Showing images of a pre-operative chest for inguinal hernia in a 72-year-old male.
1. Thyroid mass
2. Thymoma
3. Lymphoma
4. None of the above
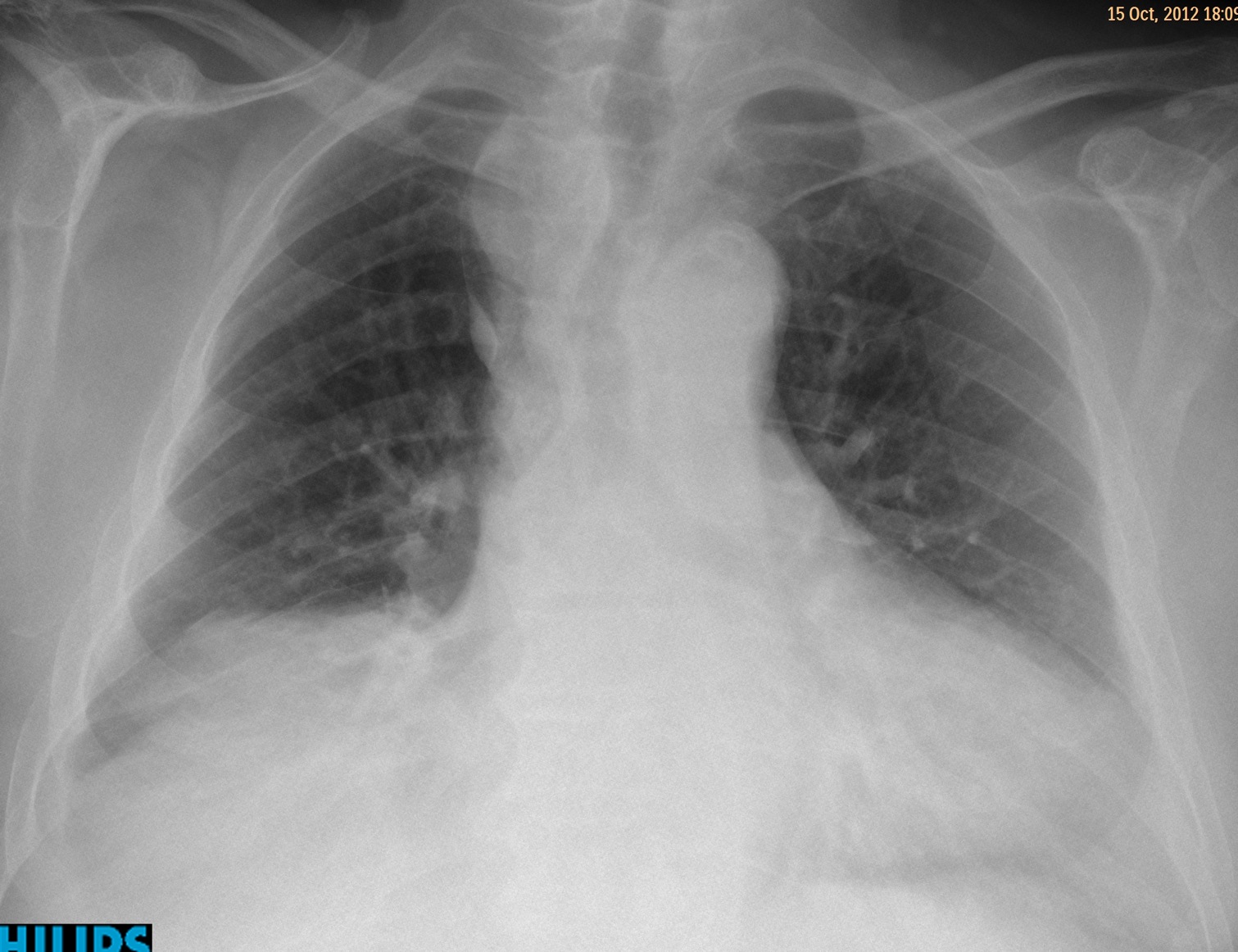
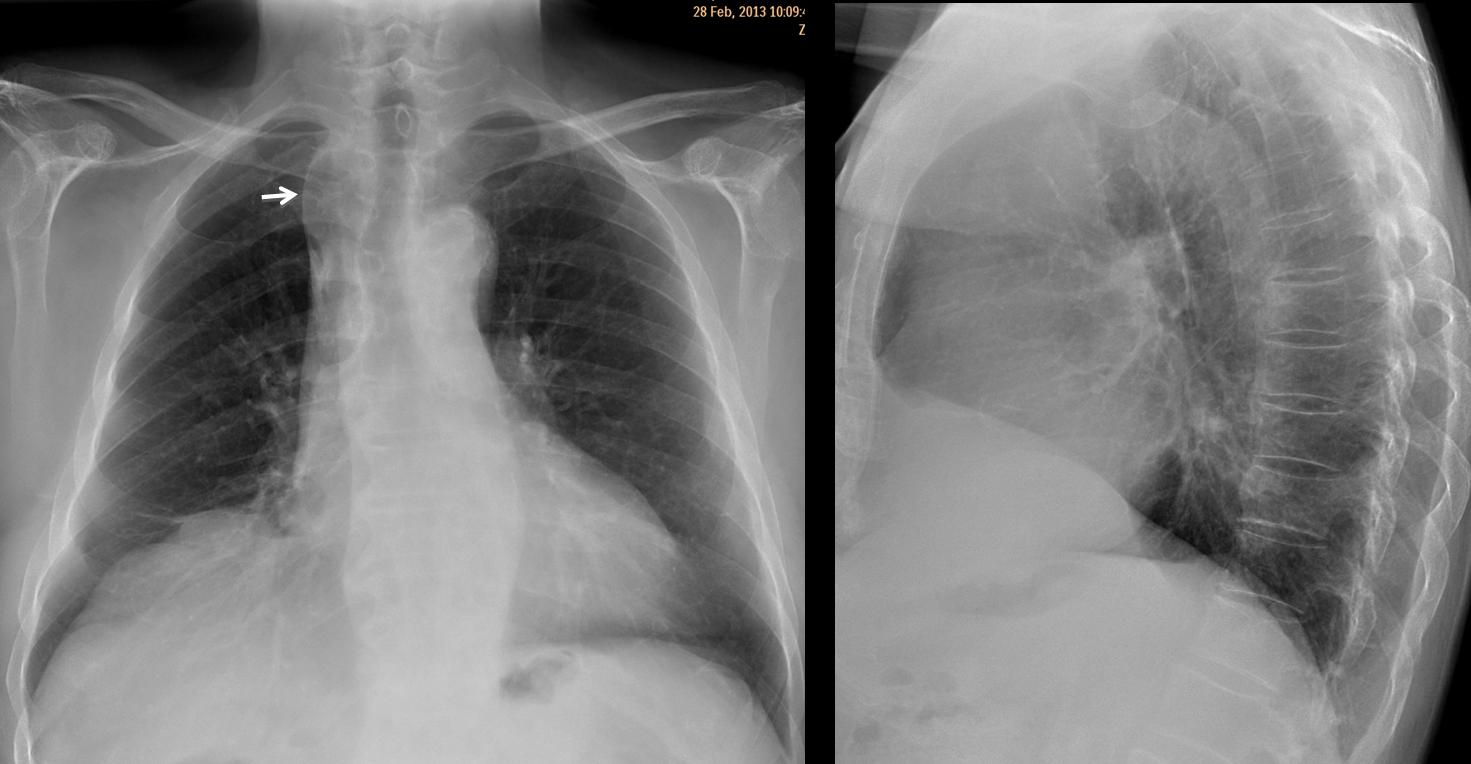
Findings: PA radiograph shows an apparent right upper mediastinal mass (white arrow), slightly