This week I want to show you a neuro/skeletal case, relating to a 25-year-old male with a 3-month history of sciatica.
1. Schwannoma
2. Perineural cyst
3. Sacrococcygeal teratoma
4. None of the above
Findings: Non-enhanced CT shows a soft tissue mass with neural foramen enlargement and bone remodelling (arrows).
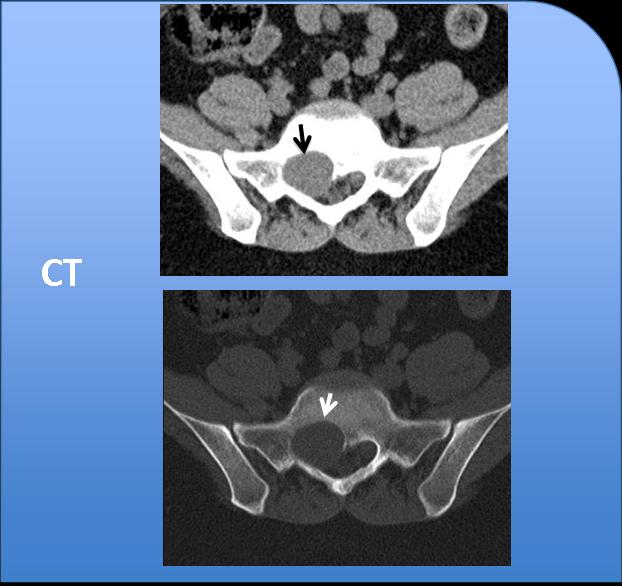
Fig. 4
MRI depicts a well-defined bilobed soft tissue mass (arrows) with intraspinal and presacral components. The mass is hypointense on T1W, heterogeneous on T2W, and shows high and low signal intensities and uniform heterogeneous enhancement with gadolinium.
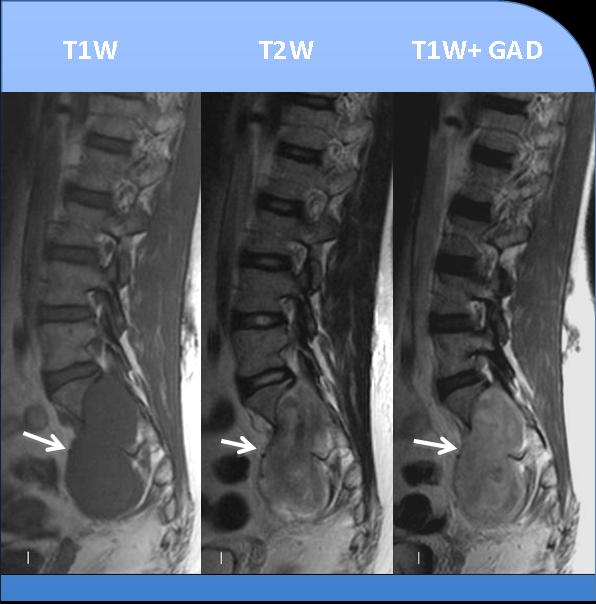
Fig. 5
These findings suggest schwannoma as the most likely diagnosis
Schwannomas are the most common intradural extramedullary masses. They grow slowly and cause bone remodelling, vertebral body scalloping, and neural foraminal enlargement (yellow arrow).
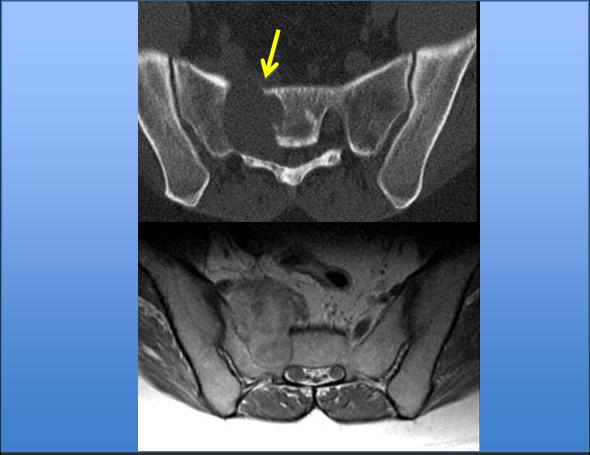
Fig. 6
On MRI imaging, schwannoma shows homogeneous or heterogeneous signal or density. Cystic areas are often seen within the tumour. The solid component enhances with contrast. Haemorrhage and calcification are rare.
