Dr. Pepe’s Diploma Casebook: Case 56 – SOLVED!
Dear Friends,
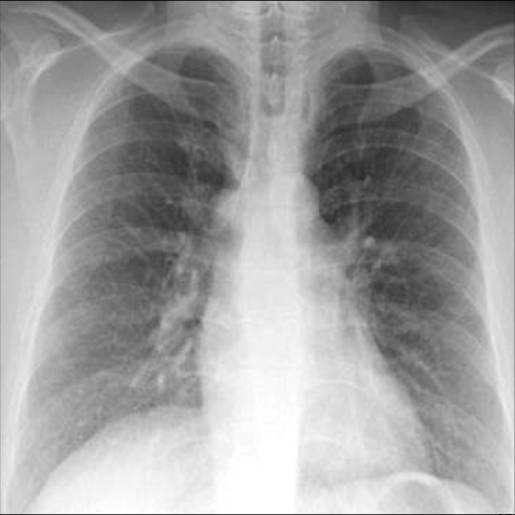
Today I am presenting radiographs of of 41-year-old woman operated on for Ewing sarcoma of T-12 one year ago. Examine the images below, leave me your diagnosis in the comments and come back on Friday for the answer.
Diagnosis:
1. Enlarged azygos vein
2. Mediastinal lymph node
3. Mediastinal mass
4. None of the above

Findings: The main finding is a mediastinal opacity (A, arrow), whose location suggests either an enlarged azygos vein or a lymph node. The lateral view places the opacity behind the trachea (B, arrow) in the location of an enlarged azygos vein; (lymph nodes are located in front of the trachea).
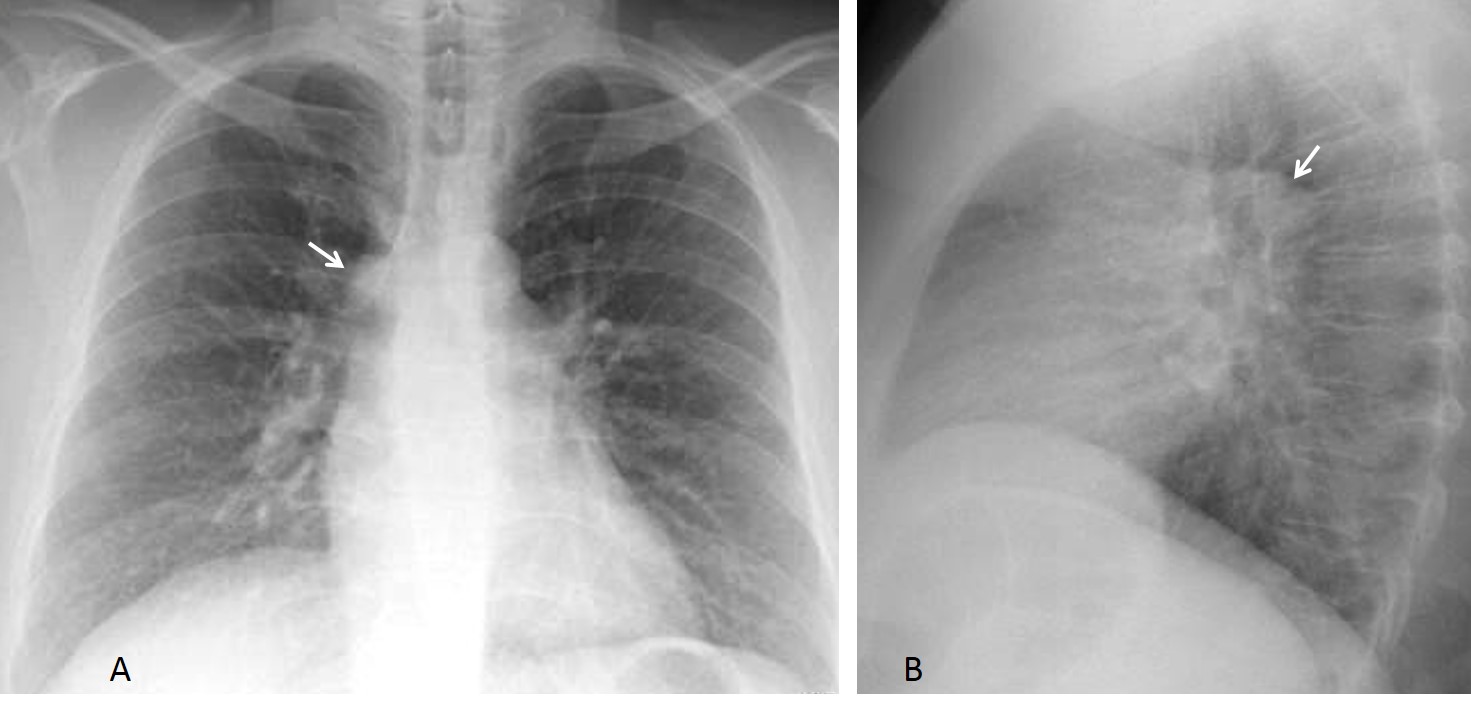
Fig. 1
Axial CT at the level of T-12 shows postoperative vertebral changes and a paravertebral soft tissue mass (C, white arrow), suggestive of tumour recurrence. The azygos vein is enlarged (Fig. 2a, red arrow). A more cephalad slice shows an enlarged and thrombosed azygos arch (2b, arrow).
