione parziale dei muscoli….ora nella “stessa” sede si trova una formazione rx-opaca , “vista” con l’Rx e”scomparsa” in TAC(!)…l’esito chirurgico muscolo-cutaneo deve aver lasciato un “vuoto cicatriziale” con fibrosi, il che spiegherebbe l’opacità all’rx( da fibrosi) con mancata visualizzazione alla TAC….và meglio come diagnosi?….
An extra joint is seen in the anterior part of the right first rib at the point where the bone meets the calcified cartilageneous part.This may simulate a lung mass on PA-CXR but the lung is normal in chest CT.
I say the same thinks with my colleagues. But i think the mass is visible in CT indirectly as a more translucent area in the mass borders with mass effect in thoracic wall.
i think these mass is chronic (benign)that’s why the hypoplastic rib.
Do you really believe that the mass is translucent on CT and opaque on the chest X-ray?
I am wrong
Rib hypoplasia probably caused a wider intercostal space that is filled with chest wall soft tissue fold. No volume averaging on ct so no visibility of lesion.
The other thing about ct: is there a intercostal (2-3) muslce absence?
Perhaps it is a mild form of Poland Syndrome?
The absence of muscle and rib hypoplasia are due to chest surgery in childhood.
How would you prove your theory?
Intercostal uncomplicated hernia on inspiration and expiretion?
Good! You are a hero!
How would you prove your theory to the Chief of Surgery?
valsava 🙂
sorry valsalva
OK, you are familiar with the classics. Wait for the images on Friday.
1- 3th right ribbon rib
2-extrathoracic tumor soft tissue not seen well
3-bronchiectasis
Diag: NFibromatosis
Intercostal lung hernia