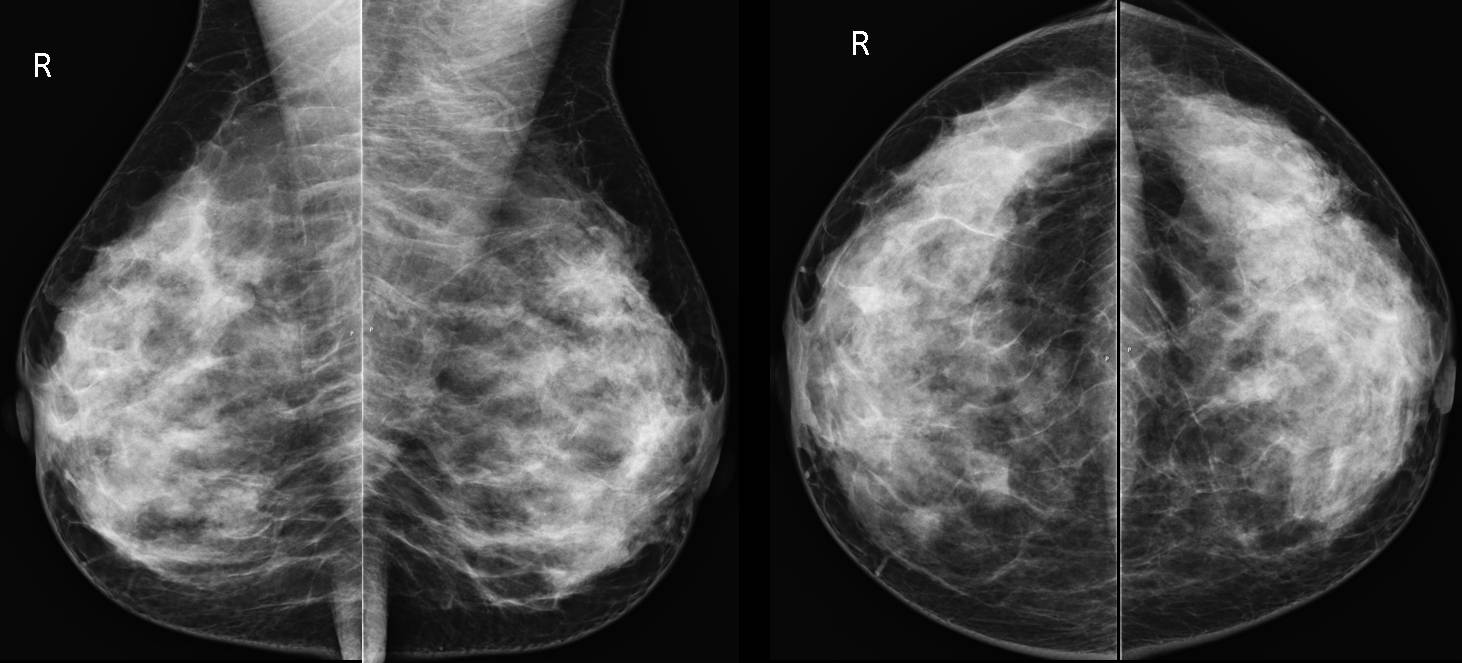
This week I’m showing screening mammograms of a 39-year-old woman in whom an abnormality was found.