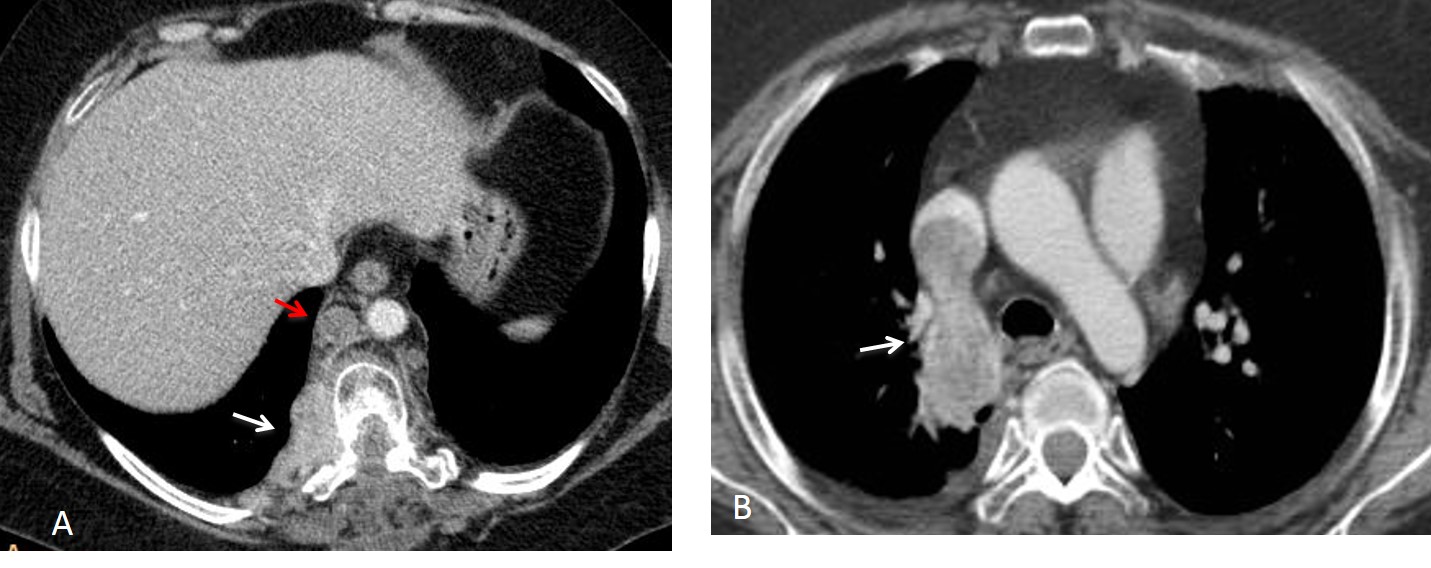
Fig. 2
Coronal CT confirms the azygos vein enlargement (Fig. 3a, arrow). PET-CT shows enhancement of the thrombus within the azygos (3b, arrows).
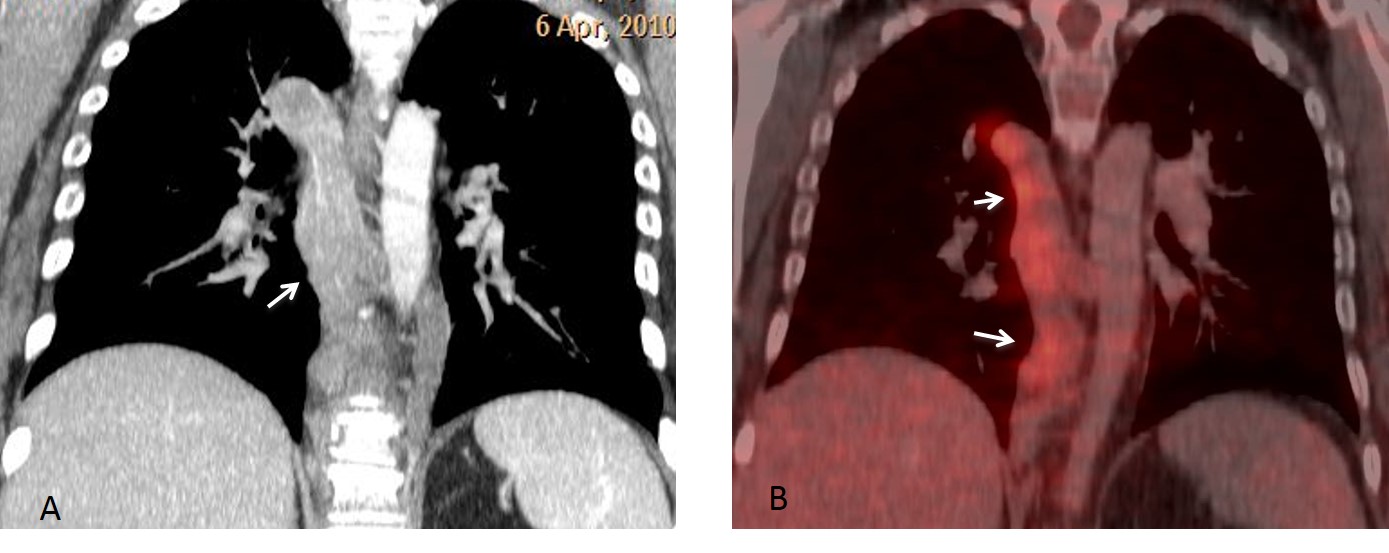
Fig. 3
Final diagnosis: enlarged azygos vein secondary to tumour thrombus.
This case is shown to comment about azygos vein enlargement. The azygos/hemiazygos system is a posterior venous pathway connected to the superior and inferior vena cava. The azygos vein ascends on the right side of the spine and arches anteriorly to join the SVC (azygos arch). The hemiazygos vein ascends on the left side and joins the azygos vein at the level of the 7th or 8th thoracic vertebra.
