Dr. Pepe’s Diploma Casebook: Case 23 – SOLVED!

Dear Friends,
This week I’m showing the case of a 26-year-old male presenting with chest pain.

23 year-old male with chest pain
23 year-old male with chest pain
23 year-old male with chest pain
Most likely diagnosis:
1. Hypertrophic cardiomyopathy
2. Leiomyosarcoma
3. Cardiac rhabdomyoma
4. None of the above
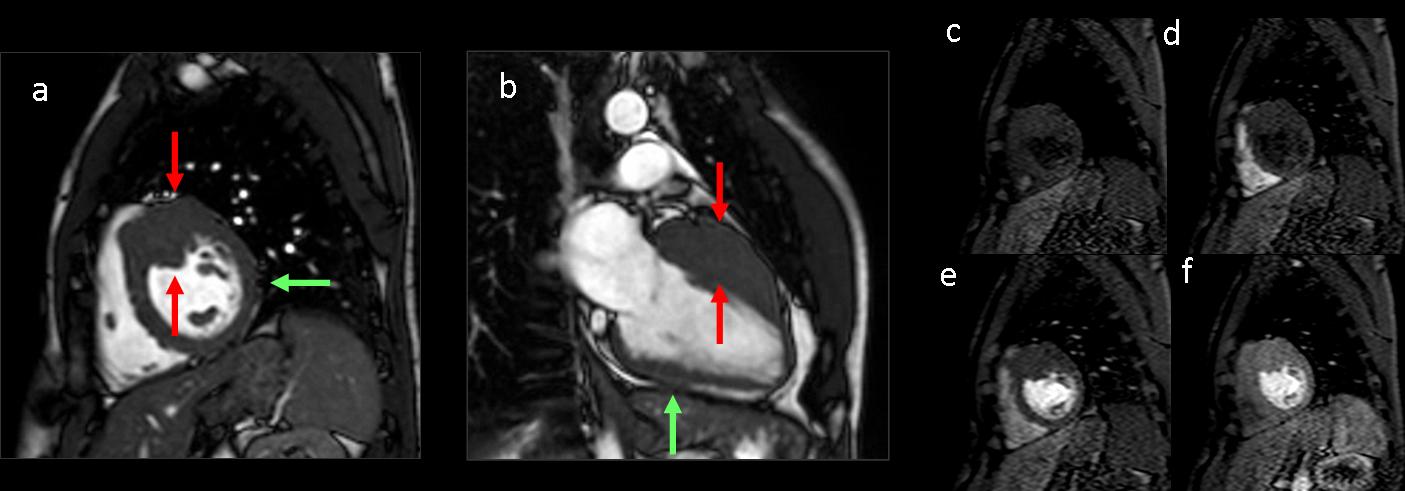
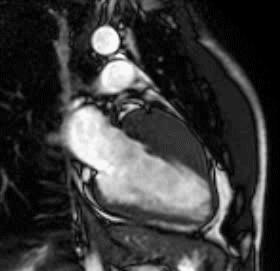
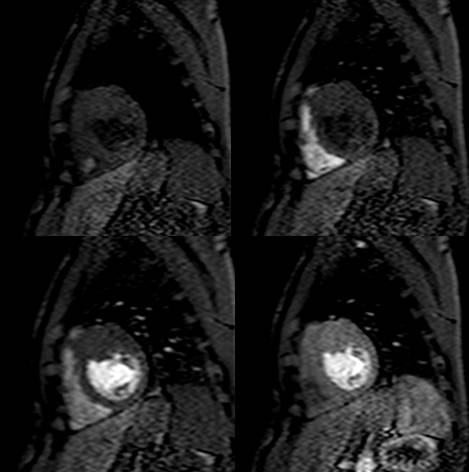
Findings: Short-axis (a) and two-chamber (b) cine-MRI show myocardial thickening (>40 mm) at the anterior segment of the left ventricle wall (red arrows). Compare with the thickness of the normal wall (green arrow). (c-f) Dynamic first-pass perfusion during Gd-DOTA injection. The anterior segment signal intensity is homogeneous in all phases of perfusion and similar to that of the adjacent normal myocardium.
Focal thickening of the myocardium can be due to hypertrophic cardiomyopathy (HCM) or neoplastic disease. Neoplastic masses such as primary or metastatic myocardial tumours show heterogeneous signal intensity, and enhancement and perfusion characteristics different from those of the remaining left ventricle wall.
