The following case depicts MRI images of a 59-year-old woman with rapid cognitive decline, progressive change of character, ataxia and diplopia.
Diffusion-weighted imaging reveals diffuse bilateral striatal and putaminal hyperintensity (arrows). ADC map shows decreased signal, indicating diffusion restriction (arrows).
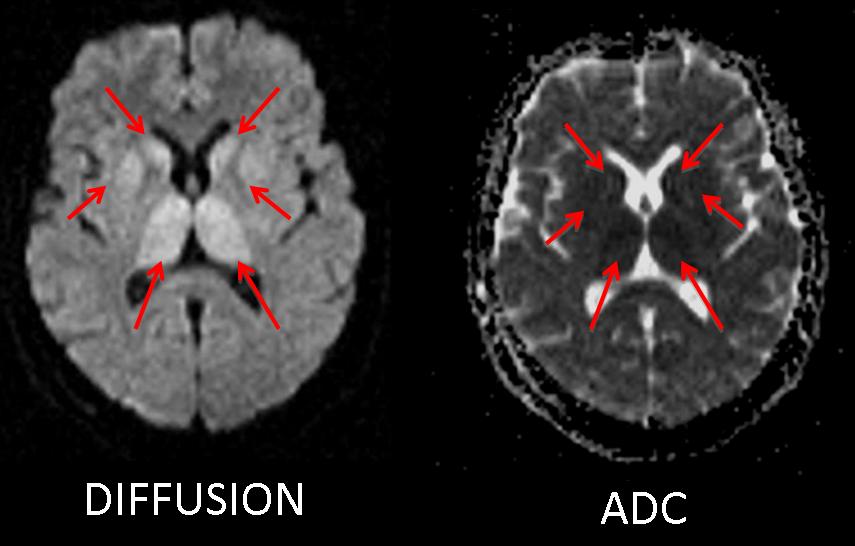
Fig. 1
Findings on T2W and FLAIR images: high signal intensity in both basal ganglia, and thalamic involvement (arrows). Diffusion-weighted imaging is superior to T2W or FLAIR in depicting lesions. Without diffusion-weighted imaging, some of the lesions might be missed.
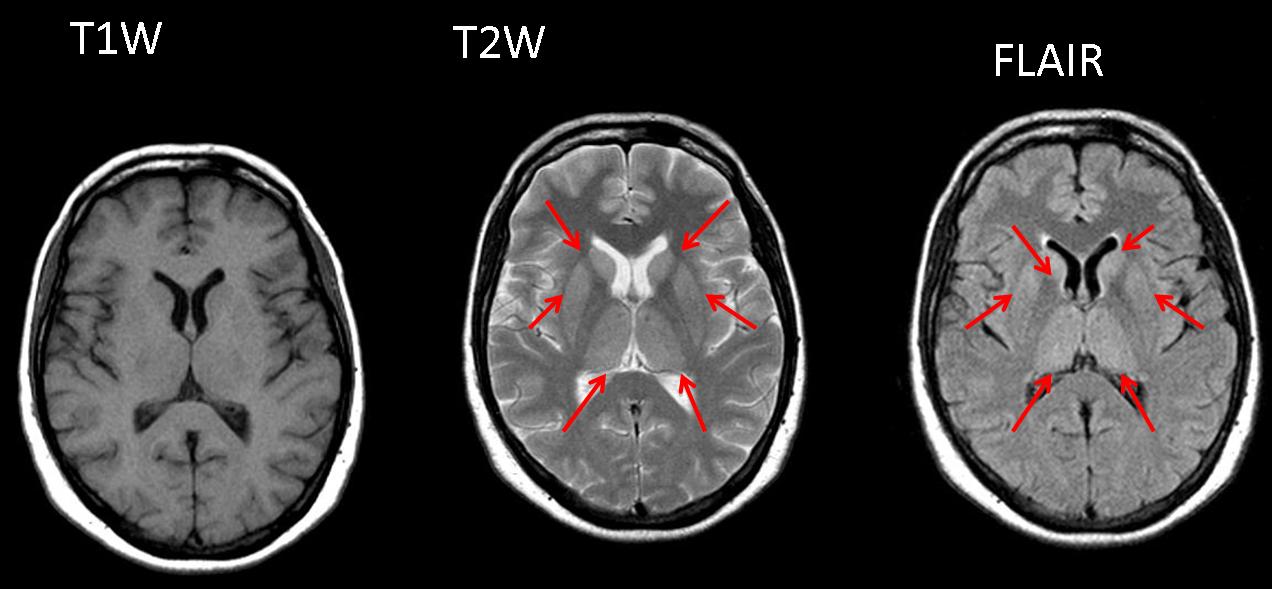
Fig. 2
Final diagnosis: Creutzfeldt-Jacob disease. Positive 14.3.3 protein in CSF.