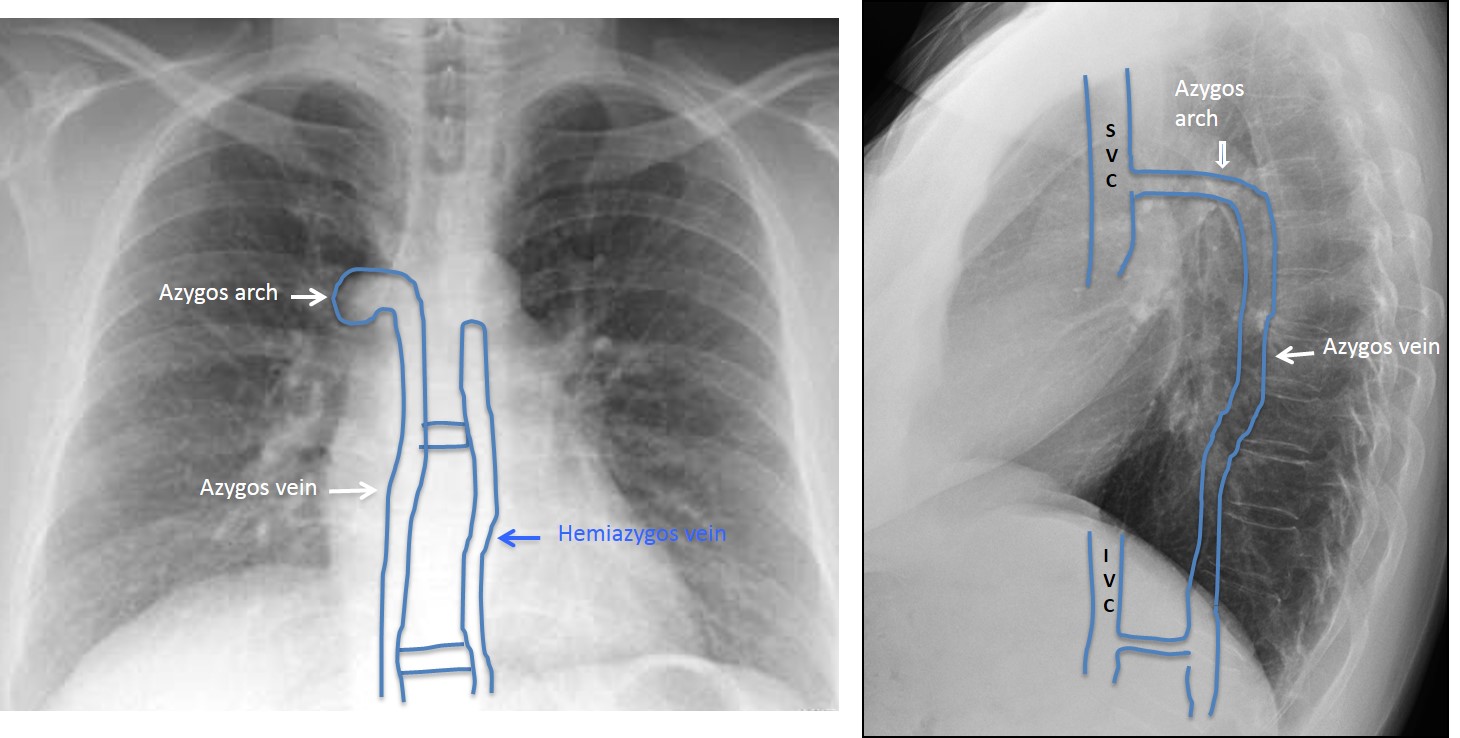
Fig. 4
For practical purposes, the azygos arch is the only part of the azygos vein visible in the PA chest radiograph. It is seen end-on as a round or oval mediastinal shadow at the take-off of the RUL bronchus (Fig. 5). It is visible in about 10% of upright PA radiographs, and is always visible in supine films.
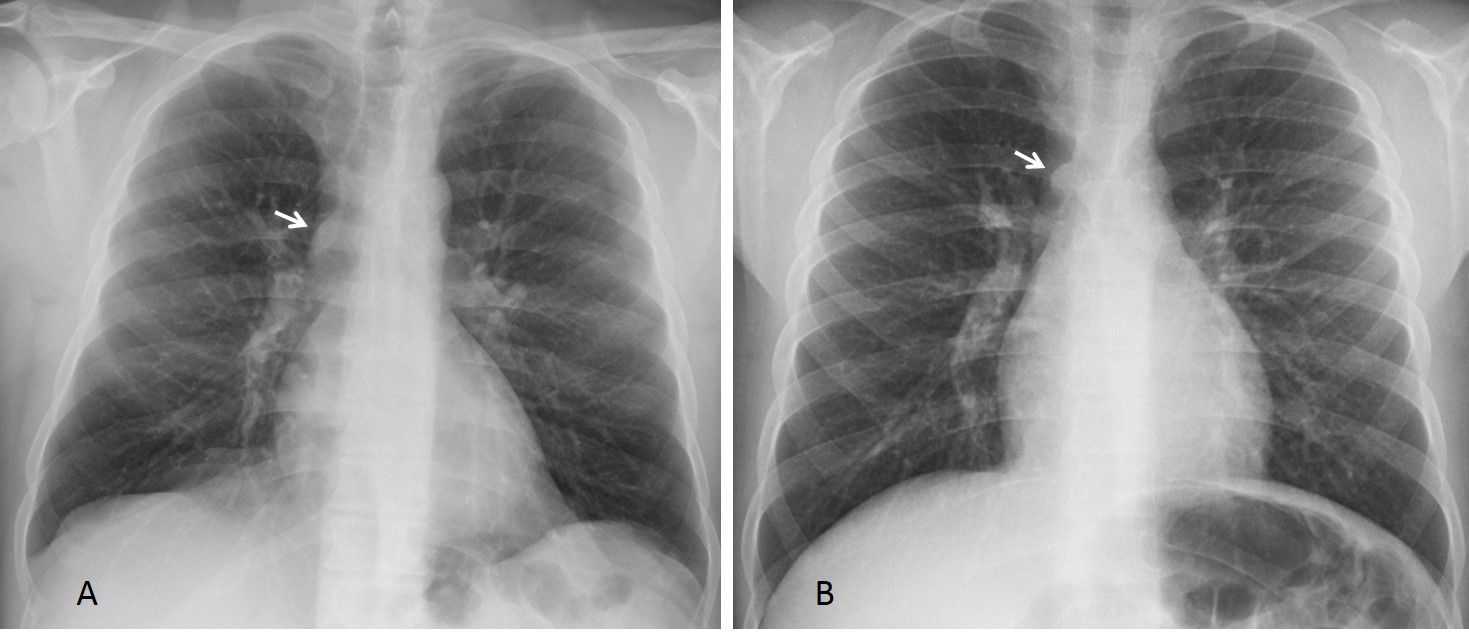
Fig. 5
Fig. 5. Two examples of a normal azygos arch. It has a lenticular shape in the first patient (A, arrow) and is rounded in the other one (B, arrow).
In the PA upright film, an azygos arch larger than 1cm is considered abnormal and should be investigated. It is important to emphasise that the size of the azygos arch cannot be evaluated in supine films.
An azygos arch larger than 1cm usually indicates increased blood flow in the azygos system. It may be non-obstructive or secondary to obstruction of the superior or inferior vena cava, in which case the azygos system acts as collateral drainage.
Very unusual causes of azygos arch enlargement are thrombosis, as in the case shown initially, or aneurysm.
Non-obstructive azygos enlargement is secondary to elevated right atrial pressure. Its most common cause is congestive heart failure and, occasionally, pericardial disease. The azygos arch reverts to normal size after heart failure improves (Fig. 6).
