Dr. Pepe’s Diploma Casebook: Case 27 – SOLVED
Dear Friends,
This week we have the case of a 45-year-old man, who is an alcoholic with abdominal pain, jaundice, and weight loss.
Possible diagnoses:
1. Duodenal neoplasm
2. Focal pancreatitis of pancreatic head
3. Pancreatic neoplasm
4. None of the above


Fig. 1
CT findings: Consecutive craniocaudal contrast-enhanced images show a sheet-like, hypodense, poorly enhancing mass between the head of the pancreas and the duodenum (green arrows in b-d). A normal homogeneously enhanced pancreatic head with fuzzy peripheral borders is seen (red arrows in b-d). There is slight dilation of the gall bladder and intrahepatic biliary tree (yellow arrow in a).
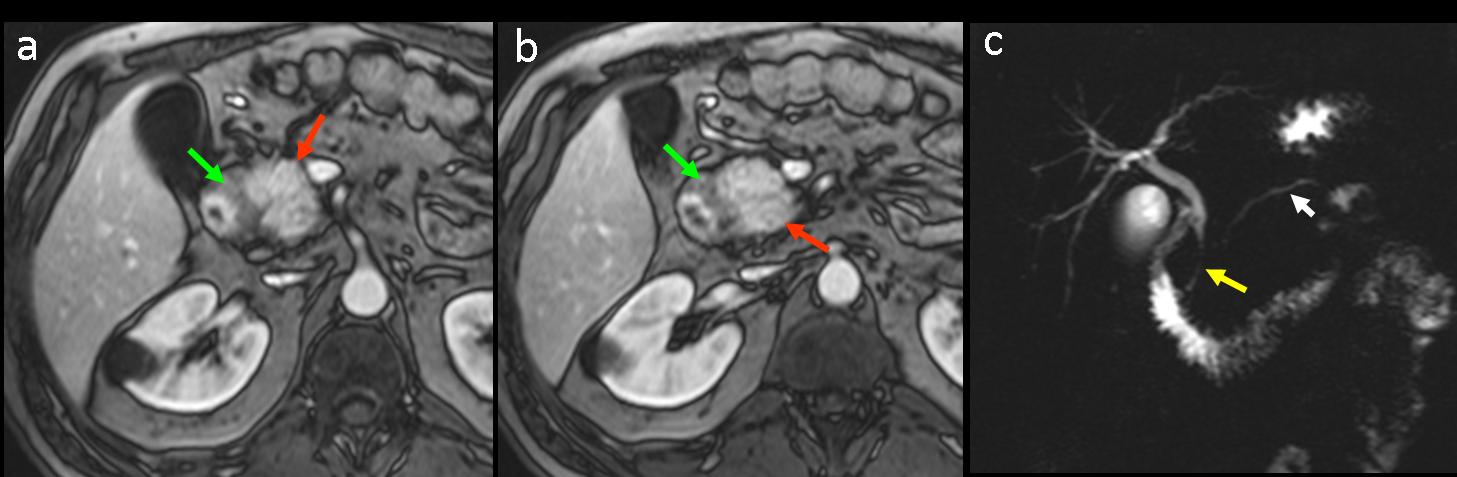
Fig. 2
MR findings: (Fig. 2 a,b) Gd-enhanced T1W images confirm the hypointense plate-like mass occupying the space between the pancreatic head and duodenum (green arrows).The parenchyma of the pancreatic head is spared, and shows normal homogeneous contrast enhancement (red arrows). (Fig 2c) MR cholangiopancreatography shows smooth stenosis of distal common bile duct (yellow arrow) with slight dilation of the intrahepatic biliary tree and pacreatic duct (white arrowhead).
Fig. 3: schematic drawing of groove pancreatitis, depicting fibrotic tissue in the pancreaticoduodenal groove (blue arrows).

Fig. 3
Final diagnosis: pure form of groove pancreatitis
Groove pancreatitis (GP) refers to a distinct form of chronic pancreatitis characterized by inflammation and fibrous tissue formation affecting the groove area between the head of the pancreas, the duodenum, and the common bile duct (CBD). Two forms of the disease are recognized, the pure form and the segmental form. The pure form affects the groove only, while the pancreatic parenchyma is preserved. The segmental form extends to the pancreatic head, despite a clear predominance in the groove.
In pure GP, a poorly hypodense plate- or sheet-like mass is seen between the pancreatic head and the duodenum on contrast-enhanced CT examinations. In MR imaging studies, a hypointense plate-like mass is visible in the groove region in both unenhanced and enhanced T1W images.
