Dr. Pepe’s Diploma Casebook: Case 52 – SOLVED!
Dear Friends,
Today I am presenting radiographs of a 43-year-old woman with moderate dyspnoea. Disregard the widening of the right superior mediastinum, secondary to long-standing goiter. Leave me your thoughts and diagnosis in the comments sectiona and come back on Friday for the answer.
Diagnosis:
1. Thymoma
2. Heart disease
3. Lymphoma
4. None of the above
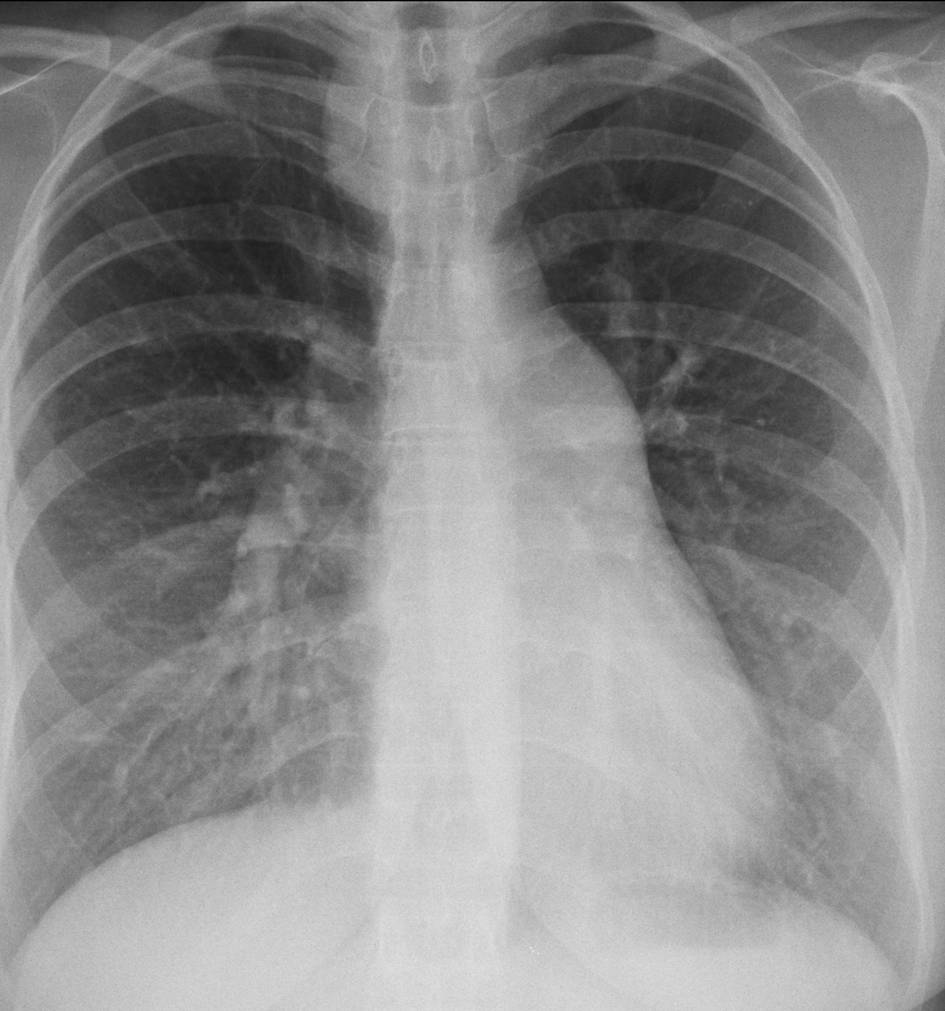
43-year-old woman with moderate dyspnoea
Findings: PA chest film shows bulging of the main pulmonary artery contour (A, arrow), accompanied by moderately increased arterial circulation of the lungs (note increased diameter of vessels in both lower lobes and left upper lobe). This combination of findings suggests a left-to-right shunt. MRI shows communication (B, arrow) between the right atrium (RA) and the left (LA).

Fig. 1
Final diagnosis: septum secundum atrial septal defect with left-to-right shunt
This case is presented to discuss prominence of the pulmonary arch. The mediastinum has three bumps on the left contour: the uppermost is the aortic knob (A, arrow). The second corresponds to the main pulmonary artery (A, red arrow) and the third represents the left ventricle (A, yellow arrow). There is a virtual bulge between the second and the third arch which, when present, represents the atrial appendage in mitral disease (B, arrow).