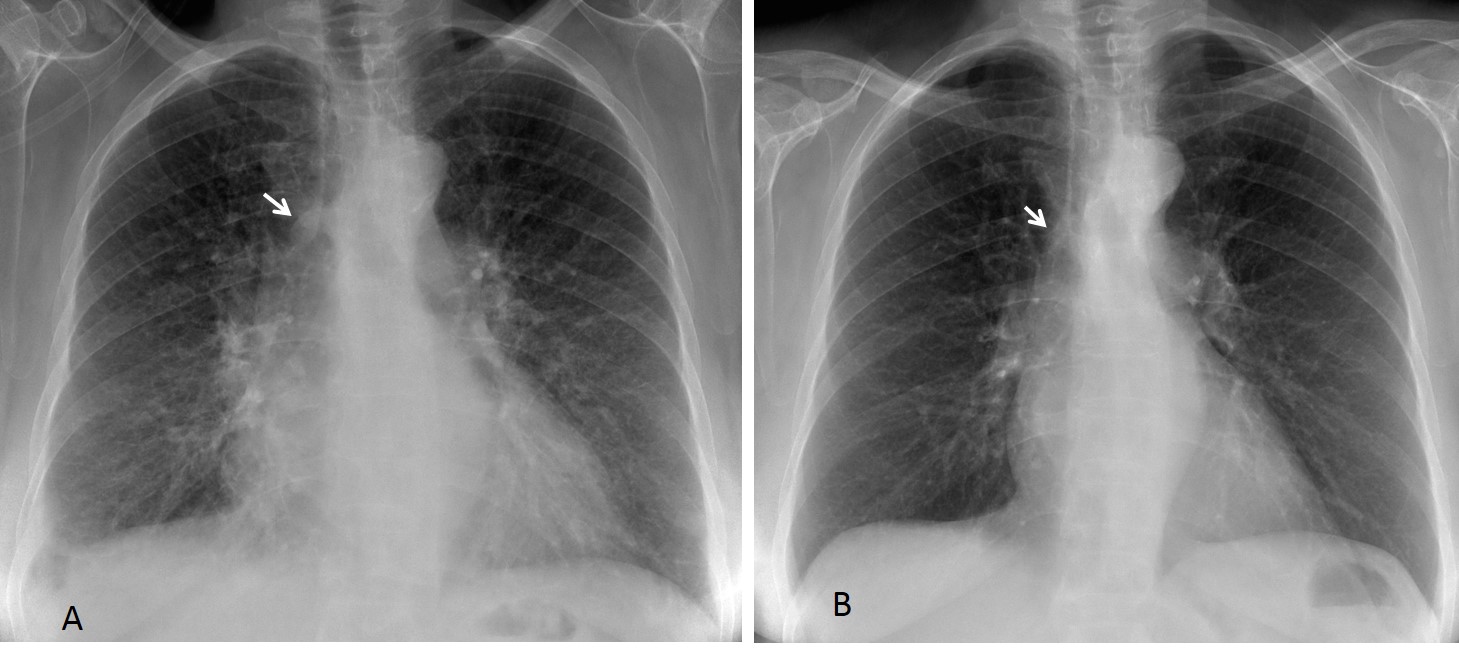
Fig. 6
Fig. 6 (above): 57-year-old woman with acute congestive heart failure. Note the enlarged azygos arch (A, arrow). After treatment, the signs of failure have disappeared and the azygos arch is smaller (B, arrow).
Portal hypertension is another cause of non-obstructive azygos enlargement. The blood flows towards the oesophageal and mediastinal veins, draining into the azygos system (Fig. 7).
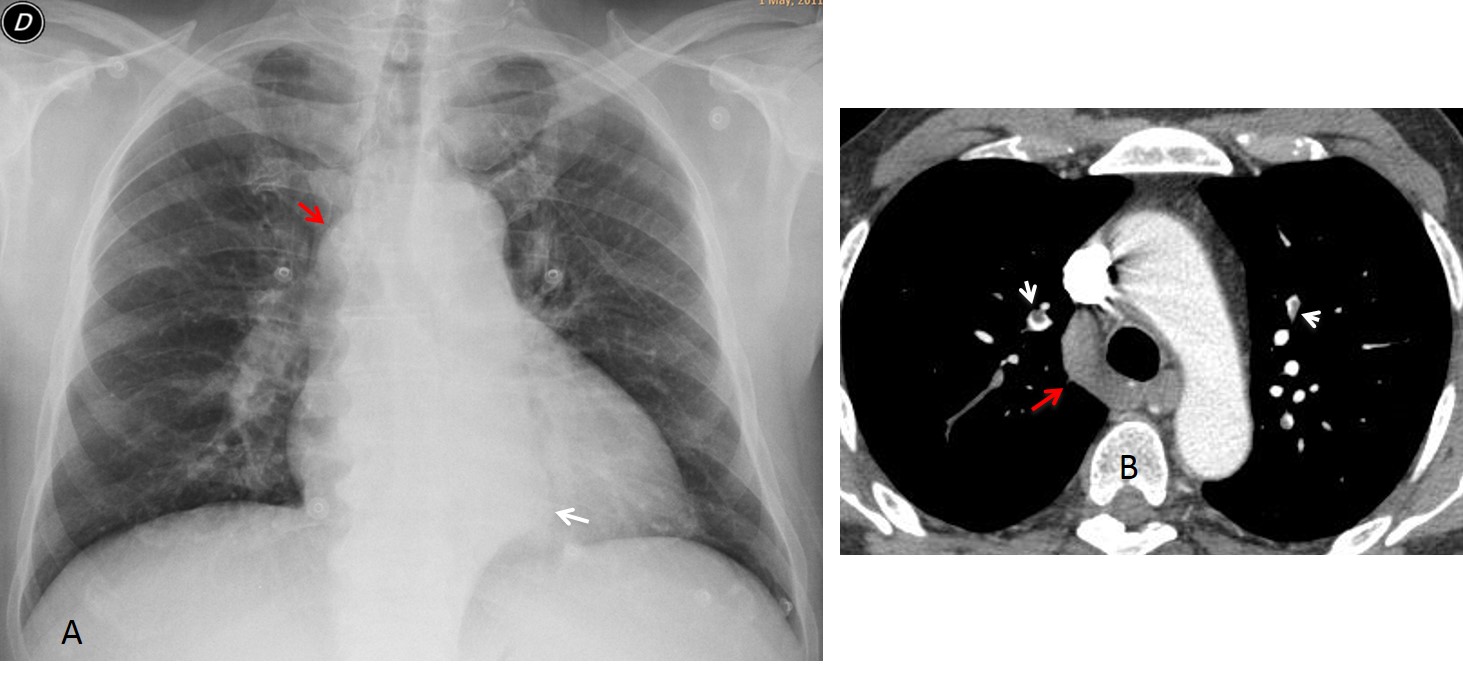
Fig. 7
Fig. 7 (above): 49-year-old man with suspected pulmonary embolism. PA chest film shows an enlarged azygos arch (A, red arrow) and a bulge in the mediastinum (A, white arrow). CT confirms the emboli (B, white arrows) and the enlarged azygos arch (B, red arrow).
