Dr. Pepe’s Diploma Casebook: Case 10 – SOLVED!
Dear Friends,
This week’s case is an 85-year-old man with weight loss. Would you call this study normal?

Fig. 1: 85-year-old man with weight loss
Findings:
Diffuse, curvilinear, low-density lines (arrows) in the small bowel suggest intramural gas collections.
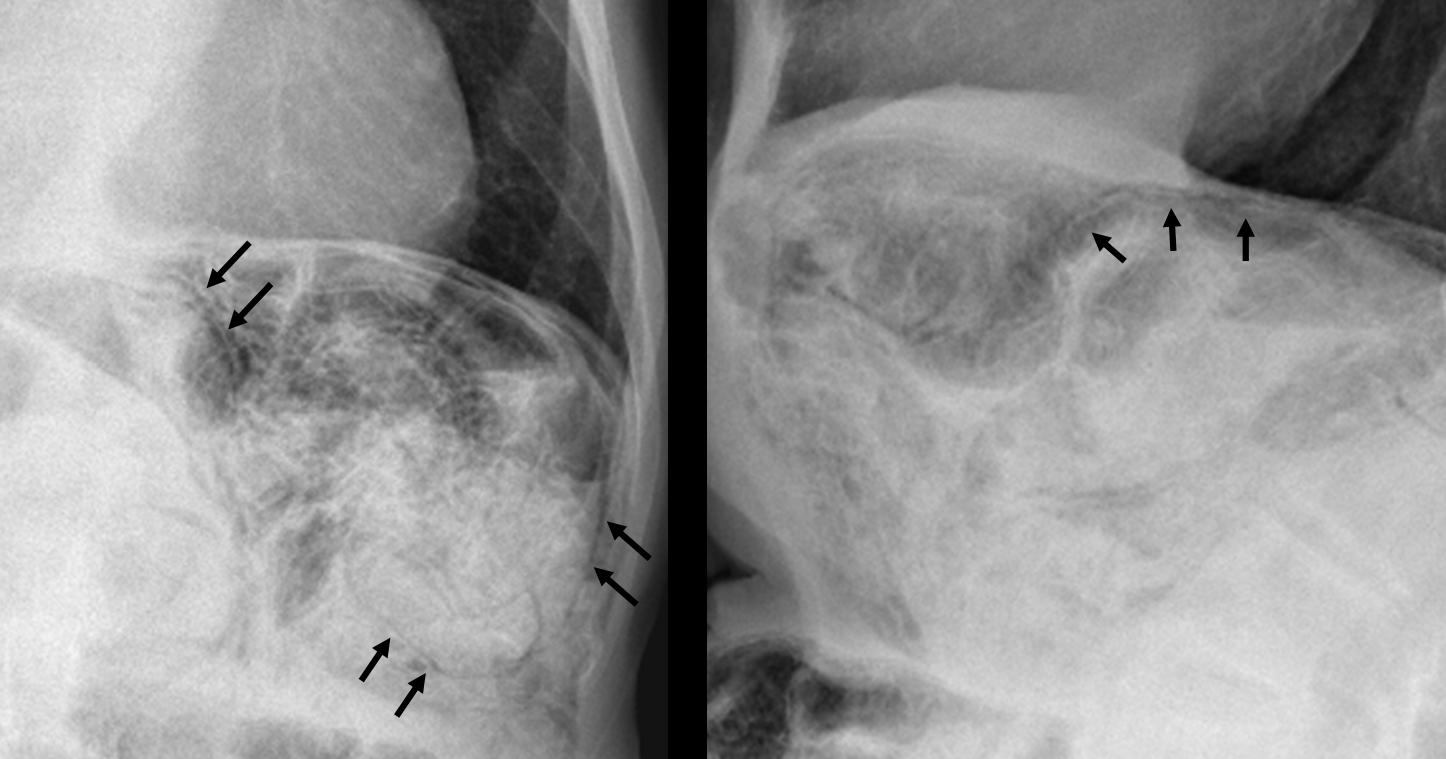
Fig. 2
CT confirms air in the jejunal walls (black arrows). No free air is seen.