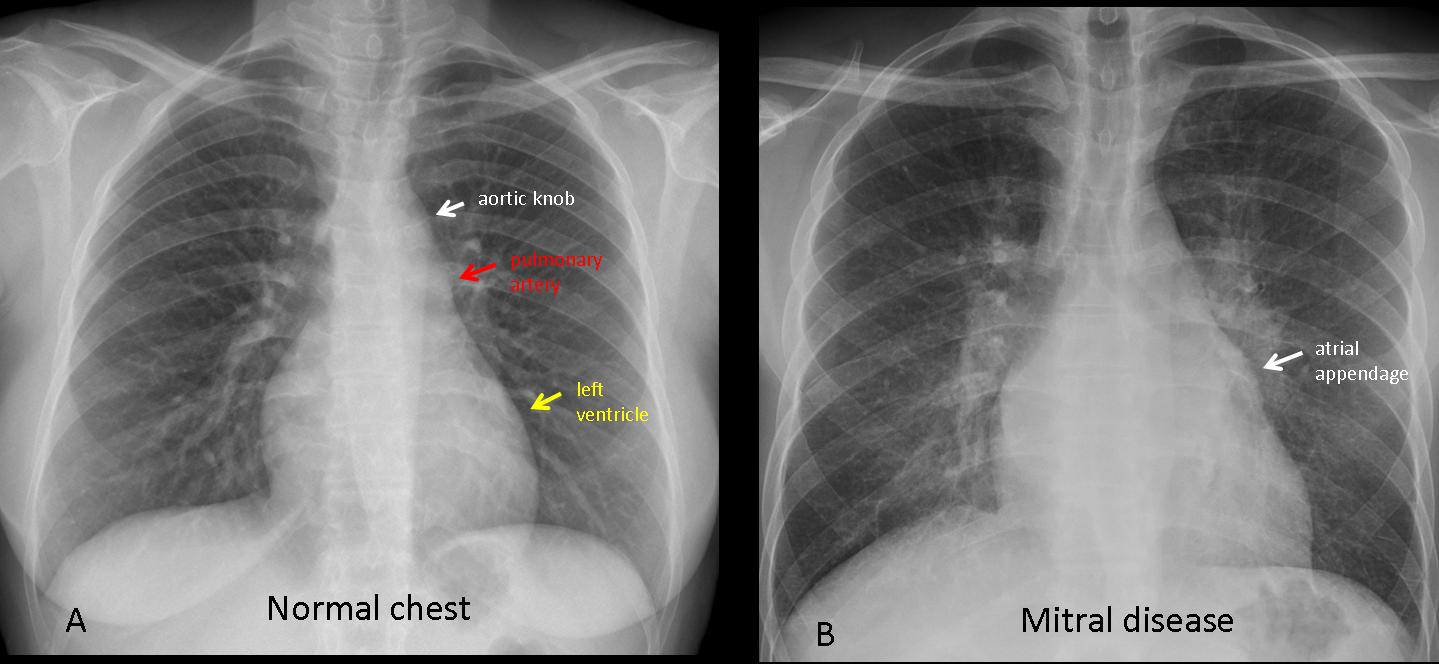
Fig. 2
Bulging of the pulmonary arch usually indicates dilatation of the main pulmonary artery. Three conditions cause dilatation of the artery. The most common is pulmonary arterial hypertension, followed by left-to-right shunt and pulmonary valve stenosis. These conditions can be suspected on chest radiographs if one knows their imaging manifestations.
Pulmonary arterial hypertension (PAH) is not uncommon in daily practice. In the chest plain film, PAH is recognized by a prominent pulmonary arch (A, white arrow) with enlargement of the central pulmonary arteries, visible in the PA and lateral views (A,B, red arrows), accompanied by abrupt tapering of the peripheral pulmonary vessels.
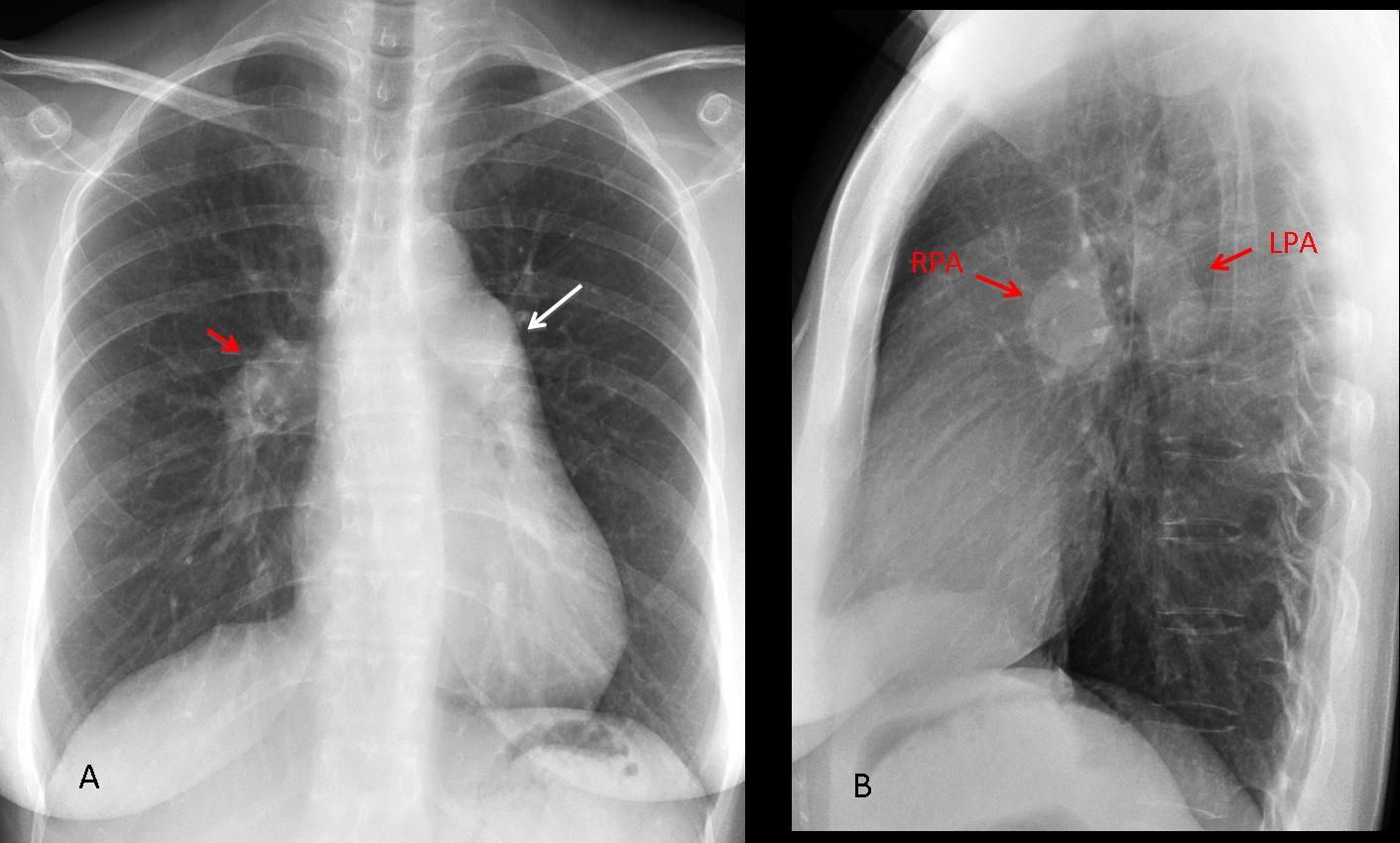
Fig. 3
Axial and coronal CT images show marked enlargement of the central pulmonary arteries (A, arrows), with tapering of the peripheral vessels. The CT criterion for diagnosing PAH is main pulmonary artery diameter greater than or equal to 29mm (B, arrow).