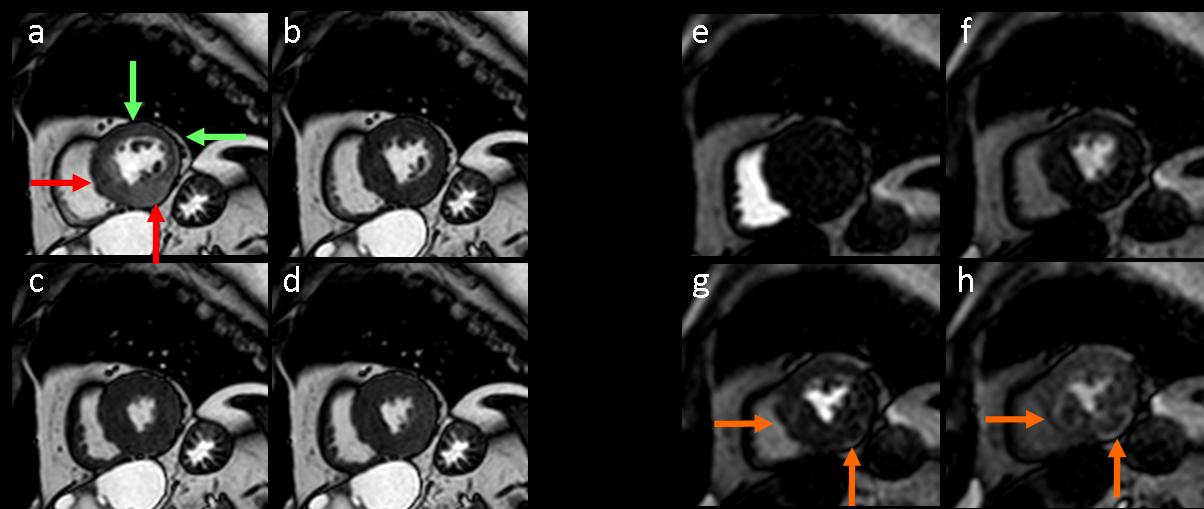
Fig. 2
Figure 2. 78-year-old man with multiple masses due to metastasis from a renal cell carcinoma. Short-axis cine-MRI (a-d) at different phases of the cardiac cycle. At end-diastole (a) myocardial thickening is seen at the septal and inferior segments of the left ventricle wall (red arrows). Note the thickness of the normal wall (green arrows). (e-h) Dynamic first-pass perfusion during Gd-DOTA injection. The septal and inferior segments show heterogeneous enhancement during perfusion (orange arrows).
- Mass-like hypertrophic cardiomyopathy presents as focal hypertrophy with segmental location of myocardial disarray and fibrosis. Perfusion is homogeneous and similar to that of the normal myocardium.
- Final diagnosis: mass-like hypertrophic cardiomyopathy
Maximal left ventricle wall thickness >15 mm in the end-diastolic phase is the morphological diagnostic criterion for HCM. The expression of the hypertrophy is variable and heterogeneous. HCM phenotypes include asymmetrical septal involvement as the most common form of the disease, as well as apical, symmetrical, midventricular, mass-like, multifocal, and diffuse forms.
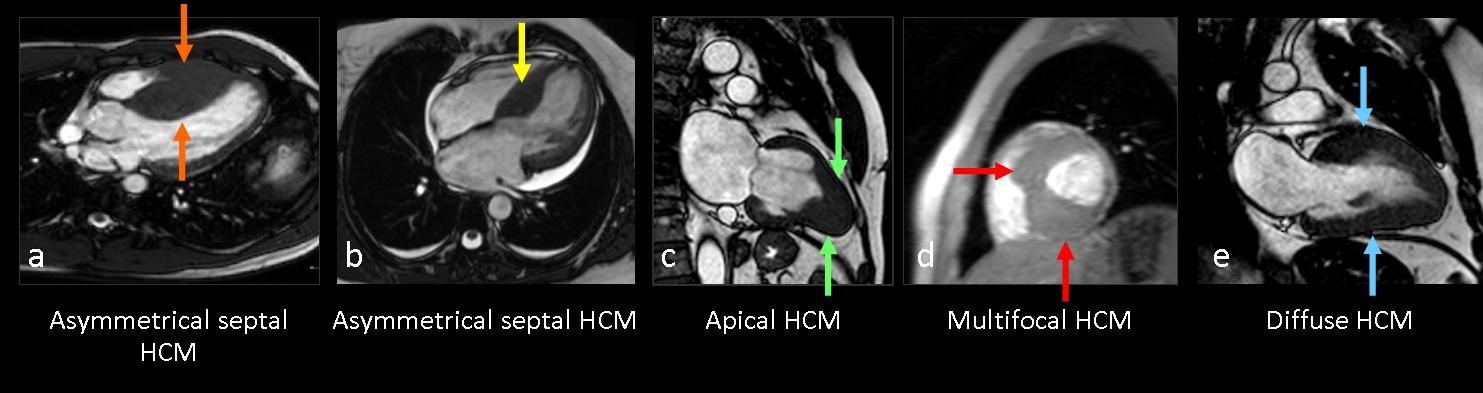
Fig. 3
Figure 3. HCM phenotypes in four different patients. (a) Horizontal long-axis cine MR view shows septal enlargement (orange arrows). (b) Four-chamber cine MR depicts asymmetrical septal HCM involving the basal segments (yellow arrow). (c) Two-chamber cine MR shows apical thickening (green arrows). (d) Short-axis cine-MR view demonstrates multifocal mass-like hypertrophy in the anterior and inferior wall (red arrows). (e) Two-chamber cine MR shows diffuse thickening (blue arrows).
Mass-like HCM shows myocardial contractility, whereas there is an absence of active contraction in tumours. Myocardial tagging with the steady-state free precession technique is useful to detect contraction in the mass-like myocardium.