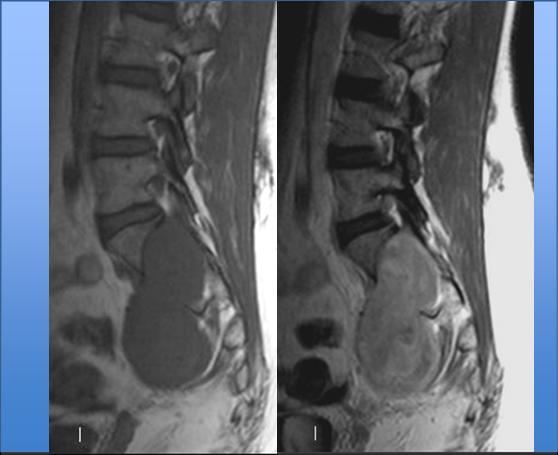
Fig. 7
Multiple schwannomas are usually found when the condition is associated with neurofibromatosis.
DIFFERENTIAL DIAGNOSIS
Perineural cyst: has homogeneous high signal intensity on T2W images following the CSF signal characteristics, and no enhancement with gadolinium.
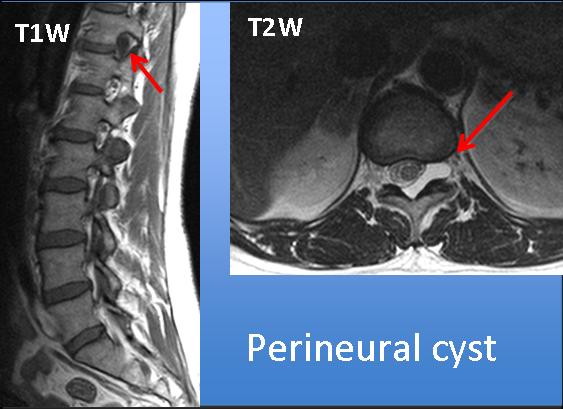
Fig. 8
Sacrococcygeal teratoma: important clues to look for are sacral malformations and heterogeneous content (eg. fat and calcium) within the mass.
Anterior sacral meningocele: important to look for associated sacral anomalies. Fluid content, highly hyperintense on T2W images, no enhancement with gadolinium.
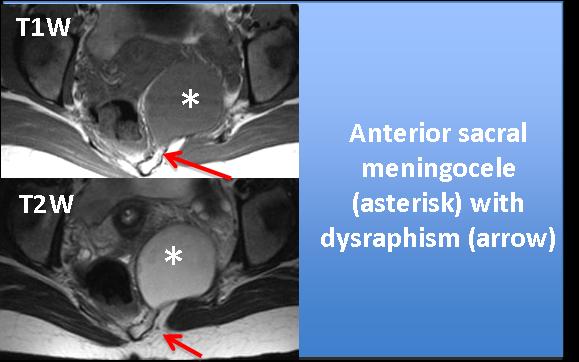
Fig. 9

Follow Dr. Pepe’s advice:
Follow Dr. Pepe’s advice:
- Spinal schwannomas present as dumb-bell tumours and cause neural foramina enlargement and bone remodelling
- High signal intensity on T2W imaging and gadolinium enhancement differentiate neural tumours from cystic masses (perineural cyst, or meningocele).
- Associated sacral or coccygeal anomalies are important clues to differentiate neural tumours from teratoma or anterior sacral meningocele.
Suggested reading: Wald JT. Imaging of spinal neoplasm. Radiol Clin North Am. 2012; 50:749-76.
