Caceres’s Corner Case 65 (Update: Solution)
Dear friends,
This is a recent case of a 55-year-old man who came to the Emergency Room with epigastric pain. PA and lateral chest were obtained.
Diagnosis:
1. Duplication cyst
2. Lymphoma
3. Neurogenic tumor
4. None of the above

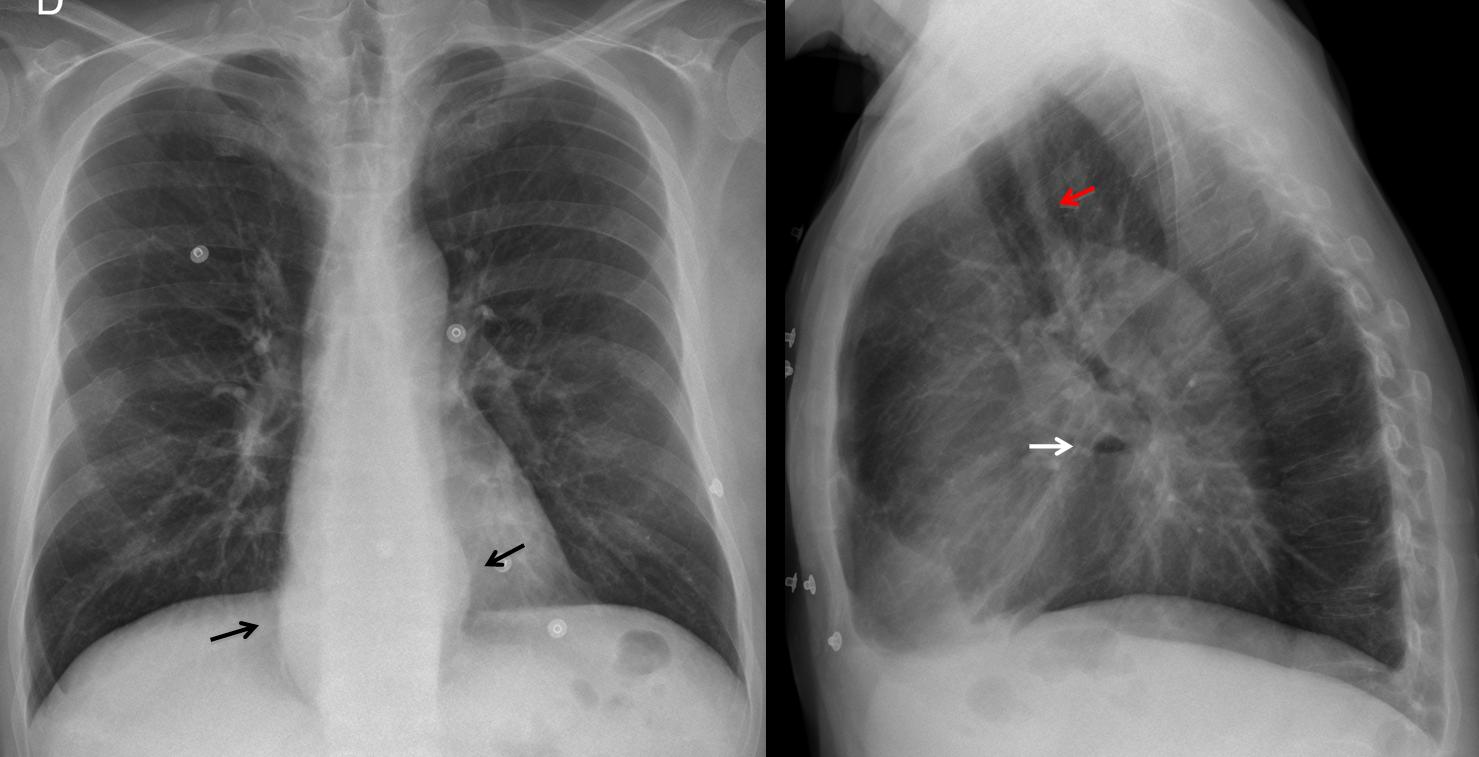
55-year-old man, lateral chest
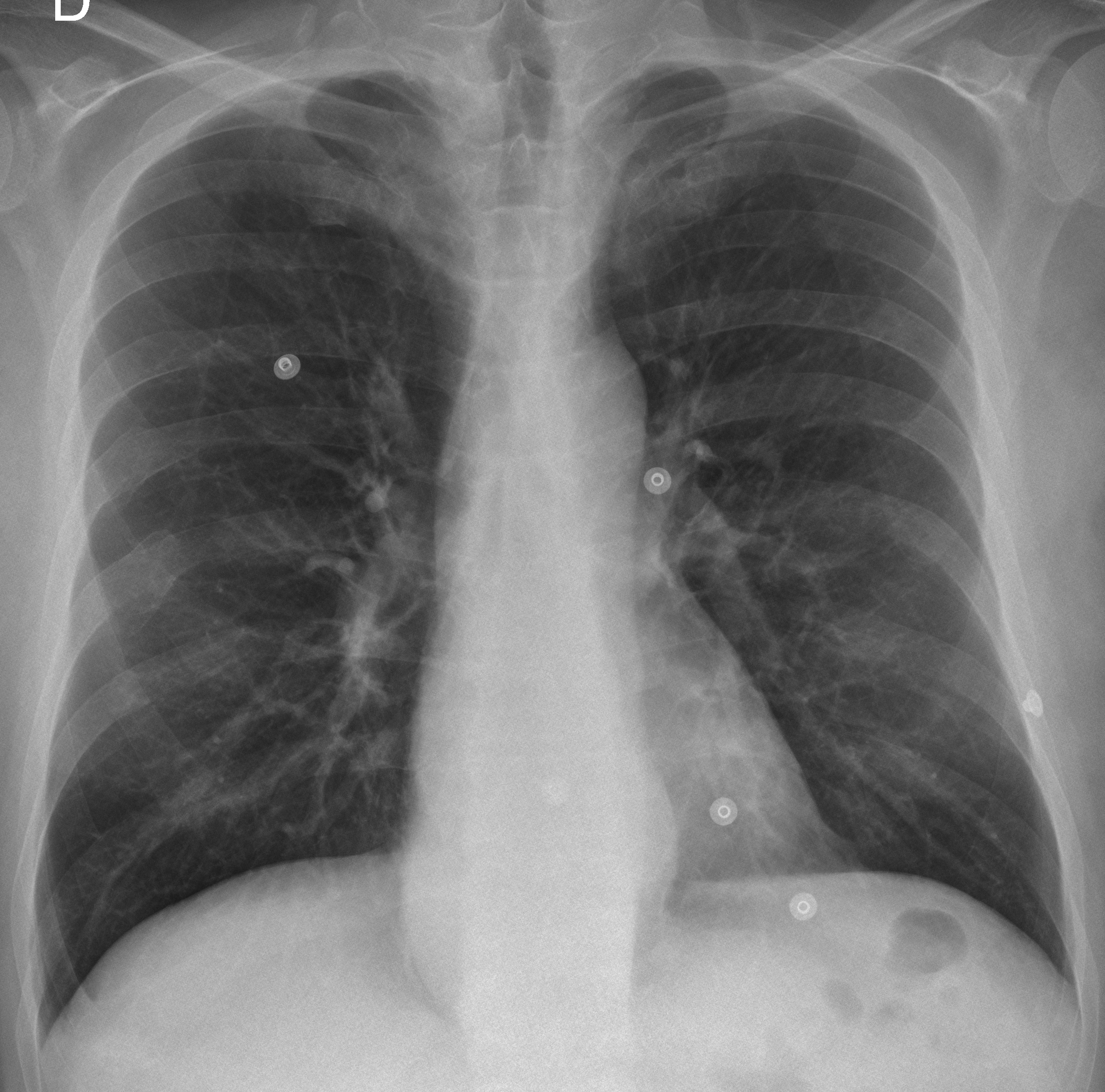
55-year-old man, PA chest
Click here for the answer to case #65
Findings: PA chest shows bulging of mediastinal lines (arrows), which in the lateral view correspond to a lower middle mediastinal opacity with a small air-fluid level (arrow). Although the initial impression is hiatal hernia, widening of the retrotracheal line (red arrow) suggests an alteration of the whole oesophagus.