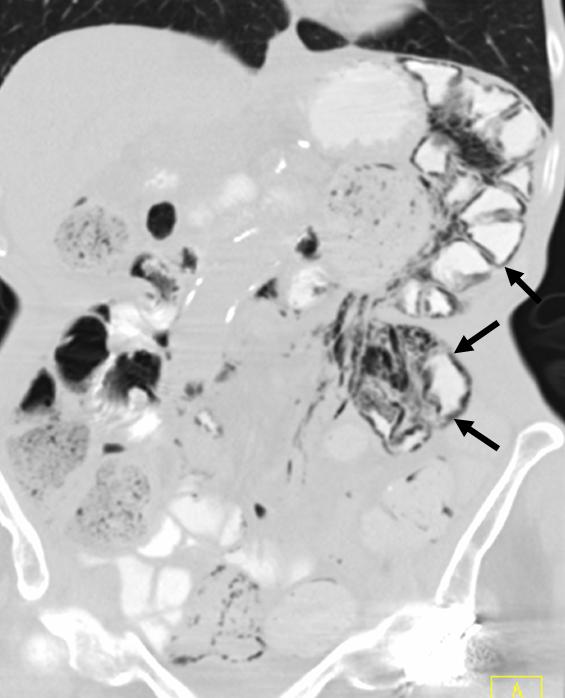
Fig. 3
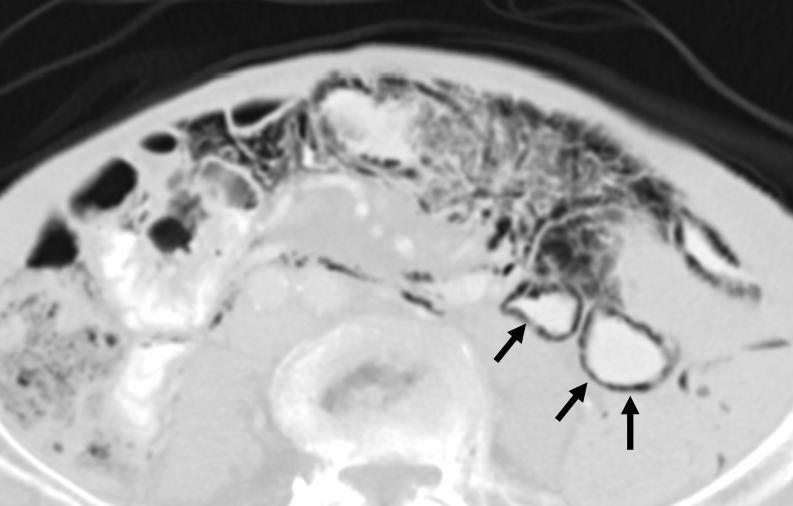
Fig. 4
Final answer: Pneumatosis intestinalis, secondary to bowel ischemia
Pneumatosis intestinalis (PI) is defined as the presence of gas in the bowel wall.
On both radiography and CT, PI usually appears as a low-density linear (Fig. 5a, arrows) or bubbly (Fig. 5b, arrows) pattern of gas. PI is a sign, not a disease, and it must be interpreted relative to the patient’s overall clinical condition.
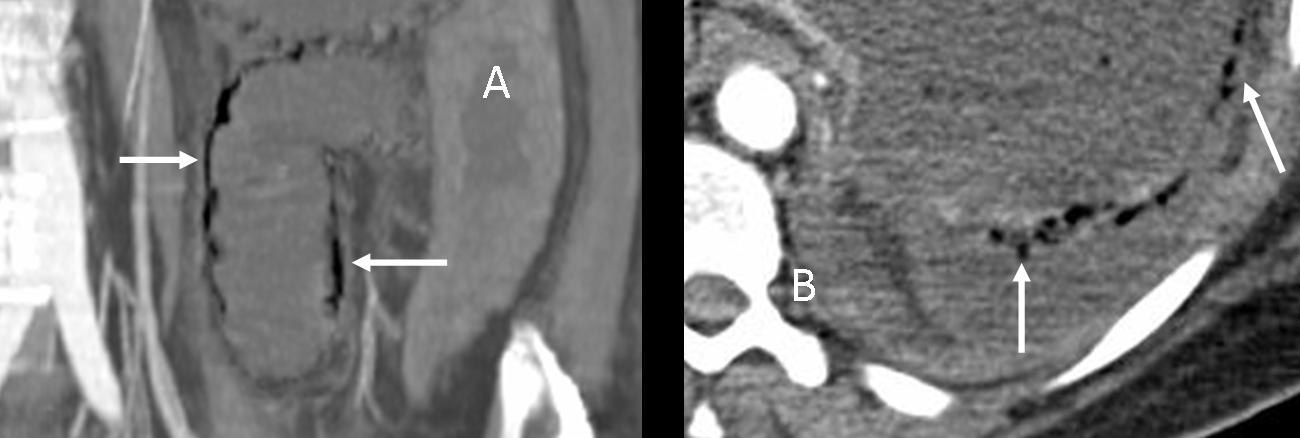
Fig. 5
PI has many causes, ranging from benign to life-threatening conditions. Clinical symptoms and laboratory data provide important clues to clarify whether PI is due to a benign or life-threatening cause. CT can be of help.