Fig. 4
Figure 4. Short-axis views of myocardium obtained at four successive trigger delays show active displacement and deformation of tags in regions of localized hypertrophy in the anterior segment similar to contraction in the entire ventricle wall (red arrows).
Sudden cardiac death is an unpredictable complication of HCM. The overall related annual mortality rate ranges from less than 1% in asymptomatic patients to 6% in patients with high-risk factors. Identification of individuals at high risk for sudden cardiac death according to the various manifestations of HCM is a challenge. Some of the MRI findings with potential application for stratification of sudden cardiac death risk in patients with HCM include: 1) Maximal wall thickness of 30 mm or more; 2) Marked left ventricle outflow tract obstruction with gradient of ≥30 mmHg at rest; 3) Left ventricle dilatation and depressed ejection fraction; 4) Perfusion defects; 5) Fibrosis, seen as delayed enhancement in as many as 80% of patients; and 6) Reduced functional reserve flow.
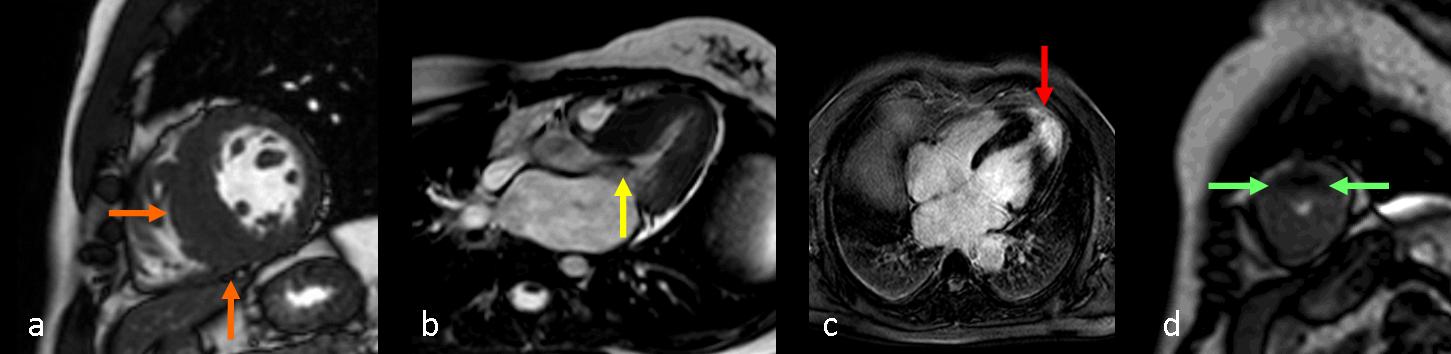
Fig. 5
Figure 5. Images from four patients show the spectrum of risk factors. (a) Short axis cine-MRI depicts septal myocardial enlargement >30 mm (orange arrows). (b) Horizontal long axis cine-MRI shows hypointensity in the left ventricle outflow tract due to turbulent flow because of obstruction (yellow arrow). (b) Delayed contrast enhancement obtained with T1W inversion recovery sequence after Gd-DOTA contrast injection; hyperenhancement is seen in the apex (red arrow). (c) Perfusion defects in anterior apical segment during injection of gadolinium chelates (green arrows).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Hypertrophic cardiomyopathy (HCM) is a genetic disease and the most common cause of sudden cardiac death in young people.
- Signal intensity, motility, and perfusion are useful to differentiate mass-like hypertrophy from myocardial masses.
- HCM phenotypes and risk status are assessed with MRI
Suggested reading:
- Hypertrophic cardiomyopathy: assessment with MR imaging and multidetector CT. Radiographics. 2010 Sep;30(5):1309-28.
- Clinical utility of cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Cardiovasc Magn Reson. 2012 Feb 1;14:13. Review.
Case prepared by Rafaela Soler MD


Hypertrophic cardiomyopathy
i believe it is likely to be a case of rhabdomyoma because leiomyosarcoma would be more heterogenous and hypertrophic cardiomyopathy would cause more diffuse thickening of the wall and would definetely affect the ventricle septum .
Non ho esperienza di Cardio-RM. Comunque, l’ispessimento di parete è localizzato, non interessando tutta la parete ventricvolare;esso inoltre è omogeneo nella sua intensità di segnale.Il soggetto è giovane: se ci sono gli altri segni della
Sclerosi tuberosa di B., la diagnosi dovrebbe essere di rabdomioma.
One of the good things of these presentations is that you are exposed to new knowledge. Myself, I am learning with every case.
I also dont have any experience with cardioMRI, anyway I tried to get an idea a with the last case about it (cardiac amiloidosis) and reviewing the literature I got I would bet for asimetric septal hypertrophic cardiomyopathy.
This is another plus of the cases: forces you to investigate on your own and learn.
hypertrophic cardiomyopathy
Grazie per il bel caso:ignoravo le forme focali di HCM e le possibilità della RM di stratificare il rischio di morte improvvisa( specie nello sport).PS : consolate il “galactico” professore per il suo Barcellona a Milano!
Thank you for the consolation. Hope someday Barcelona plays Bari.