Fig. 4
The etiology of PAH is varied. The most frequent cause is chronic pulmonary disease (mainly COPD). Other causes include obstruction of vessels (chronic pulmonary embolism), inverted left-to-right shunt (Eisenmenger syndrome), and idiopathic PAH, which occurs in young adults and more commonly affects women.
All cases of PAH show similar imaging findings on plain films, regardless of the cause. The following signs may suggest the etiology: evidence of pulmonary disease (COPD or others) (Fig. 5) or scars and blunting of the costophrenic angles, suggestive of previous pulmonary emboli. In advanced cases, CT may show calcification of pulmonary artery walls, a sign of long-standing PAH (Fig. 6).
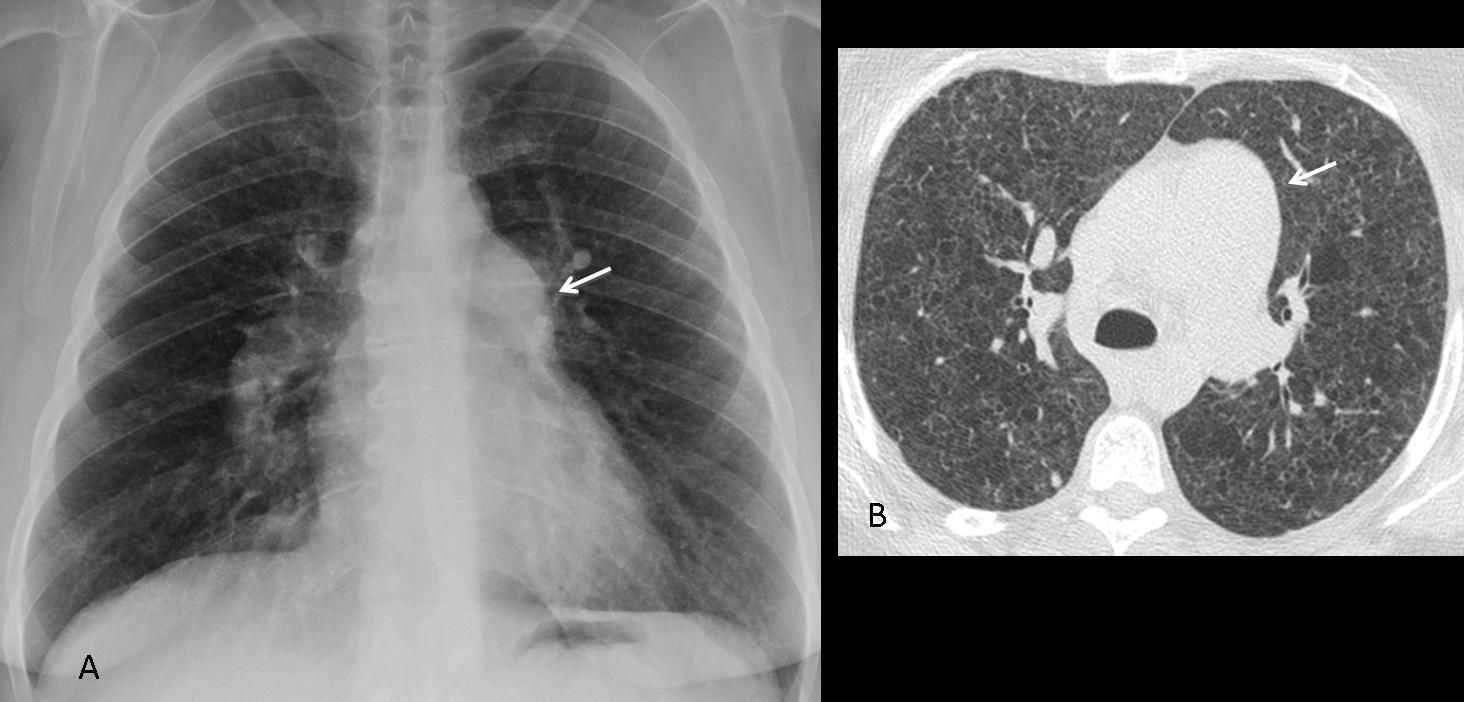
Fig. 5
Fig. 5 (above): 44-year-old woman with Langerhans cell histiocytosis. PA chest film shows the typical signs of PAH: a prominent pulmonary arch (A, arrow) and enlarged hila with tapering vessels. Axial CT shows diffuse lung disease and a markedly enlarged pulmonary artery (B, arrow).