14.3.3 is a neuronal protein that is released into the CSF during rapid destruction of the brain. In the context of rapidly progressive dementias, 14.3.3 protein has a sensitivity of 94% and specificity of 84% for the diagnosis of Creutzfeldt-Jacob disease.
Creutzfeldt-Jacob disease (CJD) is one of the transmissible spongiform encephalopathies. A number of CJD subtypes have been recognised, including sporadic CJD (the most common form worldwide), familial CJD, iatrogenic CJD, and the recently described, variant CJD.
Sporadic CJD most commonly affects patients between 60 and 75 years. It presents clinically with rapidly progressive dementia, ending in akinetic mutism.
On MR imaging, symmetrical hyperintensity (relative to cortical gray matter signal intensity) of the caudate head and putamen has been described in 67% to 79% of cases. Other gray matter structures may be affected, including the hippocampus, peri-aqueductal gray matter, and thalamus. DWI is the most sensitive sequence for CJD, with a reported sensitivity of up to 100%.
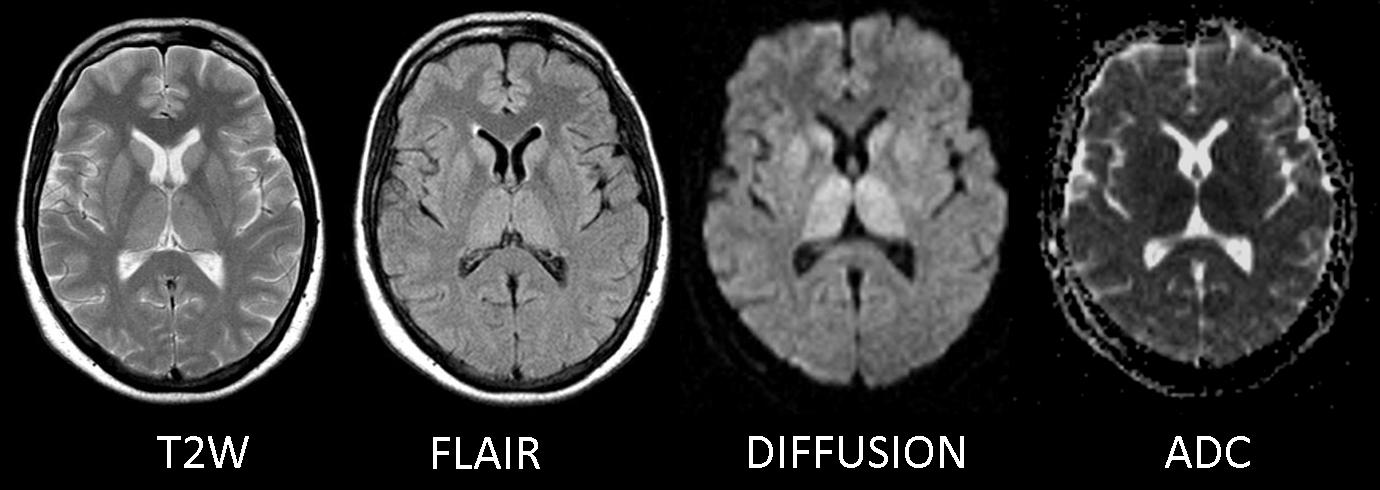
Fig. 3
Wilson disease is an uncommon, autosomal recessive, inborn defect of copper metabolism characterised by abnormal accumulation of copper in various tissues, particularly in the liver and the brain. The most frequently identified abnormality on MR imaging is bilateral symmetric high signal intensity in the putamen, caudate, and thalamus on T2-weighted images
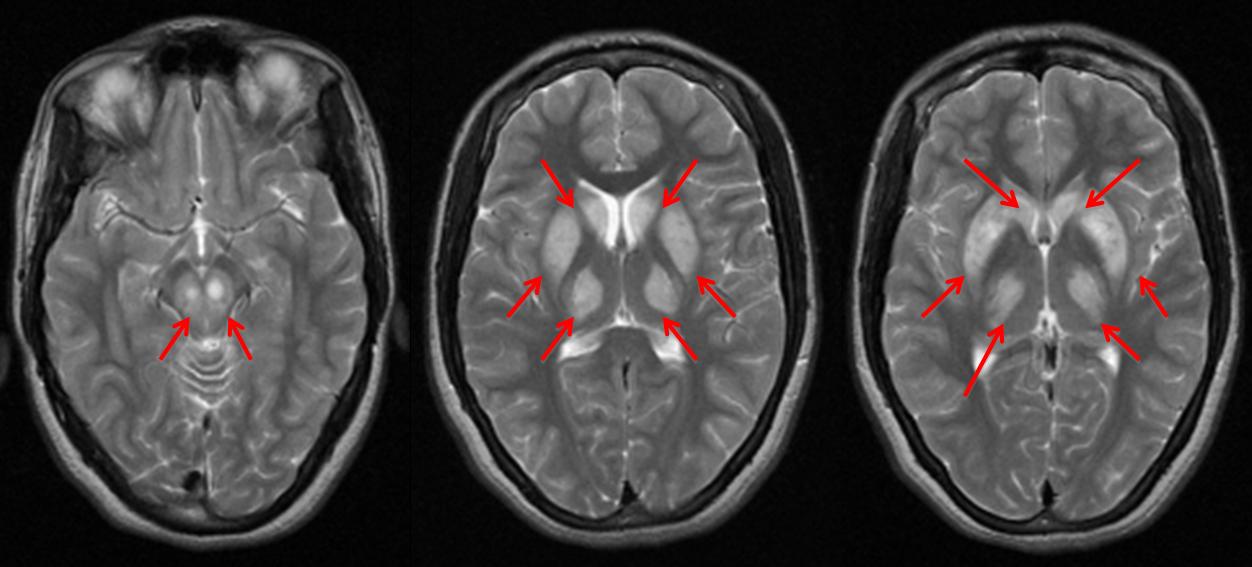
Fig. 4
Wilson disease (above). 18 year-old woman with tremor and behavioral changes. Chronic liver disease. Kayser-Fleischer ring on the eyes. T2W images reveal bilateral putaminal, striatal nuclei, and mesencephalic hyperintensities (arrows).
Posterior reversible encephalopathy (PRES) is a syndrome characterised by oedema, frequently symmetrical, in parieto-occipital areas. It may have other distribution patterns (frontal, temporal, brainstem, and basal ganglia) with a variable appearance on MRI imaging.