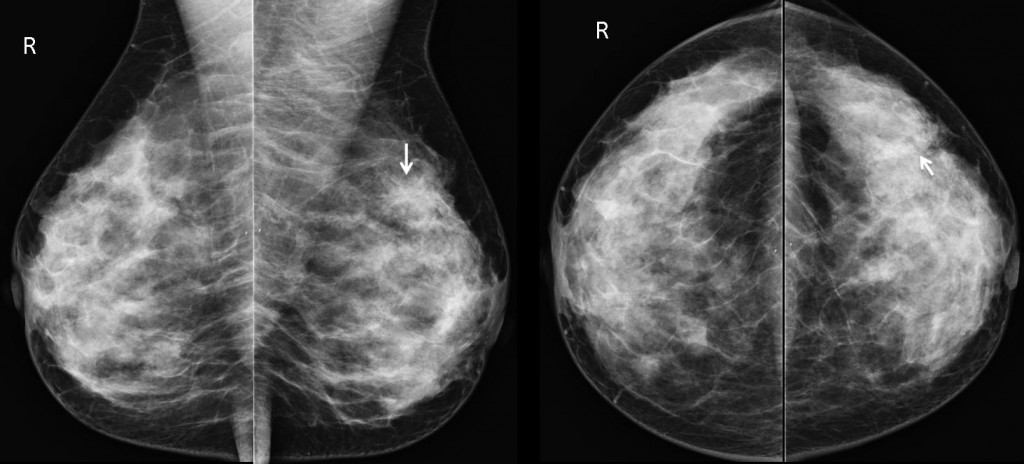
Fig. 1
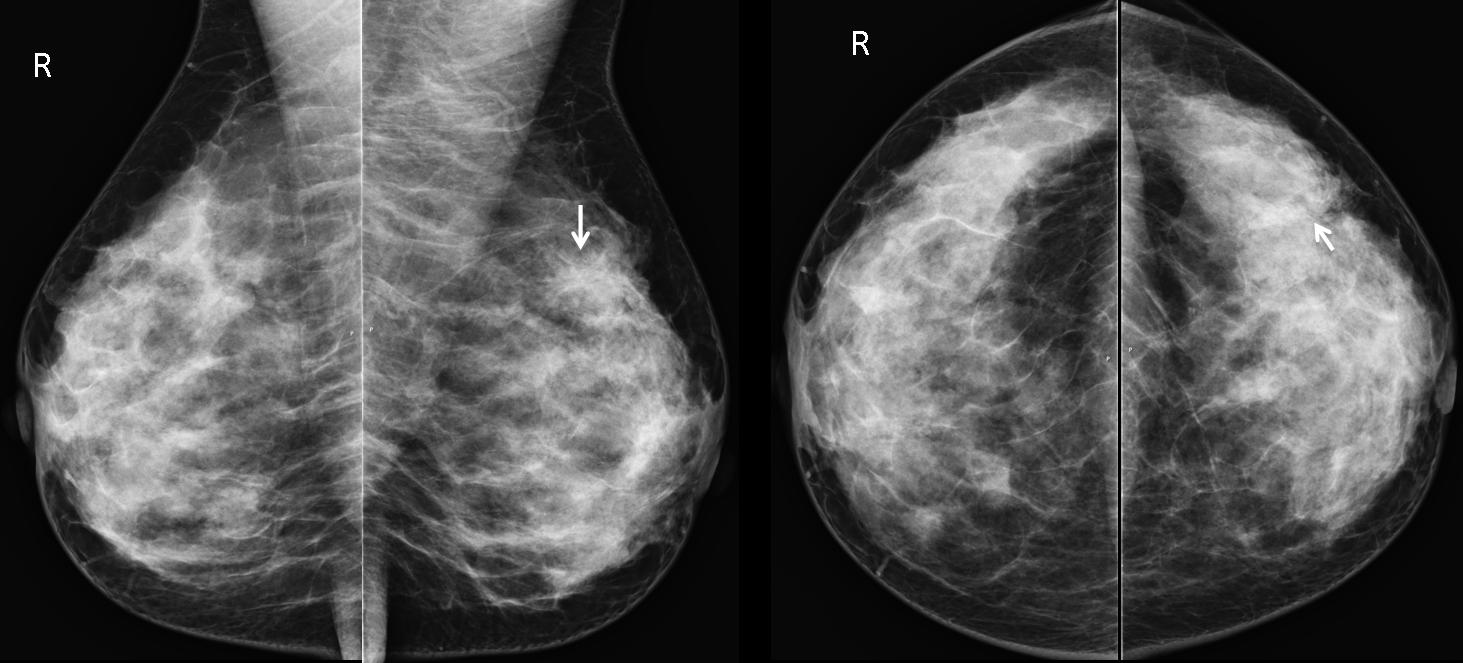
Findings: There is a spiculated lesion in the upper quadrant of left breast in the mediolateral view (arrow), poorly seen in the external quadrant in the craniocaudal view (arrow).
A spiculated lesion is one of the most significant findings in mammography. In most cases by far, it correspondes to carcinoma, but this is not the only possibility. A postoperative scar can have the same appearance. Other less common spiculated lesions are radial scar and sclerosing adenosis, among others. Because the finding of a spiculated lesion is not specific, the best option is all of the above.