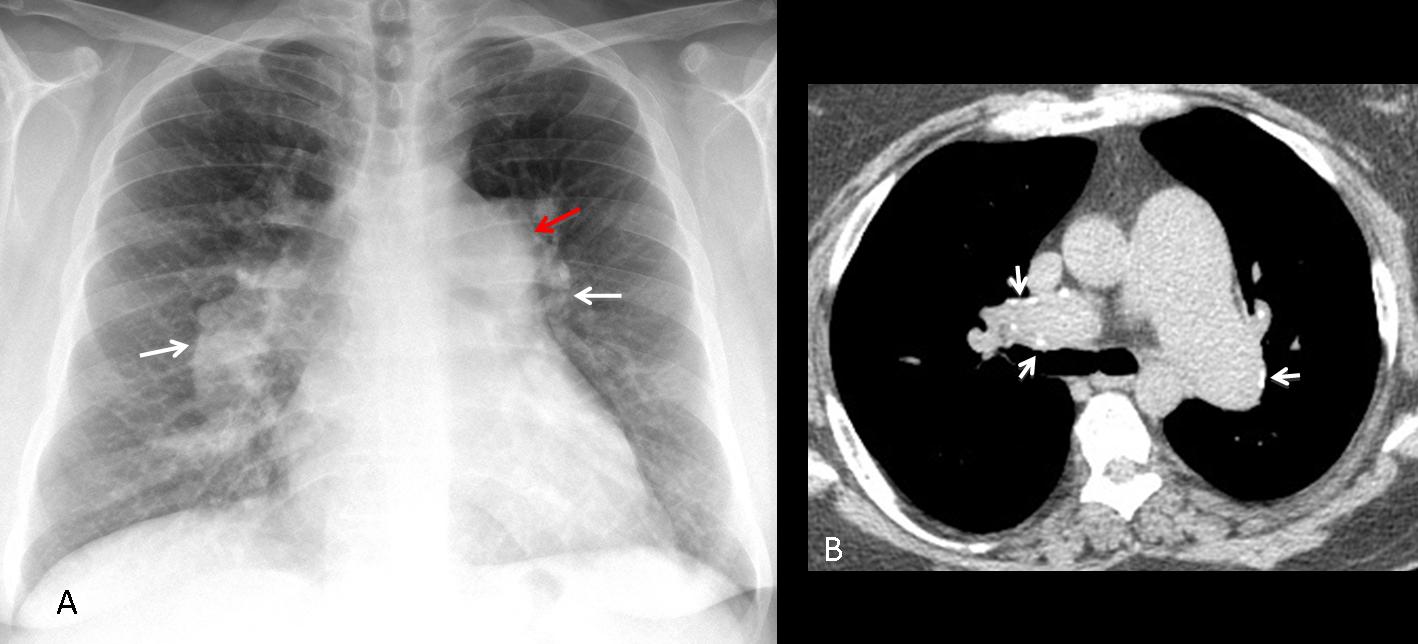
Fig. 6
Fig. 6 (above): 45-year-old man with long-standing idiopathic PAH. PA chest film depicts prominent hila (A, white arrows) with abrupt tapering of distal arteries and bulging of the pulmonary arch (A, red arrow). CT shows the marked size disparity between the aorta and pulmonary arteries, which have calcified walls (B, arrows).
Isolated left-to-right shunts are another cause of a prominent pulmonary arch. They may occur at the level of the atria, ventricles, or through a persistent ductus arteriosus. The last two are usually discovered in infancy, whereas atrial septal defect may go into adulthood without significant symptoms and be discovered in a routine chest examination. Suggestive signs of shunts are a prominent pulmonary artery and increased arterial circulation in both lungs (Fig. 7). The heart is usually enlarged.
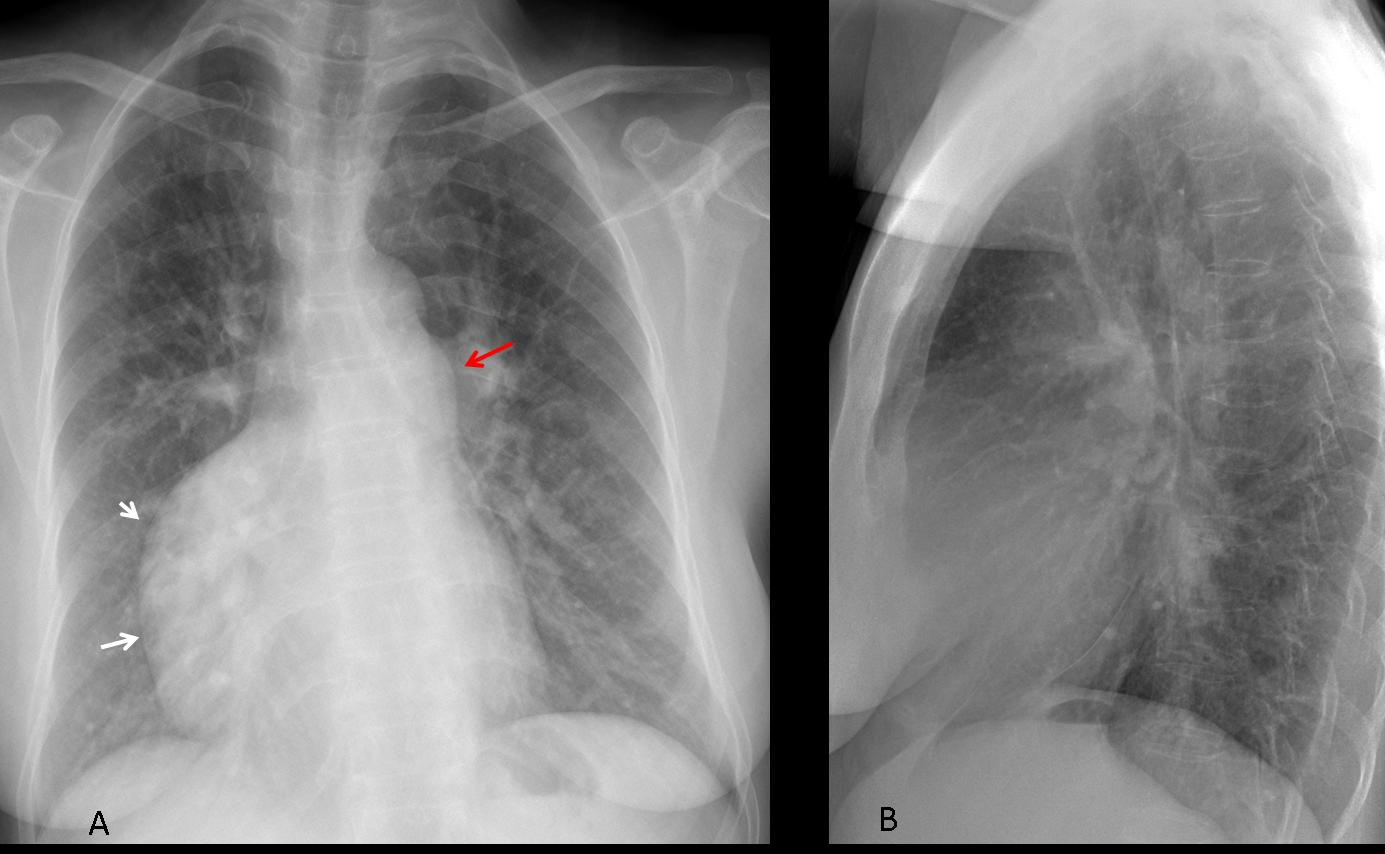
Fig. 7
Fig 7 (above): 47-year-old female with ASD. Note the markedly enlarged right atrium (A, arrows) secondary to circulation overload. The pulmonary arch is prominent (A, red arrow) and the pulmonary arterial circulation is increased. Diagnosis: septum secundum atrial septal defect.