Coronal CT shows dilation of the oesophagus (A, arrows). Axial CT shows dilated oesophagus as the cause of the apparent widening of the retrotracheal line (B, arrow). CT discovered an unsuspected mass in the tail of the pancreas, which was responsible for the patient’s symptoms (C, arrow).
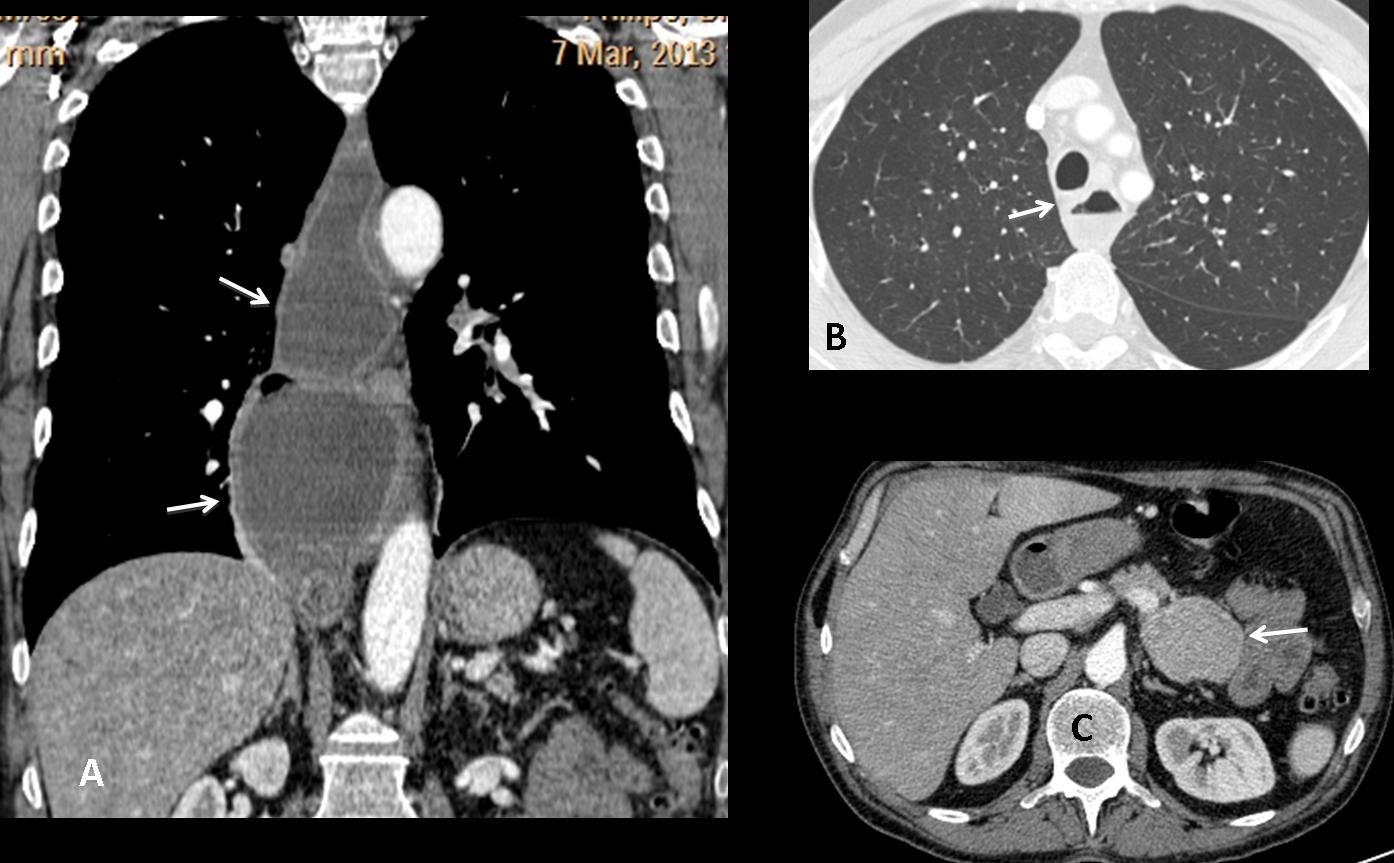
Final diagnosis: oesophageal achalasia. Neuroendocrine tumour of the pancreas.