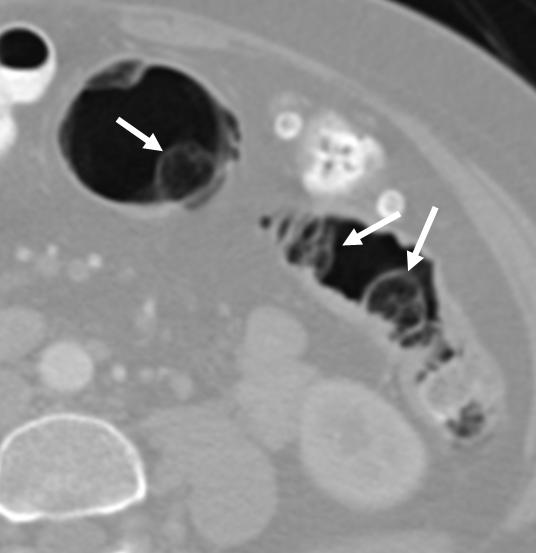
Fig. 6
Pulmonary and intestinal diseases are the most common benign causes of PI. Pneumatosis cystoides intestinalis (PCI) is a type of PI characterised by spherical gas collections in the bowel wall (arrows). PCI almost always occurs in the colon, and on colonoscopy it can mimic polyps. When viewed with CT colonoscopy, the gas cysts can be easily identified within the colon wall.
The most common life-threatening cause of pneumatosis intestinalis is bowel ischaemia. The combination of PI and an elevated serum lactic acid level is associated with a greater than 80% mortality rate.
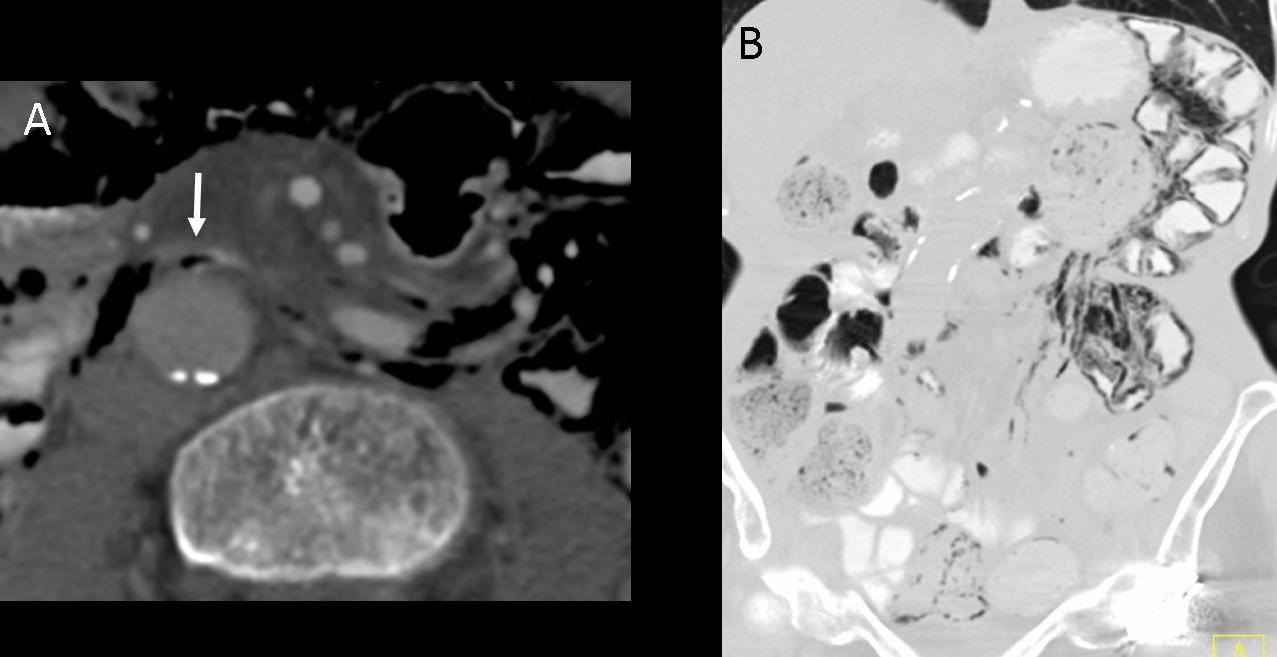
Fig. 7
CT shows gas within the mesenteric veins (white arrow in Fig. 7a). The distribution of PI is confined to the jejunum (Fig. 7b). When PI is confined to a portion of the small or large bowel within a specific vascular territory, ischaemia is the likely cause. Enteric capsule study demonstrated bowel ischaemia in this patient.