The third cause of enlarged central pulmonary artery is congenital pulmonary valve stenosis. In this condition, the jet of blood caused by the stenosis leads to dilatation of the main and left pulmonary arteries. The pulmonary vasculature is either normal or decreased (Fig. 8). Patients are usually asymptomatic and the abnormality is discovered in the 3rd or 4th decade.
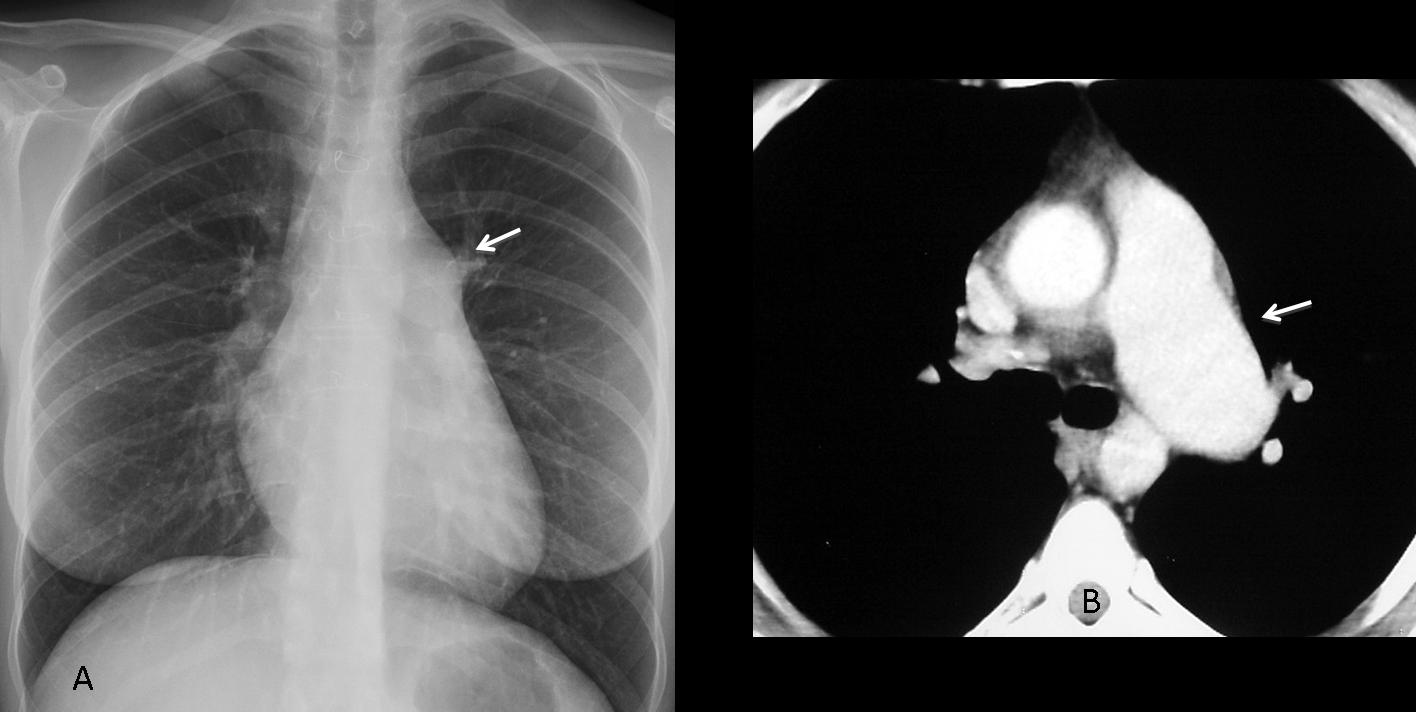
Fig. 8
Fig. 8 (above): 34-year-old female with pulmonary valve stenosis. PA chest film shows a prominent pulmonary arch (A, arrow) and decreased circulation in both lungs. Axial CT confirms the dilatation of the main and left pulmonary arteries (B, arrow).