The differential diagnosis of GP includes duodenal and pancreatic cancer, CBD cancer, and acute pancreatitis with phlegmon along the groove. The most relevant differential diagnosis (particularly in the segmental form) is adenocarcinoma of the head of the pancreas. MR imaging studies can be helpful, showing the spared pancreatic parenchyma in the pure form of the disease. MR cholangiopancreatography sequences can help to differentiate GP from pancreatic cancer: GP shows long, smooth segmental CBD stenosis, whereas in pancreatic or CBD neoplasms, the stenosis has an abrupt aspect.
MR studies may also be useful in patients with pancreaticoduodenal lesions in whom the CT findings are inconclusive.
In conclusion, GP is an interesting, uncommon pancreatic disease with a challenging imaging diagnosis, and should be included in the differential diagnosis of pancreaticoduodenal lesions with signs of duodenal/periduodenal infiltration.
The differential diagnosis of GP includes other conditions affecting the pancreaticoduodenal area, such as pancreatic neoplasm (Fig. 4) and duodenal neoplasm (Fig. 5), in which the imaging features may be difficult to differentiate from those of GP.
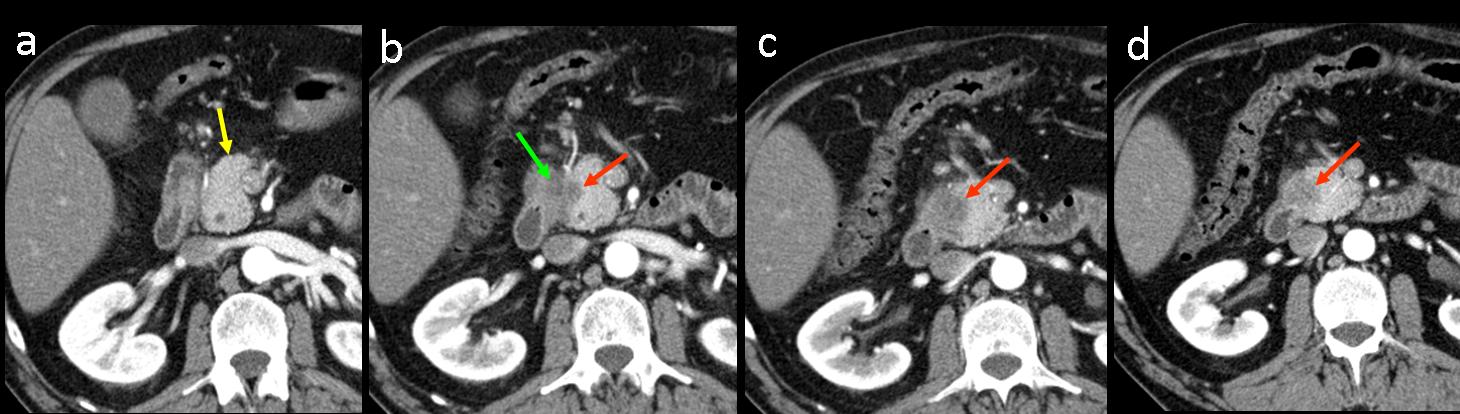
Fig. 4
Four contiguous, craniocaudal, contrast-enhanced dynamic CT images in a single patient with neoplasm of the pancreatic head. (a) In the first image, the pancreatic head is normal and no lesions are seen (yellow arrow). (b-d) Moderately well-delineated rounded hypodense lesion of the pancreatic head was confirmed to be pancreatic adenocarcinoma at surgery (red arrows). The tumour was occupying the pancreaticoduodenal area and invading the duodenal wall (green arrow).