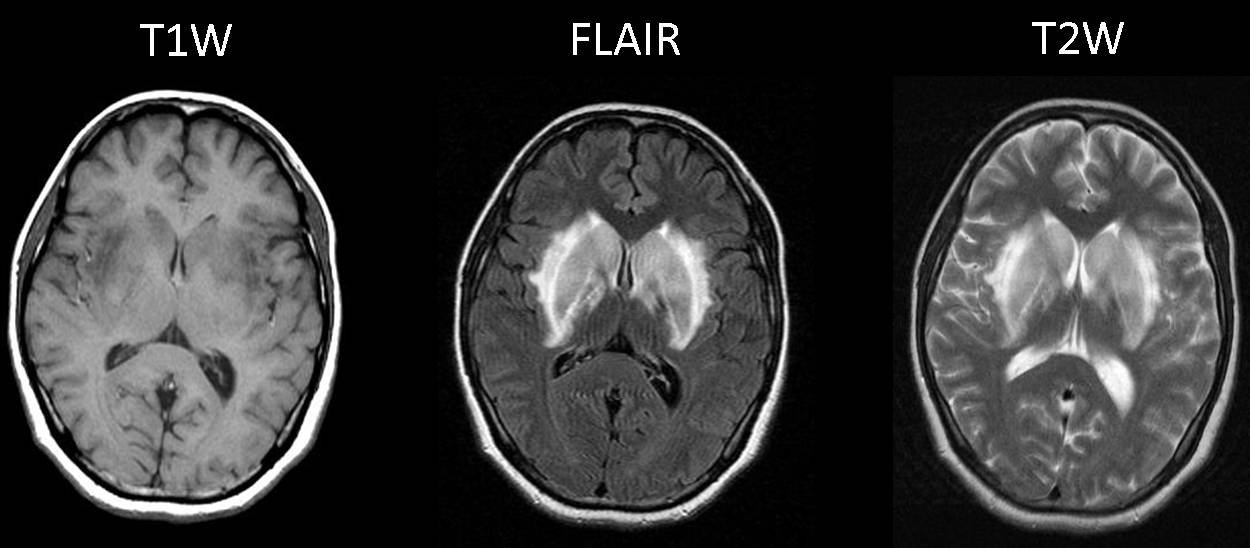
Fig. 5
Fig. 5 (above): 24 year-old woman with headache after cesarean delivery. Blood pressure 170/95. MRI shows hyperintensity at the basal ganglia on T2W and FLAIR images.
Symmetrical vasogenic oedema without restriction on DWI (arrows). 11% of patients show cytotoxic oedema with restriction on DWI; these patients have a poorer prognosis and increased risk of bleeding.
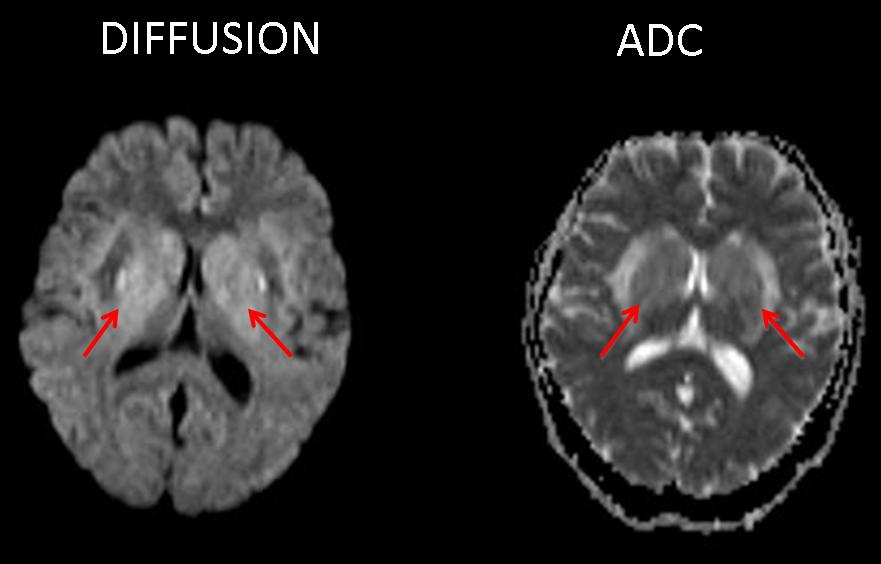
Fig. 6
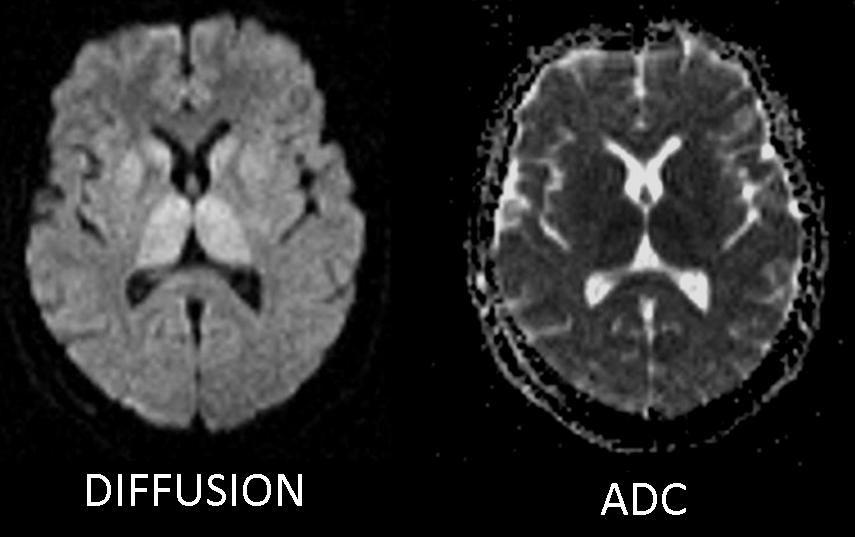
Fig. 6 (above): on diffusion images, there is increased signal due to the T2 shine-through effect, not restriction. ADC map does not show a decreased diffusion coefficient.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- In more than two-thirds of patients, Creutzfeldt-Jacob disease shows symmetric hyperintensity of the caudate head and putamen.
- DWI is the most useful sequence in CJD, with a sensitivity of up to 100%.
- The differential diagnosis of basal ganglia lesions should include hypoxia, Wilson disease, PRES, carbon monoxide poisoning, and infarcts.
Recommended reading:
- 1-Conspicuity and Evolution of Lesions in Creutzfeldt-Jakob Disease at Diffusion-Weighted Imaging. AJNR 2002 23: 1164-1172.
- 2-Creutzfeldt-Jakob disease: comparative analysis of MR imaging AJNR 2006; 27:1459-62.
Case presented by Laura Oleaga, MD


Restricted diffusion in the thalamus, caudate, and lentiform nuclei (high signal on the heavily B weighted image, corresponding low signal intensity on ADC).
Pattern is mostly suggestive of CJD, probably the variant form.
I also choose No.3; CJD.