Because of the suspicious appearance of the image in this case (BIRADS 4), core needle biopsy was performed, which yielded material consistent with radial scar. The diagnosis was confirmed at surgery.
Final diagnosis: radial scar
Radial scar is an idiopathic lesion characterized by a sclerotic center surrounded by ducts containing epithelial hyperplasia radiating from the center. The mammographic appearance is that of a spiculated lesion, which is not usually palpable.
The echographic features are very similar to those of carcinoma. For that reason, all such lesions require biopsy and, if confirmed, subsequent surgical removal to exclude the possibility of an underlying carcinoma, which may be associated.
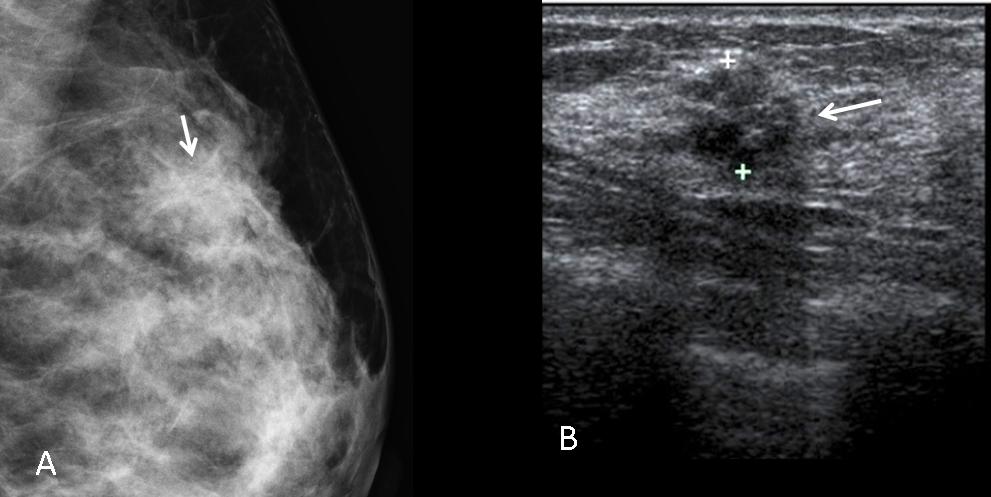
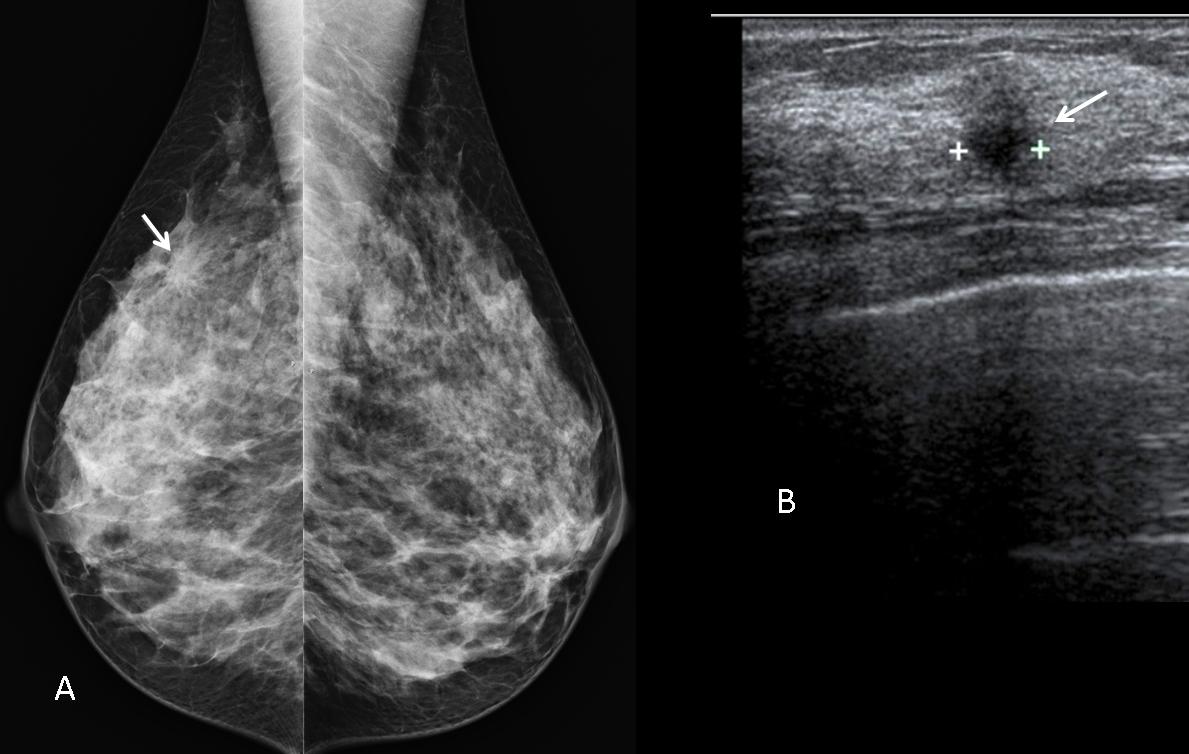
Fig. 2
Fig. 2 (above): imaging findings in radial scar. Spiculated lesion in the mammogram (A, arrow). The lesion is hypoechoic (B, arrow), with poor sound transmission.