To summarize: the imaging findings accompanying dilatation of the pulmonary arch are:
- Enlarged hila and abrupt tapering of pulmonary arterial circulation: Pulmonary arterial hypertension (A)
- Enlarged hila and increased circulation of lungs: Isolated left-to-right shunt (B)
- Normal or decreased pulmonary circulation: Pulmonary valve stenosis (C)
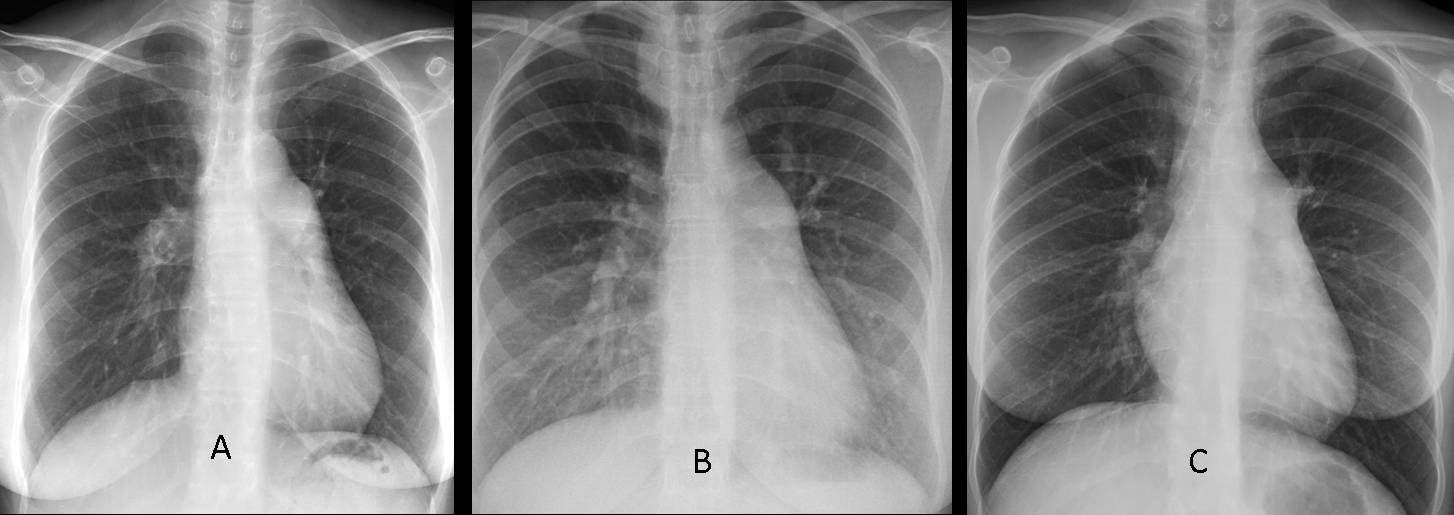
Fig. 9
A less common cause of prominent pulmonary arch is an anterior mediastinal mass superimposed on the pulmonary segment. In these cases, the hila and pulmonary vessels are unremarkable and the lateral view may show the mass in the anterior clear space (Fig. 10)
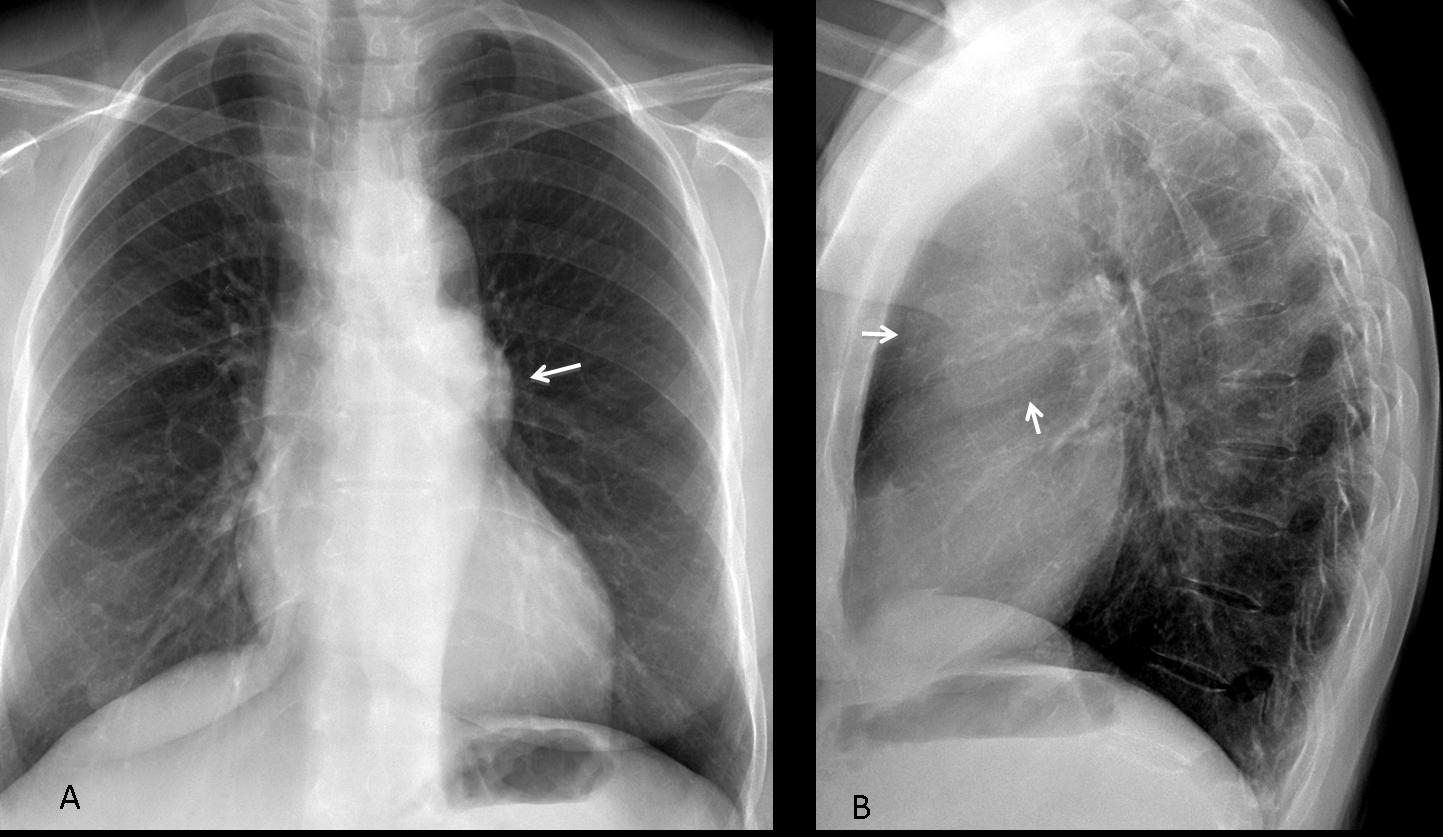
Fig. 10
Fig. 10 (above): Preoperative chest radiograph in a 45-year-old woman showing a prominent pulmonary arch (A, arrow). Hila and pulmonary vessels are normal. Lateral chest film depicts a large mass in the anterior clear space (B, arrows).