PRES (although could has thousands of faces) should be distributed around posterior circulation territories. The most often manifestation is a vasogenic edema, wich by definition has incresead difussion, in the occipital lobes. The clinical seeting is also helpful to establish the diagnosis (its usually associated with arterial hypertension and courses with headache and visual alterations as the most often manifestations.
Wilson usually affects the basal ganglia in this distribution (although most often not the whole thalam)and could has a restricted diffusion in early phases. The clinical setting is usually also helpful. The most characteristic feature is the T1 hyperintensity.
CJD is the one of the three possibilities that is more possible in the clinical setting and more over the restricted diffusion is the most important feature to suggest the diagnostic as far as I concern.
Other possibilities I would contemplate are the hypoxic-ischemic encephalopathy and the osmotic myelinolisis (both should have an specific clinical sceneraio); and on the other hand vascular etiology (ischemia), specially deep venous thrombosis and posterior circulation arterial infarcts (including Percheron artery variants) -the symptoms should be more abrupt-.
Summarising, I would choose (obsvisously in the clinical scenario and obviating all the other sequences) CJD. Anyway, I think it is not possible to establish the diagnostic only with these images.
WOW! I believe you are ready to take the eaxmination.
Creutzfeldt-Jacob disease
MRI findings and clinical presentation are strongly sugestive of CJ
wilson dz