Coronal CT (Fig. 8) shows that the mediastinal bulge corresponds to mediastinal varices (A, arrows). Note the marked splenomegaly. Oblique CT depicts the varices (D, white arrow), draining into the azygos vein (B, red arrow). Note the change in caliber of the azygos vein at the point of entry of the varices (B, yellow arrow). Diagnosis: unsuspected cirrhosis in a patient with unrelated pulmonary embolism.
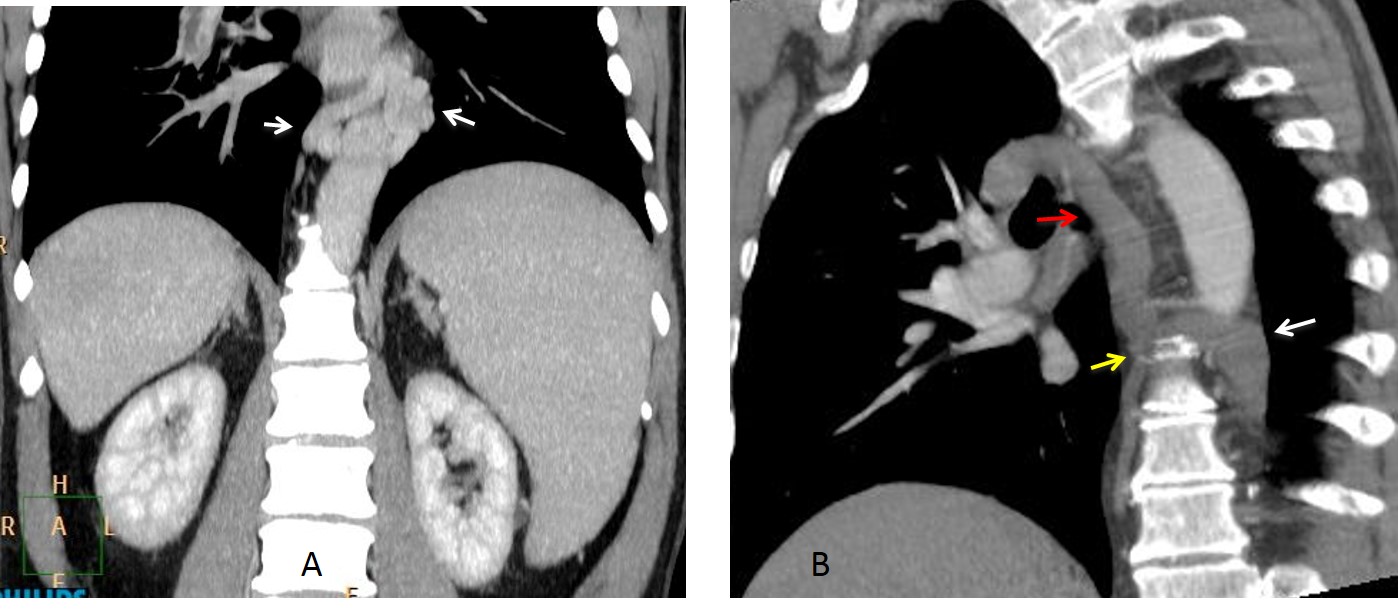
Fig. 8
Obstruction of superior or inferior vena cava are common causes of azygos vein enlargement. In these cases, the azygos system acts as a collateral pathway to derive the blood from the thrombosed vein towards the right atrium (Figs. 9 and 10). Lung cancer is the most common cause of SVC obstruction.
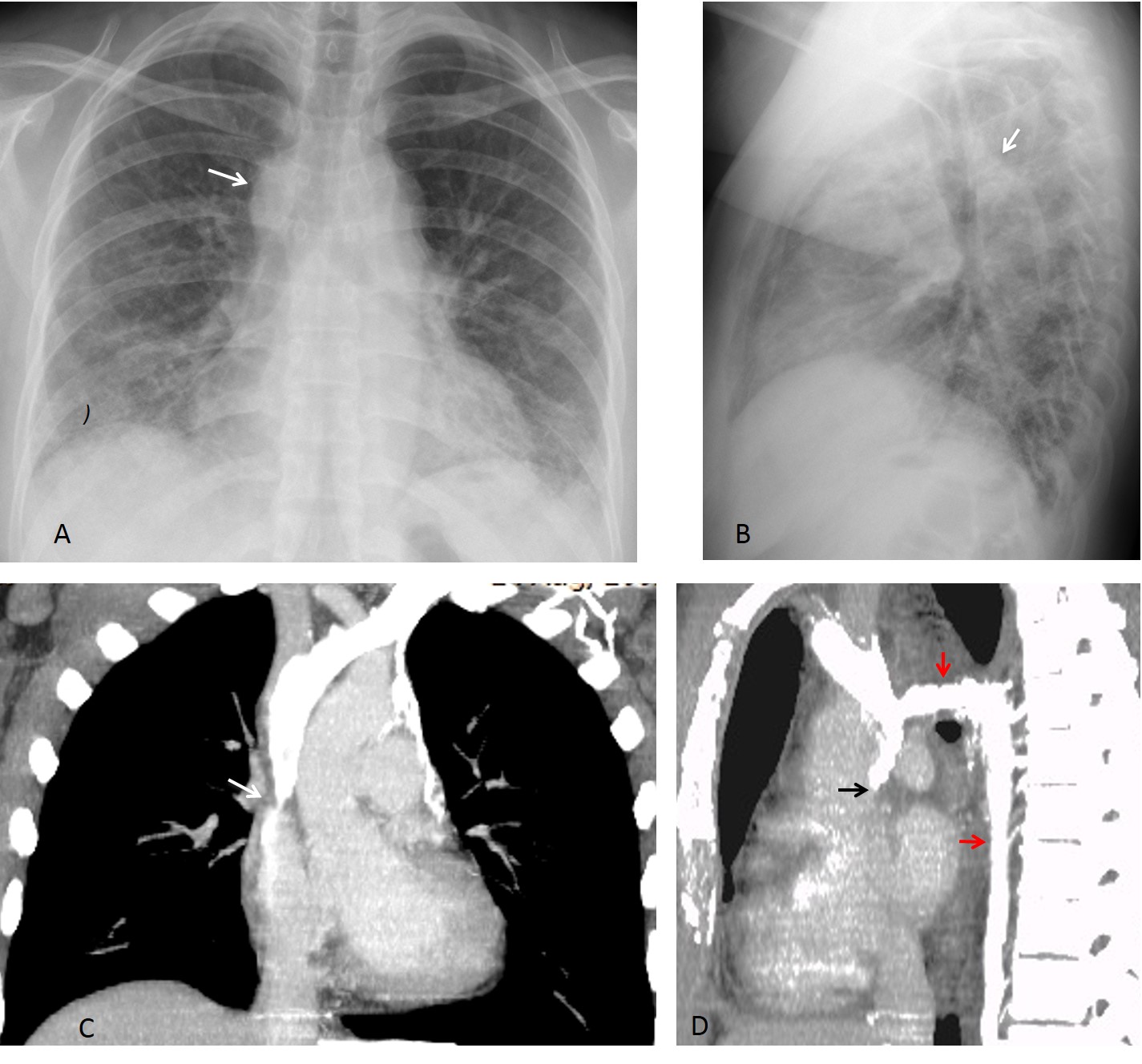
Fig. 9
Fig. 9 (above): 64-year-old man with Behçet syndrome. PA chest film shows ill-defined pulmonary opacities. The azygos arch is increased in size and visible in both the PA and lateral views of the chest (A,B, arrows). Enhanced CT images show marked SVC narrowing (C,D, arrows) with directing of blood flow towards the IVC through the azygos vein (D, red arrows).