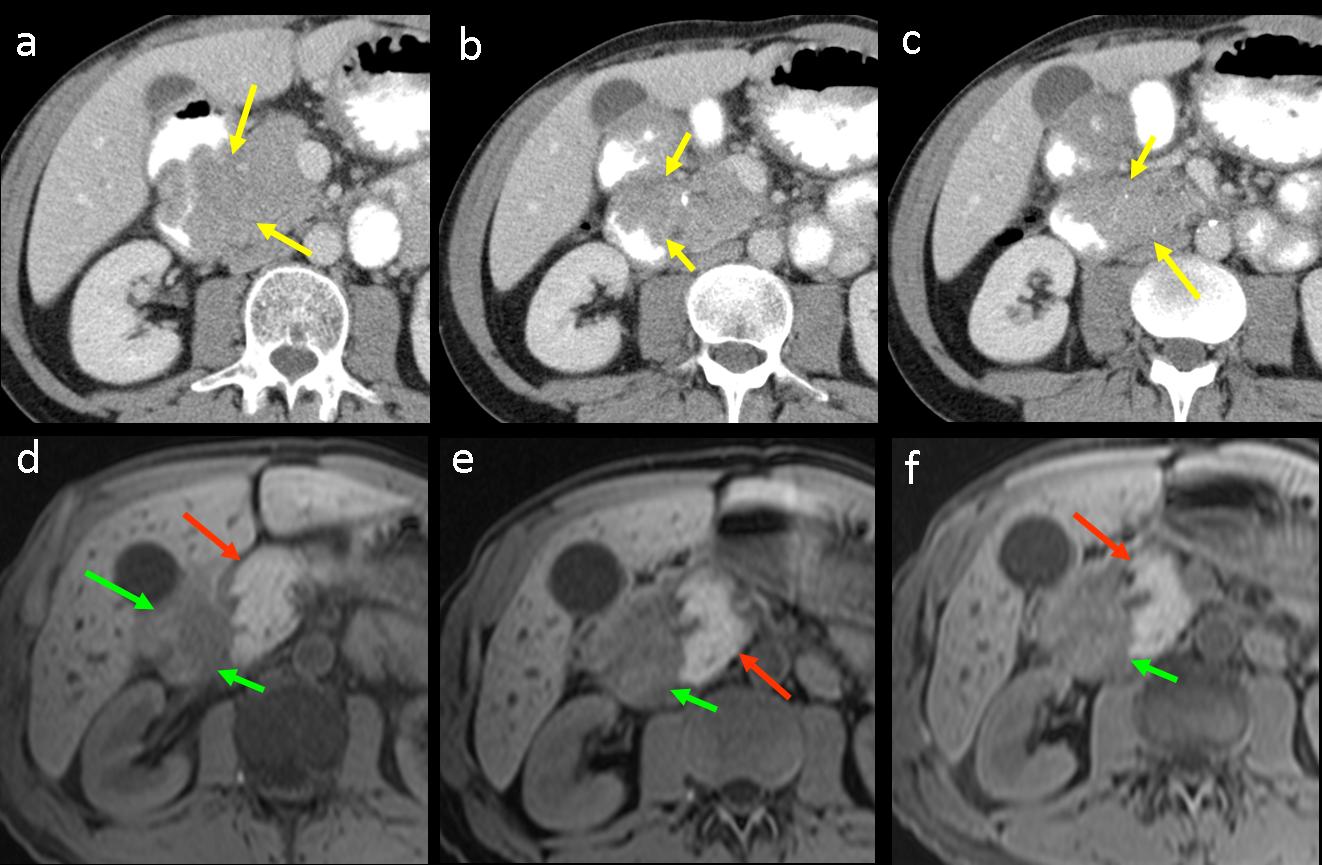
Fig. 5
Soft-tissue mass in the pancreaticoduodenal region in a patient with duodenal cancer. (a-c) Consecutive, enhanced CT images show a solid mass in pancreaticoduodenal area (yellow arrows). It is difficult to know whether the lesion is a primary pancreatic neoplasm invading the duodenum or a primary duodenal tumor affecting the pancreas. (d-f) Consecutive craniocaudal images on unhenhanced fat-suppressed T1W MR imaging confirm that the lesion only affects the duodenum (green arrows), whereas the pancreatic head is spared and shows normal, hyperintense signal intensity (red arrows).

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- GP is an interesting, uncommon pancreatic disease with a challenging imaging diagnosis that should be included in the differential diagnosis of pancreaticoduodenal masses.
- On CT images, the diagnosis of GP should be suspected when hypodense tissue is occupying the space between the duodenal wall and head of the pancreas in a clinical scenario similar to that of chronic pancreatitis.
- MR imaging may be helpful for diagnosing GP, showing the fibrotic tissue in the groove area, sparing of the parenchyma of the pancreatic head, and depicting a smooth narrowing of the distal CBD on cholangiopancreatography pulse sequences.
Recommended reading
Triantopoulou C et al. Groove pancreatitis: a diagnostic challenge. Eur Radiol 2009 ; 19 : 1736-1743
Blasbalg R el at. MRI Features of Groove Pancreatitis. AJR 2007; 189; 73-80
Case prepared by Julio Martin MD


pancreatic neoplasm
Pancreatic head enlarged.
Edema around pancreatic head and adjacent duodenum.
No ductal dilatation.
2. Focal pancreatitis of pancreatic head
4. None. Groove pancreatitis.
Groove pancreatitis
why not a groove pancreatitis?
Groove pancreatitis is a good option. There’s no expansive lesion and there is densification in duodenalpancreatiatic sulcus.
My vote for a focal pancreatitis
?focal panceriatitis
focal pancreatitis
focal pancreatitis maybe
Duodenal neoplasm
Focal pancreatitis of pancreatic head
I’d say groove pancreatitis.
2.
doudenal neoplasm