Case prepared by Laura Oleaga, MD

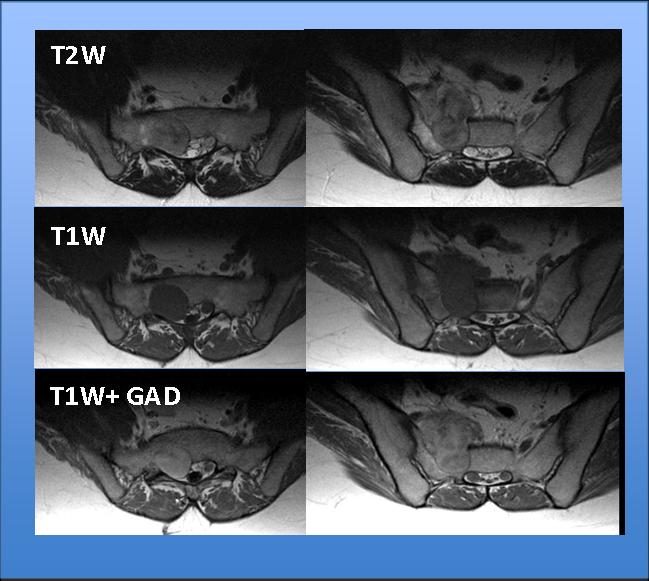
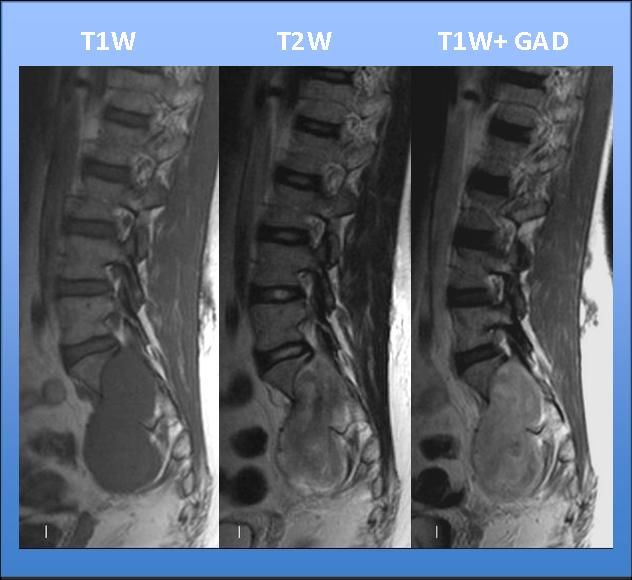



Pre and post contrast T1W, and T2W MR images with axial CT images showing a well defined focal lesion in the sacrum on right side at the level of SI vertebrae. The lesion is hypointense on T1W images and heterogenously hyperintense on T2W images with target appearance on T2(signal not parallel to CSF-rules out perineural cyst)). No evidence of any hyperintense T2 signal suggesting fatty component or hemorrhage is seen in it. No calcification is seen ruling out teratoma. The lesion is showing heterogenous enhancement on post contrast images. There is remodelling with expansion of the right ventral sacral foramen and the lesion is seen to extend into the presaral space on right side with dumbell appearance in saggital images.In axial T1W MR images the 1st sacral nerve root appears medial to the lesion.The diagnosis will be nerve sheath tumor(it is not possible to differentiate exactly between neurofobroma and schwannoma but the feature favouring schwannoma are -heterogenous enhacement and eccenteric S1 nerve root).
shwannoma
shwannoma
Tumore benigno ,intradurale- extramidollare(TIEM).Ipointenso in T1;Iperintenso in T2;con impregnazione intensa in T1.Margini regolari con dislocazione della cauda equina. Diagnosi :Schawannoma.
I reckon it is a dumbell-shaped mass. There are some nonenhancing, as well as hypointense on T2-weighted images, areas. Why not neurofibroma?
I would also say nerve sheath tumor (schwannoma).
I would consider in my differential for sacral mass: chordoma (destructive, with calcifications and very very hyperintense on T2 images), GCT (typically hypo on T2 and hypervascular, would not expect such sclerotic borders), teratoma (loof for fat hyper on t1), ABC (pseudo agressive lytic lesion with classical blood levels), osteoblastoma (lytic with or without sclerotic nidus and with solid nonagressive periosteal reaction), mets and plasmacytoma-mieloma (agressive and much more freq in older patients) and a small cell tumor like Ewing- PNET (much more heterogeneous and would expect more agressive appearance). My first option as I said would be by far the Nerve Sheath Tumor (schwannoma).
Classical dumbell shaped mass exiting the neural foramen. Neurofibroma. Less likely schwanoma. I would discuss further management with the primary physician. To differentiate the two, I would like to perfom MRI guided core biopsy. This will save the patient from Ct induced radiation. Other option would be to have complete surgical resection and send the specimen for histopathology.
Nerve sheath tumour.
Dumbbell shaped, widening the neural foramen, and the other reasons mentioned by colleagues.
The findings are consistent with Schwannoma. (Complicated perineural cysts are extremely rare)
Again, you are offering excellent discussions of the case. Imagine you have already obtained the Diploma. If not, you will not have any problems passing the examination.