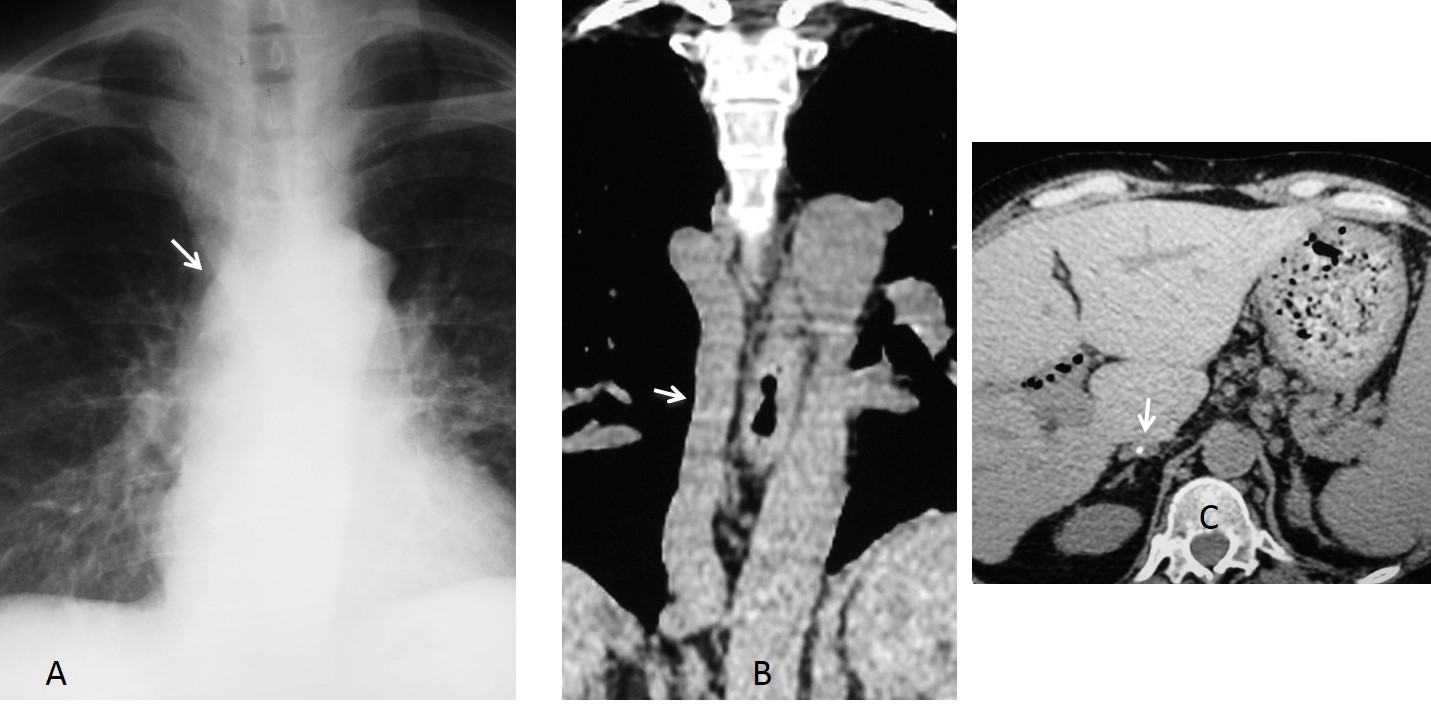
Fig. 10
Fig. 10 (above): 61-year-old patient with a history of leg phlebitis and IVC thrombosis. PA chest film shows a prominent azygos arch (A, arrow). Unenhanced CT demonstrates a large azygos vein (B, arrow) which is draining a collapsed IVC. Note the calcified thrombus in the IVC (C, arrow).
Azygos continuation of the IVC is a congenital anomaly in which the intrahepatic segment of the IVC is absent. Blood is shunted to the SVC through the azygos system. It occurs in about 1.5% of the population. It is an incidental finding in asymptomatic patients, usually discovered because of the enlarged azygos arch in the PA chest film (Fig. 11).