displacing the trachea. There is an associated azygos lobe (
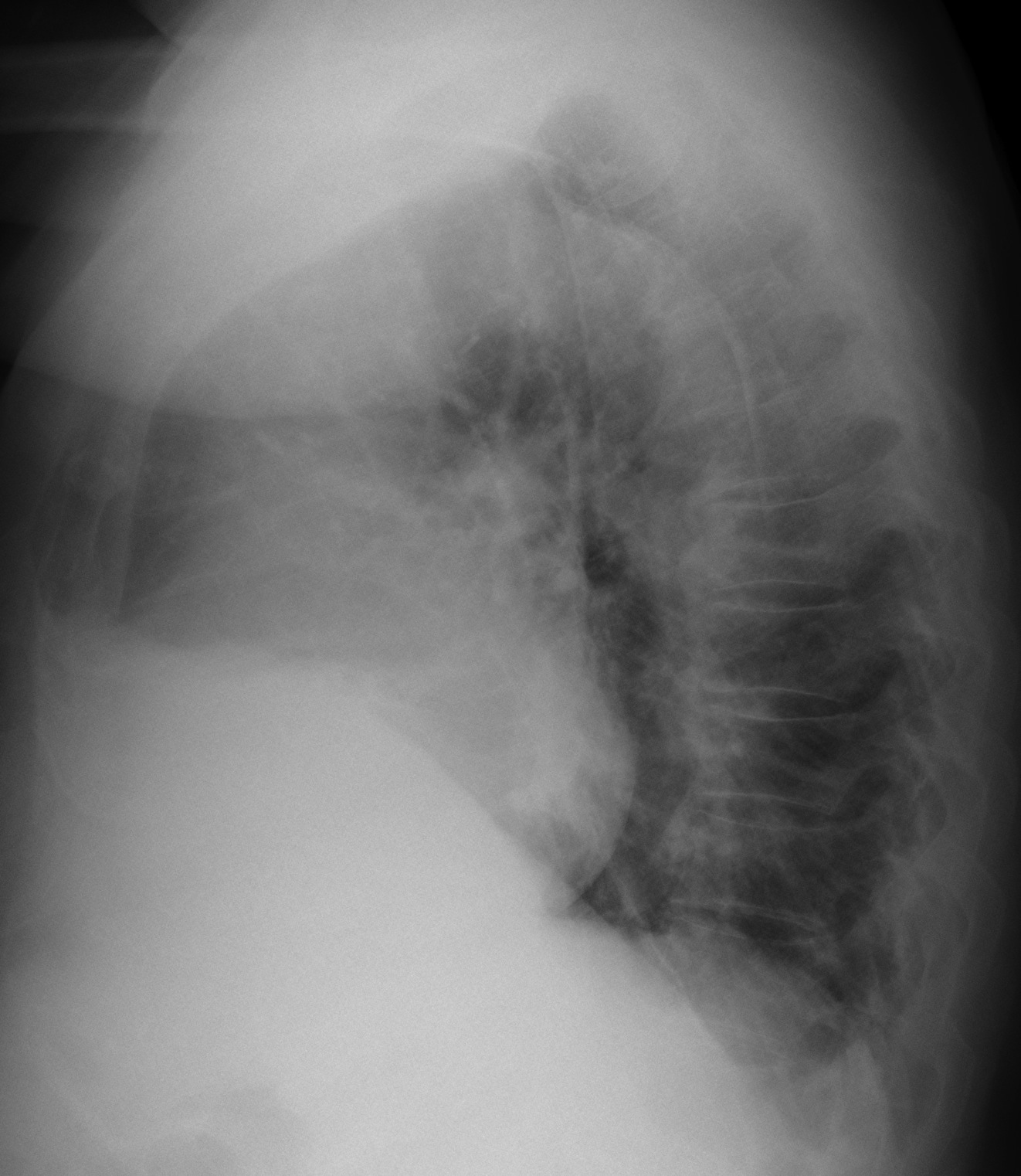
red arrow). Lateral view is non-contributory.