Congratulations to Genchi Bari, who suggested the diagnosis. Katerina is a close second.
Teaching point: always consider an oesophageal origin of any middle mediastinal mass. Looking at the retrotracheal stripe may be of help, as in the present case.


Hernia iatal . In lateral view there is a little air fluid level . No evidence of gastric nulla in ipocondrium . It’ ok
Hernia iatal . In lateral view there is a little air fluid level . No evidence of gastric nulla in ipocondrium . It’ ok??
Posterior mediastinal winding.. Can be an aneurysm of the descending thoracic aorta at the aortic hiatus.
Posterior mediastinal winding.. Can be an aneurysm of the descending thoracic aorta at the aortic hiatus in addition to hiatus hernia
Carlo you are the man.)
I think carlo is right.
We have rib fractures on the right 6,7,8 too
There is not Lymphoma or Neurogenic tumor
Duplication cystit if is symptomatic is usually identified soon after birth.
Second choice Bronchogenic cyst.
A hiatus hernia does not cause any(Emergency Room) symptoms,but rolling hernias can strangulate a portion of the stomach above the diaphragm.
I think you are right
On the AP chest X/ray there is displacement of the azygoesophageal recess on the right and a paravertebral line on the left, which does not obliterate the shadow of the descending aorta (pseudoparavertebral line). Gastric bubble is not seen under the left hemidiaphragm.
On the lateral X/ray there is a very small air-fluid level in the mass, which is located posteriorly to the posterior heart border (positive silhouette sign) and anteriorly to the spine.
These findings point to a mediastinal process in the lower portion of the middle mediastinum.
The most frequent pathology in this location is hiatal hernia. If the gastric bubble was in the right place and there was no air-fluid level, we could consider also in the differential diagnosis oesophageal tumor (without proximal dilatation of the oesophagus)or varices.
Duplication cysts and enlarged lymph nodes due to lymphoma are more frequently located in the middle portion of the middle mediastinum. Neurogenic tumors are located in the posterior mediastinum.
Therefore, I choose 4. None of the above
Happy Easter to all the Orthodox Christians !!!
Kalo Pasxa !!!
…un piccolo sorso di Gastrgraphin potrebbe fare la diagnosi, di questa “pseudo-massa” localizzta alla base del mediastino posteriore, contornata superiormente dal piccolo livello idro-aereo: io penso ad una ernia iatale gastrica “complicata” da volvolo, il che spiegherebbe il dolore acuto retrosternale.PS : non sempre si può fare ,subito, una diagnosi corretta , cosi’ come non sempre si può vincere. Auguri a Te mitico ed allo splendido Barcellona!!!!
…un piccolo sorso di Gastrographin potrebbe fare la diagnosi, di questa “pseudo-massa” localizzta alla base del mediastino posteriore, contornata superiormente dal piccolo livello idro-aereo: io penso ad una ernia iatale gastrica “complicata” da volvolo, il che spiegherebbe il dolore acuto retrosternale.PS : non sempre si può fare ,subito, una diagnosi corretta , cosi’ come non sempre si può vincere. Auguri a Te mitico ed allo splendido Barcellona!!!!
Hiatal hernia.
I think is a hiatal hernia or paraesophageal hernia? may be related to a volvulus ?
…per completare, la DD potrebbe essere fatta con l’acalasia esofagea: sempre con un sorso di Gastrographin.
Hiatal hernia.
hiatal hernia
There is also a wide tracheoesophageal line on lateral view that suggests esophgeal process or lymphadenopaty. An esophgeal neoplasm could produce this sign plus rib metastases and opacity with air fluid level at the posterior clear space. Achalasia and trauma could be another posibility and would explain the epigastric pain.
Good observation about the retrotracheal stripe. Better late than never!