Dr. Pepe’s Diploma Casebook: Case 8 – SOLVED!
Dear Friends,
This week’s case is a 61-year-old man who was treated surgically for colon cancer 9 months ago. Normal CT at that time.
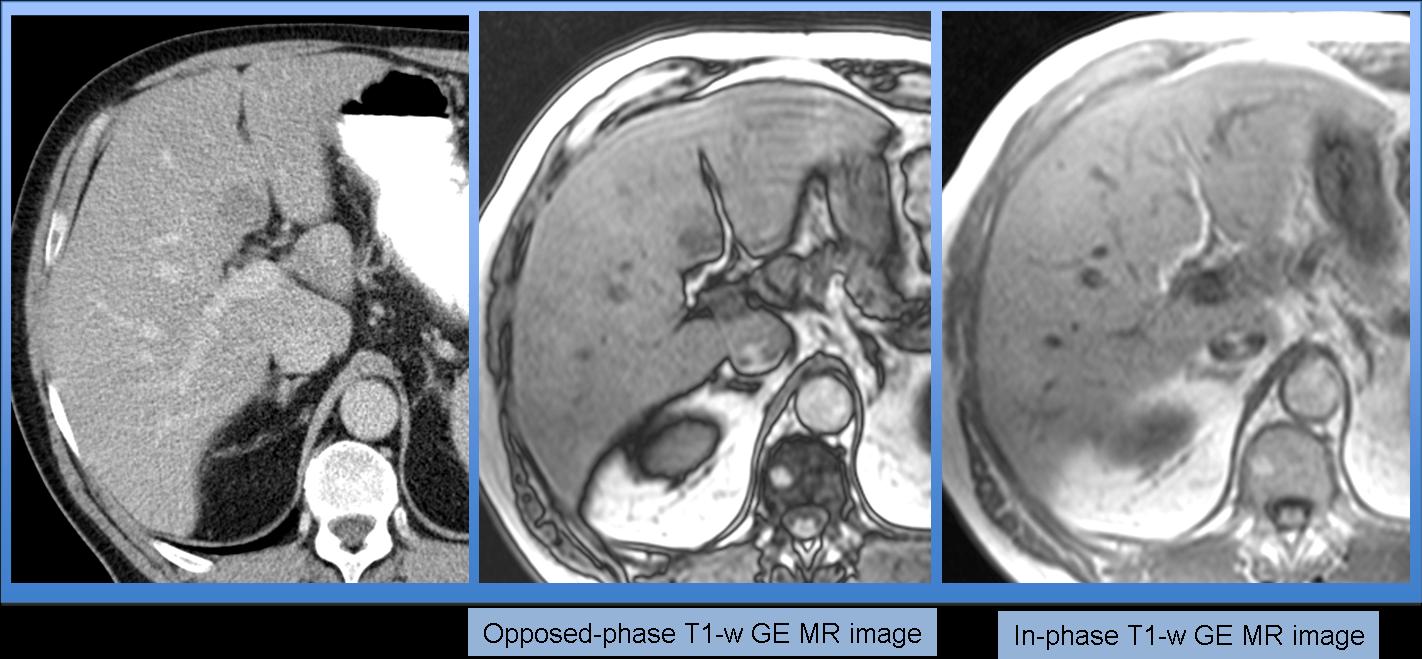
Fig. 1
Most likely diagnosis:
1. Liver metastasis
2. Nodular fatty infiltration of the liver
3. Hepatocellular carcinoma
4. None of the above
Findings: (a) Opposed-phase (OP) T1-w gradient-echo (GE) image of the liver shows a hypointense nodule in seg. IV (arrow). (b) On in-phase (IP) T1-w GE image, the nodule is not seen because it is isointense to the liver parenchyma. (c) The nodule is hyperintense on IP-OP subtraction image (arrow). (d) On Gd-enhanced OP arterial phase, the nodule is hypovascular and (e) no capsule is seen on OP venous phase image (arrows).
Final diagnosis: Nodular focal fatty infiltration of the liver.