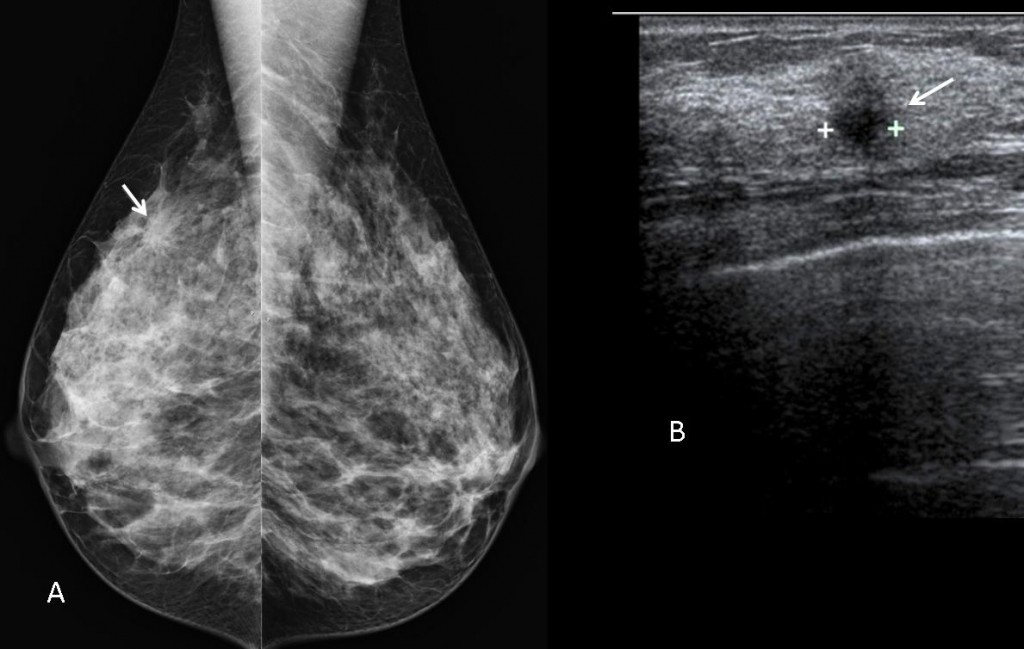
Fig. 3
Fig. 3 (above): carcinoma of the breast is the most common cause of lesions with a spiculated appearance (A, arrow), which is due to peripheral infiltration or accompanying desmoplastic reaction. The sonographic pattern is that of an irregular hypoechoic mass with diminished sound transmission (B, arrow). This combination of findings is an indication for immediate biopsy.