Pneumatosis secondary to infection
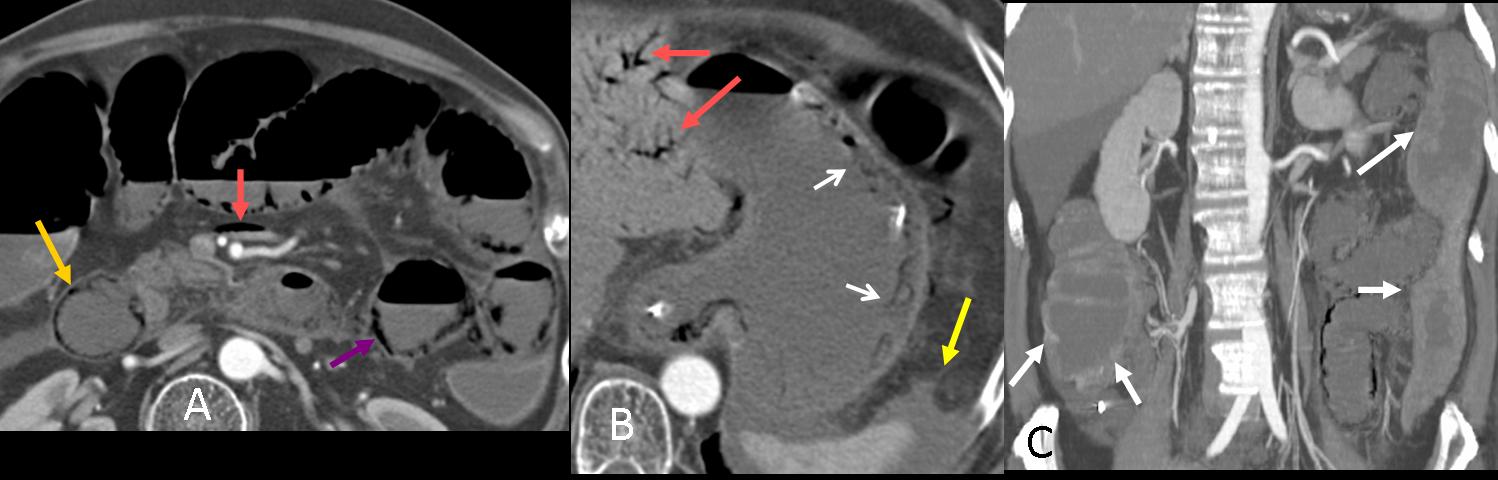
Fig. 8
PI in the duodenum (Fig. 8a, yellow arrow) and jejunum (8a, purple arrow) secondary to chemotherapy and infection in a patient with oesophageal neoplasm. In this case, gastric pneumatosis is also present (8b, white arrows). This PI distribution does not correspond to a specific vascular territory.
The presence of bowel wall thickening (white arrows), absent or intense mucosal enhancement, dilated bowel (8c, white arrows), arterial or venous occlusion, ascites (8b, yellow arrow), and hepatic portal or portomesenteric venous gas (8a and b, red arrows) increases the likelihood that pneumatosis has a life-threatening cause.
Portal venous gas
CT is more sensitive than radiography in detecting hepatic portal and portomesenteric venous gas, the presence of which increases the possibility of PI due to life-threatening causes. Portal venous gas (Fig. 9a, white arrows) can be differentiated from biliary gas (Fig. 9b, arrowheads) by its characteristic tubular branching lucencies that extend to the periphery of the liver, whereas biliary air is more central.

Fig. 9

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
Pneumatosis intestinalis can be diagnosed in chest radiographs: look below the diaphragm when you read the film.
CT differentiates benign from life-threatening causes: cystic appearance suggests a benign condition. To diagnose life-threatening entities look for air in the mesenteric veins, clots within the mesenteric arteries, air in portal veins and additional bowel findings.
Suggested reading
- Pneumatosis Intestinalis in the Adult: Benign to Life-Threatening Causes. AJR 2007; 188:1604–1613.
- Pneumatosis intestinalis versus pseudo-pneumatosis: review of CT findings and differentiation. Insights Imaging. 2011;2:85-92.
Case prepared by Alberto Villanueva MD


bowel, chest, diagnosis, EDiR, European Diploma in Radiology
No.
It identifies a thoracic aortic elongation senile degenerative spine changes with previous marginal osteophytes and vertebral body wedging dorsal anterior low.
A striking arrangement of abundant bowel below the left diaphragm, that given the patient’s clinical context, it would be advisable to continue the study with abdominal ultrasound.