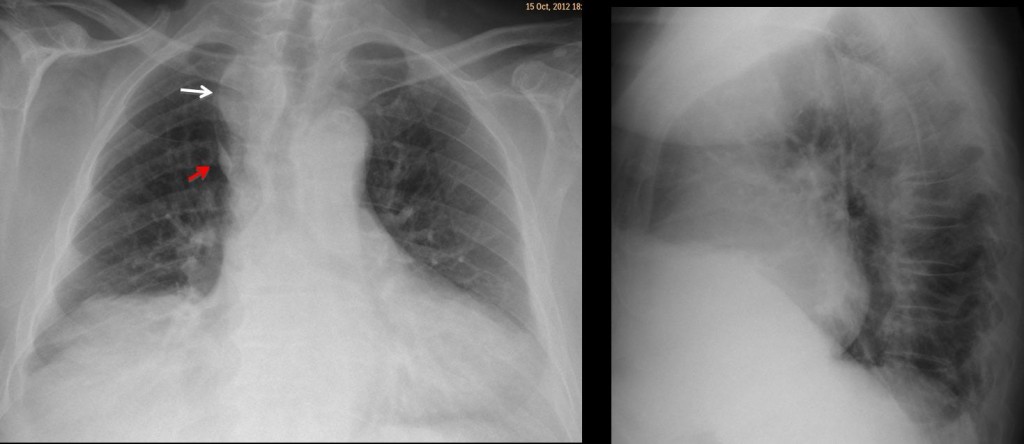
Findings were interpreted as a normal variant, the opaque azygos lobe, in which tortuous supra-aortic vessels in combination with an azygos lobe give the impression of a right upper mediastinal mass. In this particular case, films were not taken in full inspiration, which increased the false impression of a mass. Radiographs taken five months later confirm the original diagnosis (Fig 2).
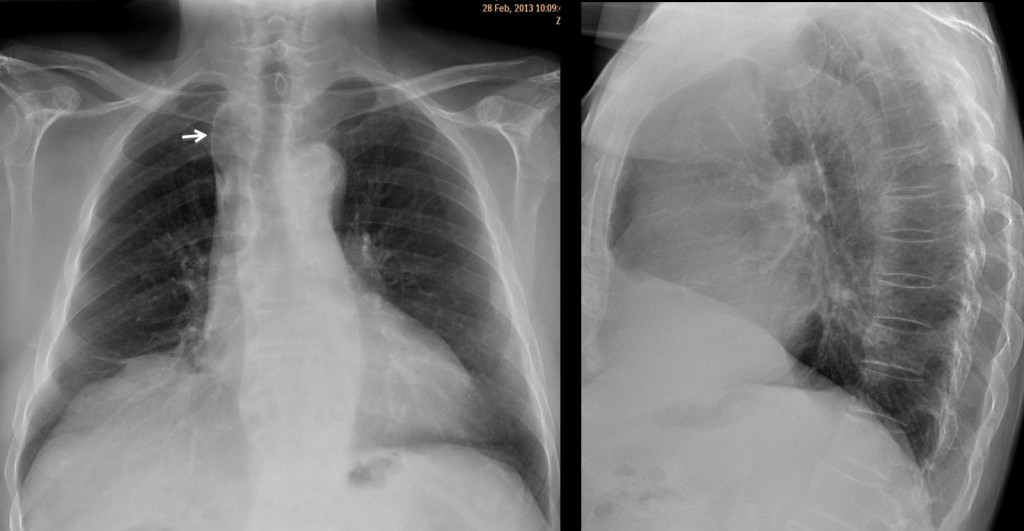
Fig 2. Note the opaque azygos lobe (arrow)
Final diagnosis: opaque azygos lobe (ref. AJR 160:245-48, 1993)
Congratulations to Katerina who reconsidered her original impression and suggested a vascular lesion.
Teaching point: forgive my insistence but, as stated in case 42, remember that vessels compose the mediastinum, basically.