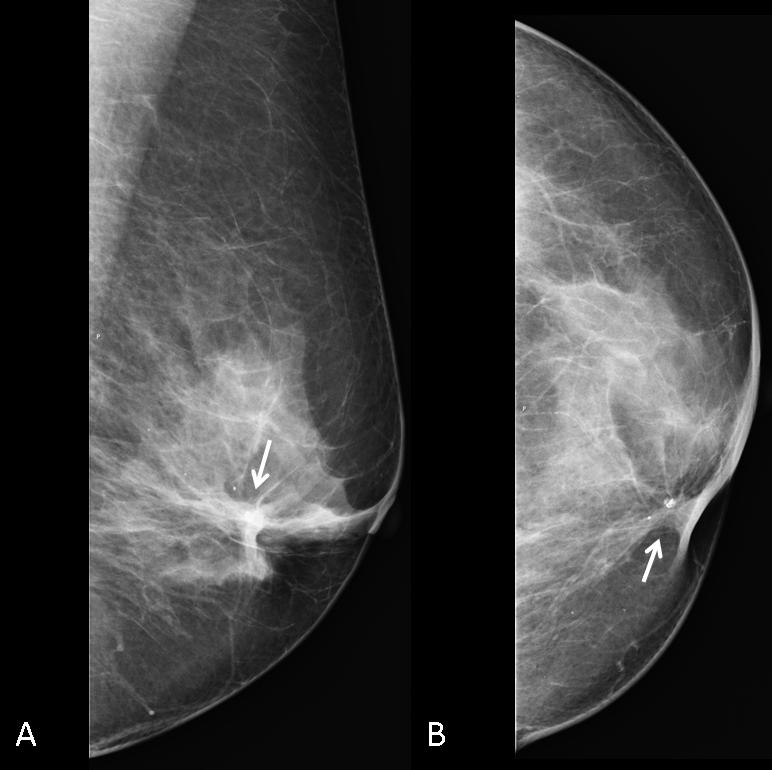
Fig. 4
Fig. 4 (above): Postsurgical scars are fibrotic lesions that give a spiculated appearance in the mammogram (A,B arrows). In the follow-up of operated neoplasms, it is important to compare carefully with previous examinations to detect possible recurrence. If one is suspected, ultrasound is not helpful, as the scar produces extensive shadowing. MRI is the examination of choice, followed by biopsy, if indicated.

Follow Dr. Pepe’s advice:
- Various spiculated lesions of the breast have similar imaging features at mammography and need core biopsy to reach a definite diagnosis.
- US cannot differentiate between carcinoma and radial scar.
- When recurrence is suspected in postoperative scars, MRI is the examination of choice.
Recommended reading: Spiculated lesions of the breast: mammographic-pathologic correlation. RadioGraphics 13:841-852, 1993
DB Kopans. Beast Imaging 2nd edition, page 302
Case prepared by Elena Rabanal MD


Radial scar in upper aouter quadrant
In the upper-outer quadrant of the left breast there is a stellate lesion which is better seen in MLO view. In CC view the lesion would not be easily discernible if it didn’t produce a “tent sign”. The stellate lesion has no dark center and the spiculations are short(option 1 is ruled out). There is no skin thickening or suspicious microcalcifications. There are no enlarged lymphnodes in the left axilla.
I choose 2.carcinoma
i agree with katerina plus we have asymmetry in the central – internal quadrant in CC view in the R breast.
we need compress view first und U/S in both lesions.
mine first choose is 1.carcinoma but if i am wrong with the second lesion could be 4. All of the above
Until proven otherwise: carcinoma.
I have same comment as Katerina, diagnosis 2carcinoma
In the upper-outer quadrant of the left breast there is a stellate lesion which is better seen in MLO view. In CC view the lesion would not be easily discernible if it didn’t produce a “tent sign”. The stellate lesion has no dark center and the spiculations are short(option 1 is ruled out). There is no skin thickening or suspicious microcalcifications. There are no enlarged lymphnodes in the left axilla.
Non ho esperienza in senologia; tuttavia alcune considerazioni vanno fatte. Perchè uno “screening” mammografico già a 39 anni? C’è familiarità genetica per Cr: BR-CR1-BR-CR2? L’anamnesi è postiva per un precedente chirurgico,es. fibro-adenoma? la DD tra un radial-scar e un Cr si potrebbe fare con una RM con mdc paramagnetico, prima di un prelievo cito-istologico su guida US?L’esame clinico, parte “integrante” di una visita senologica, cosa ha trovato?
Clinical examination negative. No palpable lesion
Distorsione dell’architettura ghiandolare: approfondimento! 1’ecografia. 2′ RM. 3’Biopsia.
caro dott.Pepe ed io cosa avevo detto circa l’RM con mdc come gold-standard per la diagnosi?
Once malignancy is suspected, core biopsy is much more accurate than MRI
…di fronte al maestro…”chapeau”!