An abdominal ultrasound is of no use in evaluating bowel.
Findings:
1. Gas under the diaphragm, especially on the left and extending medially.
2. Wedging of T10 – looks like an oldstanding osteoporotic collapse…posterior elements preserved.
3. A possible (cavitating) lesion in the lower retrosternal space…must measure around 3-4 cm
Cardiothoracic ratio borderline, thoracic aorta might be at the upper limit of normal…
The diagnosis we need to exclude here is a gastric/colo-rectal NG … might have perforated (ie T4 by definition) and have spread (? cavitating pulmonary deposit).
I would recommend CT and gastro-colono-scopy.
There is a free air in the below of the left diapragm.suggesting that an abdominal perforation.also there Might be a deep sulcus sign. Pneumomediastinum.?
Is tahsis Right?
See answer by Rahul, below
During oral part of the examination How would we should answer the questions? Say all the findings ?
When the examiner presents a case you should describe the findings and make a differential diagnosis. You can suggest any additional examination which will clarify the diagnosis.
Crushing T10
no
thoracic aortic elongation and widening
” Troppo” bella la silhouette cardiovascolare in LL, perchè delineata da aria “libera” nel mediastino:pneumo-mediastino.A ciò si aggiunge sottile falda di aria libero in addome:pn-peritoneo, con anomala morfologia del contenuto intestinale in sede sottodiaframmatica sx. La “fisiologica” comunicazione tra lo spazio retroperitoneale ed il mediastino, suggerisce che la patologia è a livello colico distale.Un clisma opaco con mdc iodato idrosolubile( Gastrographin diluito) può chiarire la patologia di base.
Siccome la TC è un esame diagnostico di natura molto più informativa, perché non fare TC in prima istanza invece della clisma opaca? Entrambi coinvolgono raggi X, ma la TC ci da più informazione, e può servire come esame di stadiazione se la causa del pneumo-peritoneo fossi una K colon perforata.
1.Emphysema pulmonum.Bronchitis chronica.Cardiomegalia,Fractura Th-9 consolidata.Spondyloarthrosis deformans.Chilaiditi’s syndrom.
Mottled and curvilinear lucencies in the region of the splenic flexure are concerning for large bowel pneumatosis. Additionally there appears to be gas under the left hemidiaphragm. Correlation with the patients serum lactate as well as a CT abdomen with a CT angiogram to evaluate the mesenteric vasculature is warranted to exclude ischaemic colitis.
Excellent diagnosis and discussion. Congratulations
deep sulcus sign ?
should be more MSK ,Cardiovascular MRI and thorax questions .
We are working on it. But we also need breast cases, pediatrics, etc.
I think that this can be SİGMOİD VOLVULUs
I think that this can be a sigmoid volvulus
I agree with all these chest findings.
Additionally there are signs of bowel pneumatosis or/and free air below diafragm.
There are air filled bowel loops under the left hypohondrium.
It seems that there is free abdominal air under the left hemidiaphragm.
There is a small cavitating lesion at about the medial segment of medial lobe.
We can see anterior wedging of a lower thoracic vertebra, with height loss, (there is no clear evidence of bone reaction, it could possibly be an osteoporotic fracture)
Possible diagnosis: intestinal tumor , with bowel perforation and cavitating pulmonary metastase. Pathologic or osteoporotic vertebral fracture.
Farther investigation needs to be taken, like bone scintigram, thoracic and abdominal CT, bood tests for cancer markers, etc.
1. Free air under the left diaphragm
2. Distended splenic flexure with pneumatosis
3. Pneumomediastinum
4. Air (free?) on the left of the trachea just above the aortic arch
Possible cause: bowel perforation (probably colon), ischaemic colitis, previous colonoscopy
Suggested exams: CT
Other findings:
5. Pulmonary emphysema
6. Increased anterior-posterior diameter of the trachea (tracheobronchomegaly?)
7. Wedging fracture (probably old) of TH10
8. Increased diameter of thoracic aorta
9. Cardiomegaly
Cystic lesions bilateral hila
Anterior wedging of one of dorsal vertebra
Free air abdomen
In context of history of wt loss possibility of mitotic aetiology cannot be ruled out
Adv ct thorax and abdomen
Left colonic pneumatosis, pneumoperitoneum, pneumomediastinum, weight loss, all these suggest a probable obstructing colon carcinoma.
Beside, I can see some small lung nodules, metastatic ?
There should be more MSK , head and neck,Cardiovascular imaging Cases.
Free subdiafragmatic air, pneymoperitoneo. Body thoracic vertebrae fracture.