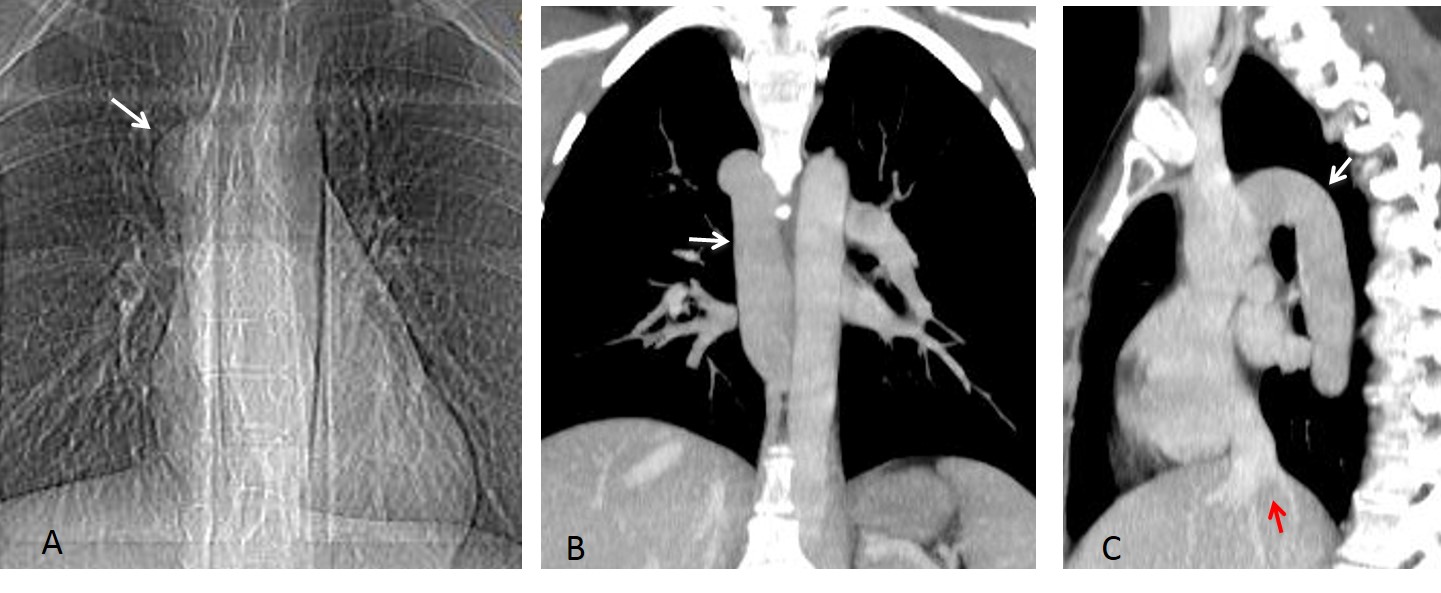
Fig. 11
Fig. 11 (above): azygos continuation of IVC. Scout film show a large azygos arch (A, arrow). Coronal and sagittal reconstructions depict a very large azygos vein (B,C, arrows). Note the absent intrahepatic segment of the IVC (C, red arrow).
A paratracheal lymph node (azygos node) may simulate an enlarged azygos vein in the PA view. The lateral view helps to make the distinction: The vein is behind the trachea, whereas the node is in front of it (Fig. 12). When in doubt, CT will clarify the situation (Fig. 13).
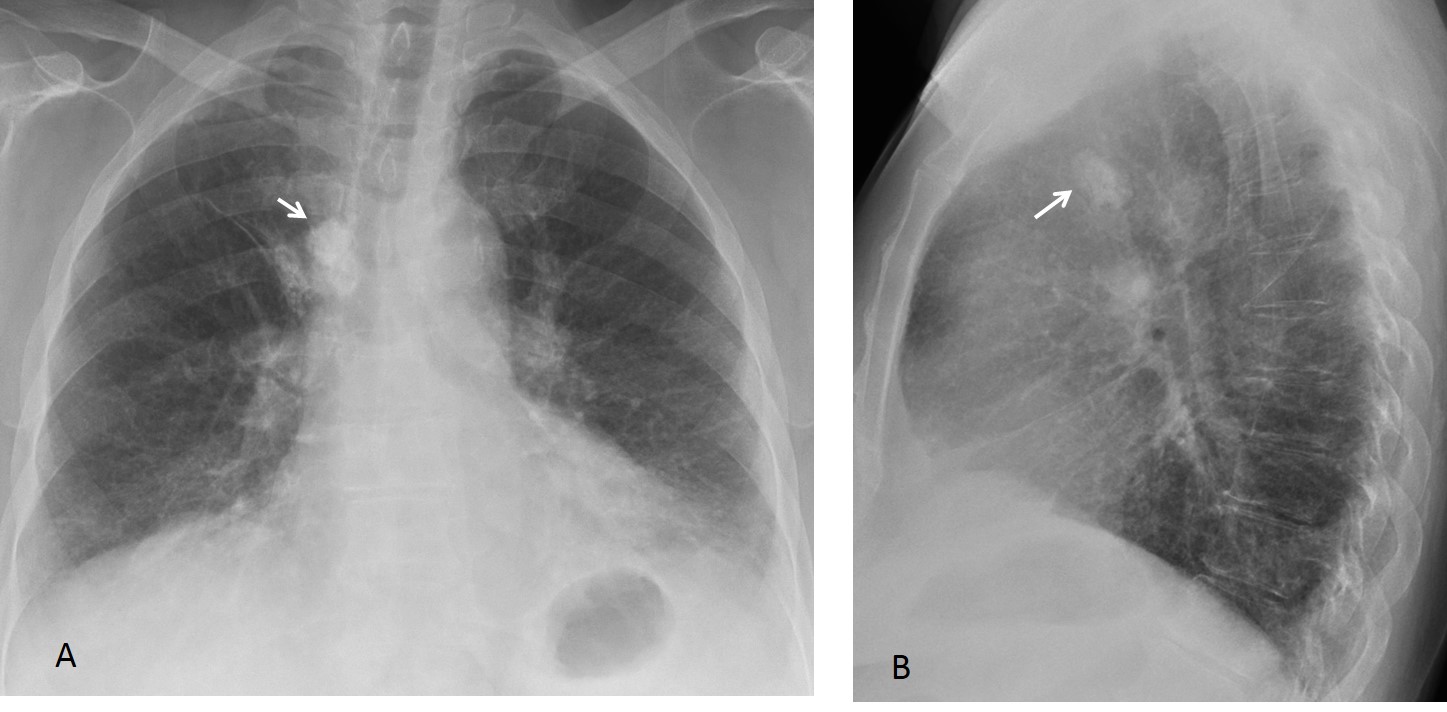
Fig. 12
Fig. 12 (above): 63-year-old woman with a calcified azygos node. The location of the node is similar to that of the azygos arch in the PA view (A, arrow) but it is anterior to the trachea in the lateral view (B, arrow).