chest ray 2 views
a well defined soft tissue mass is sen at right paratracheal region indenting the trachea medially and limit laterally by azygos fissure , also right hemidiaphragm is elevated by a mass through which the lung vessels are seen ,
however plural angels are clear .
mild left ventriculomegaly evidenced by bulging posterior cardiac border.
so it could be diaphragmatic paralysis due to compressionof right recurrent laryngeal nerve by right paratraceal mas that could be thymoma or bronchogenic carcinoma , also right cardiophrenic angle mass as thymoma migrating down ward with another one at right paratracheal region ,another possiblity is metastasis if thre s known primmary tumor .
s CT chest is advised
Right paratracheal mass with deviation of the trachea to the left (upper middle mediastinal mass). This could be due to a thyroid mass but I would expect to see the maximal tracheal deviation further up at the thoracic inlet. The upper boundaries of the mass are well delineated and project over the level the right clavicle (can not be an anterior mediastinal mass). But on the lateral chest X/ray there is obliteration of the retrosternal clear space suggesting an anterior mediastinal mass. So, there must be both an anterior and a middle mediastinal mass probably due to lymphoma.
Moerover, there is an elevation of the right hemidiaphragm with effacement of the right cardiophrenic angle. This finding could be attributed to the compression of the right phrenic nerve by the paratracheal mass.
The. Right paratracheal stripe is not seen by a paratracheal oval well margined soft tisue mass,shifting the trachea.
Lobus v.azygos.
Dif.dg.lymphoma
I agree with compression of the right phrenic nerve.the problem is with the mass…is too delineated as a cyst or vessel,and the density…
the mass in the upper right mediastinum is well circumscribed and not very dense. i can not identify it on the lateral.
if lymphoma origin in upper mediastinum would imply hodgkin instead of nhl, but patient is in his 70ies, therefore i think lymphoma not very likely.
lobus v. azygos
perhaps it is a fatty mass so no. 4 none of the above.
Opacità di massa localizzata nel mediastino antero-superiore con relaxatio diaframmatica. Reperti accessori, scissura da lobo v. azygos e cardiomegalia.Gli organi e strutture in tale sede, sono tiroide ectopica , timo,linfonodi e residui embrionali.Pertanto la patologia è da ricercare in queste strutture.L’opacità presenta limiti netti, forma ovoidale e non sembra in continuità con la tiroide.Con un pò di “fantasia” che non deve mancare in noi radiologi, azzardo per una linfoadenomegalia isolata come nella Castleman’s disease: riserva per un teratoCR..
There is not true right phrenic nerve paralysis because only the anterior part of the hemidiaphragm is elevated. Maybe there is some RML atelectasis. The right para tracheal mass is well demarcated and has low density. A bronchogenic cyst would be a possibility if he was younger even though it is more common situated in subcarina space. I am a little suspicious over the inguinal hernia because those patients commonly have aneurysms.
So far, the diagnosis has not been mentioned. Think of basic principles!
Maybe esophageal lesion such as diverticula or foregut cyst.
Si sono d’accordo con Maria: dopo aver escluso la natura “maligna” della massa, dovremmo pensare, data la sede, i margini, la densità, la “dolce” impronta sulla trachea a qualcosa di disontogenetico e quindi una cisti broncogena a sede mediastinica.
We always forget the basics professor !!! As you mentioned in case 42: ” remember that the mediastinum is composed basically by vessels “. Having this in mind, the paratracheal lesion must be of vascular origin (aberrant right subclavian artery or double aortic arch?). Taking into account the barely discernible posterior indentation of the trachea in the lateral Xray (I missed it the first time), the dilated aberrant right subclavian artery (Kommerell diverticulum) is my first choice.
Good, at least somebody follow indications!
Tra le cause di impronta ab-extrinseco, sul lato dx della trachea, dobbiamo pensare ad un arco aortico dx-posto: l’arco aortico dx-posto si associa spesso a succlavia dx aberrante con dilatazione aneurismatica alla sua origine(=diverticolo di Kommerel).Farei allora un esofago baritato ed una angiotc.