Unenhanced CT (Fig. 11, below) confirms the presence of a large soft-tissue mass (A,B, arrows) projected over the pulmonary artery arch. Final diagnosis: thymoma.

Fig. 11
Moderate prominence of the pulmonary arch is common in adolescents. It is believed to correspond to thymic tissue and should not be considered an abnormal finding (Fig. 12).
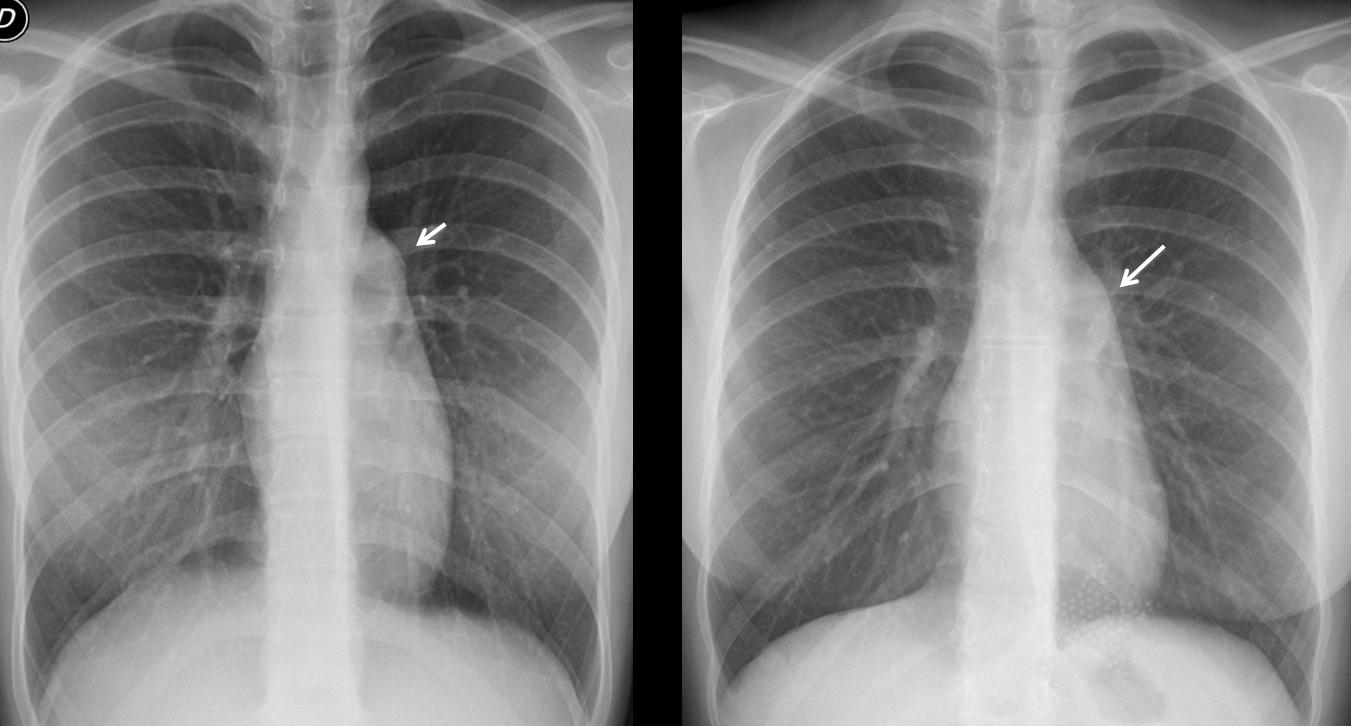
Fig. 12
Fig. 12. PA radiographs of two asymptomatic female teenagers. Both have prominent pulmonary arch (A,B, arrows).

Follow Dr. Pepe’s advice:
- Prominence of the pulmonary arch is abnormal, except in teenagers.
- The most frequent cause is increased size of the main pulmonary artery due to PAH, left-to right-shunt, or pulmonary valve stenosis
- Anterior mediastinal masses may simulate increased size of the pulmonary arch. Look at the anterior clear space in the lateral view.


Dear Profesor Caceres and Dr Pepe,
perhaps this is my last post before EDIR
In this erect pa chest xray is:
– markedly seen vascular pattern in lower and partially medial pulmonary fields bilateral
– bilater cephalisation of vascular pattern in upper fields
-less vascular pattern on the peripherial parts of the lungs
-the right pulmonary artery look enlarge, i think more then 16 mm
– the left vascular hilum is impossible do diagnose
-the upper right mediastinum is enlarged unilateral;sail sign?thymoma?