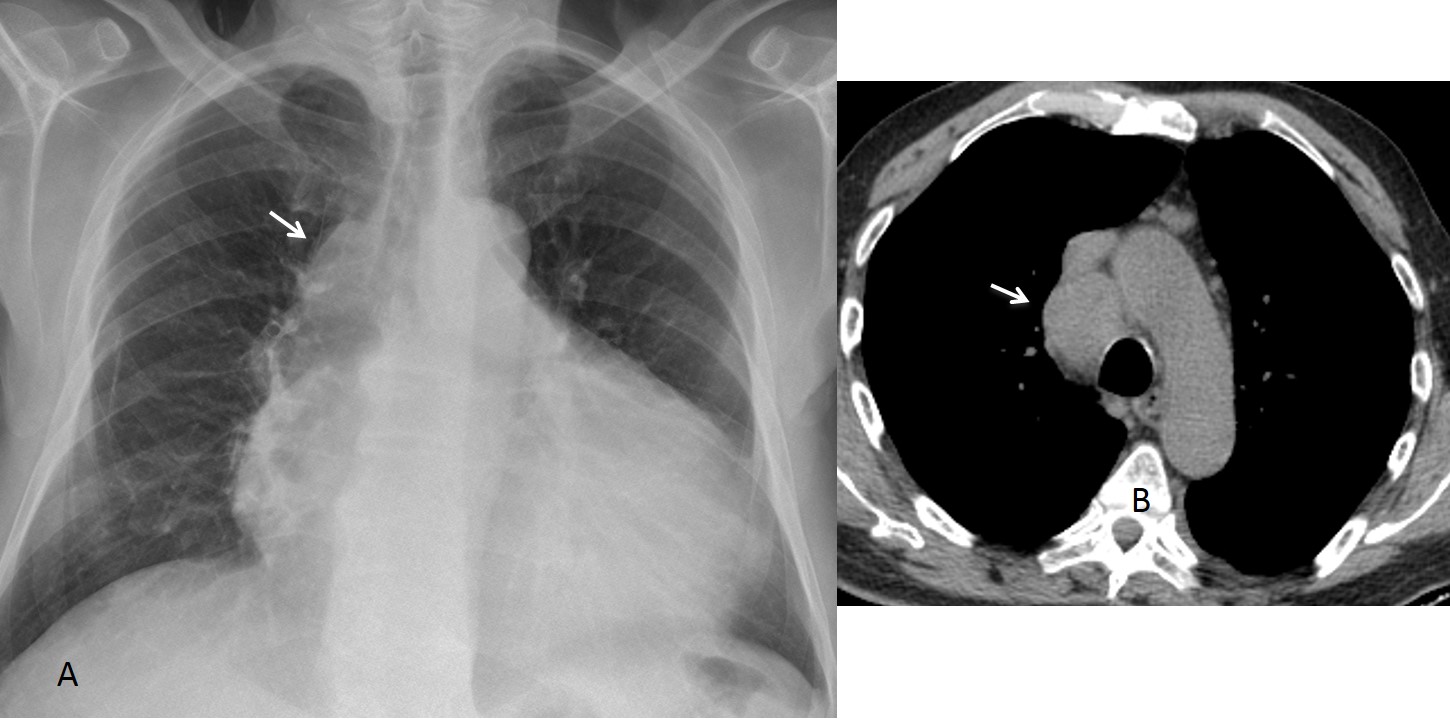
Fig. 13
Fig. 13 (above): 57-year-old man with cardiomegaly and an apparently enlarged azygos arch (A, arrow). Axial CT demonstrates a large lymph node (B, arrow), simulating the azygos arch in the PA film.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
1. An azygos arch larger than 1 cm in upright PA films is considered abnormal and should be investigated.
2. The size of the azygos arch cannot be evaluated in supine films.
3. Non-obstructive causes of azygos enlargement are congestive heart failure and occasionally, portal hypertension.
4. Obstructive causes of azygos enlargement are thrombosis of the superior or inferior vena cava and, occasionally, partial congenital absence of the IVC.


The quality of the films is not so good.
I think the finding is at the level of aortic arc but on the right side.
You are right about the finding, but you didn’t answer the questions.
Distended azygous vein
arcus venae azygos
There is a nodular lesion located in the projection of right tracheobronchial angle. I also see indistinct left tracheal wall ,above aortic arch, I also suspect a lesion there.
Additionally, lytic lesion of fifth rib on the right? (mid-axillary line). With all mentioned above, I would suspect metastases.
No lesion in the left tracheal wall or 5th rib.
….carissimo dr Pepe…per primo una condiderazione clinica-anamnestica….il soggetto è stato operato di S.Ewing un anno prima,…quindi sono stati fatti dei toraci precedenti….l’immagine era presente nei radiogrammi precedenti o è comparsa dopo? …mi sembra inoltre che , nei campi polmonari, specie a dx, ci siano immagini opache micronodulari….Pertanto , pur essendo quella la sede della v. Azygos, in quella sede ci sono ANCHE linfonodi….In conclusione se l’immagine non era presente nei radiogrammi precedenti e se si confermano , come micrometastasi polmonari quanto visto nei polmoni la conclusione è linfoadenopatia metastatica in sede N2…..
The lesion was not present in the chest radiographs one year earlier. The CT did not show micrometastases.
Did this patient have any relevant chemotherapy side effects(e.g. doxorubicin)?
No, to my knowledge
If other lesions are excluded (rib and trachea ok) I will go with enlarged azygos vein.
And I hope for patient’s sake this isn’t because of vertebroplasty material leakage into vascular system.
….carissimo dr pepe…la lesione è quindi connessa con la malattia di base:sarcoma di Ewing…..Se escludiamo l’adenopatia metastatica allora l”opacità è la vena azygos “dilatata”….tenendo presenti le connessioni emodinamiche del vaso, la sua dilatazione potrebbe rappresentare lo “scarico collaterale” di una eventuale occlusione della CVI(vena cava inferiore), occlusa su base trombotica-metastatica….
On the PA view the right hila appears to be elevated with respect to the left. There is also a faint rounded opacification just superior to the right hila. The lateral view seems to show a rounded irregular opacification in the middle mediastinal compartment just anterior to the spine. The patient has a history of Ewing sarcoma which I believe most frequently gives metastases to bone and the lungs. I would consider this a suspicious lesion and follow-up with a CT to rule out metastatic disease.
At this time of the day I can safely congratulate Laurens for being the first to mention the azygos vein and Genchi Bari for giving an explanation of the findings.
Full answer tomorrow.
..grazie dr.Pepe…..ti prego comunicare al prof. Cáceres quest’altro goal del piccolo Bari…..non sempre si può vincere ….anche i “ricchi”(BARCA), piangono…..!
Thank you dr. Pepe!!! 🙂 Just a few more days till a new case! 🙂