– marked left round shadow of the left middle mediastinum.
-CH ratio looks ok
-no bone destruction
-no metal parts which can suggest an surgical intervention
ddx:
– pulmonic stenosis ( with or without asd )
– pulmonary artery hypertension
– mediastinal mass – sail sign ? thymoma ( there is no calcification, no marked tracheal shifting ) or thyroid goiter.
Good luck! When meeting the examiners, tell them that you are a friend of Dr. Pepe.
thank you!!!!! i ll do for sure.
i have learned a lot immersing my self in all cases !
any tip for diagnosis of this patient.
Too early for tips. Besides, you have to concentrate in your examination.
Agree a lot with the you dear.
But it looks like pulmonary venous hypertension with loss of pulmonary bay- D/D MS and other causes of pulmonary venous hypertension.
Dr Pepe…I miss the lateral view…may you show it to us?
Still!
I observe a mediastinal widening, with bulging of the aortic line, so there is not a aortopulmonary window. Edges are smoth. The hila and the cardiotoracic silhouette seems not pathological to me. Parenchima also looks normal. So, as we wait for the lateral rx, I’d think of vascular disease( aortic aneurisma…), but by now, thymoma or lymphoma cannot be discharted, so I guess I need more tips, then…
Sorry, no lateral view was taken.
But I suggested the diagnosis with the PA…
enlarged left pulmonary artery
….carissimo dr Pepe….iniziamo con la clinica:dispnea….è di origine cardiaca(= disturbo di circolazione del piccolo circolo) oppure è di origine tracheo-bronchio-respiratoria?…i polmoni sono normo-espansi e normo-perfusi, per cui penso di escludere la causa cardiaca….rimane la seconda ipotesi….la “silhouette” vascolare del mediastino è alterata, lasciando pensare che è quella la causa….l’ilo di dx, vascolare , è normale….rimane l’ilo vascolare di sx che non è valutabile….conclusione “anello vascolare” dato dalla “anomala origine dell’arteria polmonare di sx,con compressione tracheo-bronchiale….vedremo la TC con le varie ricostruzioni…..NB. il mio Bari è fallito ,si va ora in tribunale per la vendita del titolo…..siete interessati?
Sorry, not smart enough to be rich and buy Bari. Do you really think that the pulmonary vasculature is normal?
…allora hai fatto pretattica per “confondere” le idee all’avversario….Scarsa definizione del profilo cardiaco di dx, con ombra cardiaca “scivolata” a sx…..prominenza del cono della polmonare….”strano orientamento delle coste….HAI NASCOSTO la LL, perché la diagnosi sarebbe stata così facile…Straight back Syndrome…..
Right heart border not visualised. Posterior ribs more horizontal & anterior ribs more vertical.Possible diagnosis – Pectus excavatum..
Need ur wishes & last minute tips for the exam!! 😛
My best wishes and lots of luck!
Frontal chest radiograph reveals prominent pulmonary conus (convex margin) with dilated central pulmonary arteries and peripheral pruning sugggestive of pulmonary arterial hypertension.Also there is suggestion of right ventricular contour of apex s/o right ventricular hypertrophy. However , cardiac size is normal.
There is no focal lung parenchymal lesion.
Bilateral CP angles are clear.
There is widening of right superior medastinum with convex lobulated outline. But as suggested by you to ignore it as it is due to long standing goitre.
I disagree about the peripheral pruning. Look at the vessels of the right lower lobe
Dear Dr.,
I can add two things to other answers.
1/ Widening of rt.sup.mediastinum which seems not related to the thyroid gland because the trachea is not displaced.(mediastinal mass probabaly related to neural tube)
2/prominence of pulmonary trunk(R/O pulmonary HTN )although straight back syndrome or pigeon chest cant be rulled out.
Trunk of pulmonary artery is prominent with asymetric pulmonary vasculature, right side more prominent than left.
If you you a prominent pulmonary trunk and increased pulmonary vasculature, what do you think of?
pectus excavatum till proved otherwise…..
What I see is left sided aortic arch, prominent pulmonary trunk nad increased vasculature suggesting PDA or in this case a less severe aorto- pulmonary shunt…
Coexistence of most probably thyroid goiter…
Good luck for the Exam-Takers!!!
Good thinking. Congratulations!
Thank You very much… finally scored :]
…..grazie per la bellissima lezione! il caso insegna inoltre la validità della regola KISS….avevo pensato a questa diagnosi, dimenticando questo insegnamento …e fatto una diagnosi molto più difficile e fantasiosa! NB:Spagna-Italia 1 a o…goal di Pepe su assist di Caceres !!!!!!!
Grazie
Agree a lot with most of the previous comments.
However, there is no signs of pulmonary arterial hypertension. This thought of pulmonary arterial hypertension is confusion the issue. The presence of cephalization of the flow and the likely dilated right descending pulmonary artery should suggest pulmonary venous hypertension.
There is also loss of normal pulmonary bay.
But it looks like pulmonary venous hypertension with loss of pulmonary bay- D/D MS and other causes of pulmonary venous hypertension.
Sorry, I disagree with you. The radiologic signs of pulmonary venous hypertension are reversed flow, with grater caliber of upper vessels, compared to the lower ones. The case presented shows the opposite: the lower vessels are much more prominent than the upper ones.
Thanks for replying.
I again carefully looked at the X-Ray-I think I must revise my opinion- you are right in observing that the lower zone vessels are wider then the upper zone vessels- thus my conclusion, that there is cephalization of the pulmonary flow is probably erroneous. So suggesting pulmonary arterial hypertension (due to increased pulmonary artery flow) is prudent. However there is no peripheral prunning.
Thanks for nice case!
Promint pulmonary trunk