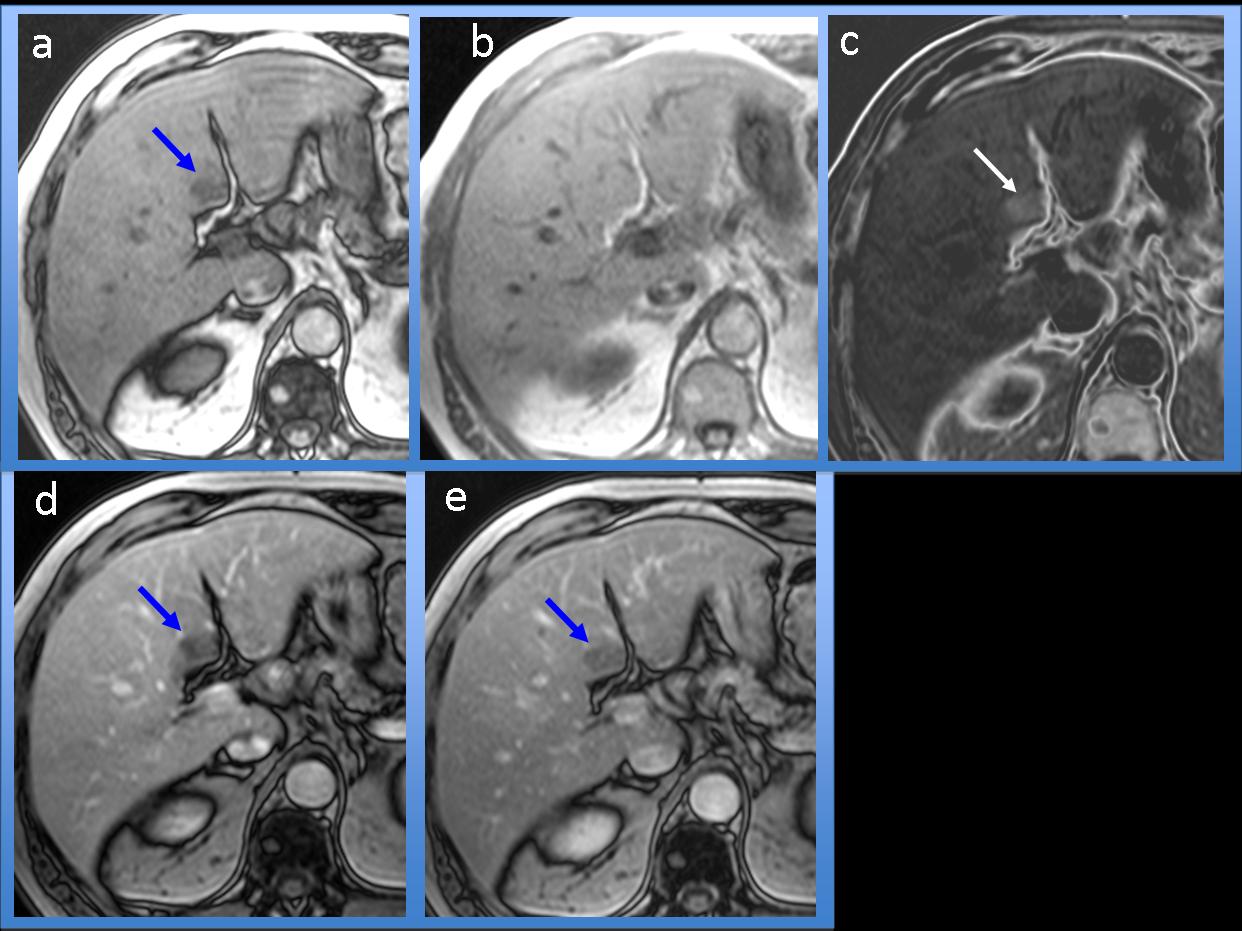
Fig. 2
On CT studies, nodular focal fatty infiltration of the liver is difficult to diagnose because the amount of fat usually does not suffice to reach CT density values (-90 HU); thus it mimics other, non-fatty liver lesions. However, the diagnosis can be easily reached using a chemical-shift T1-w GE MR imaging technique, which is based on the difference in resonance frequency of water and fat protons (OP and IP images). This technique enables accurate differentiation between liver nodules with a fatty component and others without fat. Nodules comprised of a mixture of water and fat show notable signal intensity (SI) loss on OP images compared with the SI on IP images, whereas in lesions without fatty component, the SI is the same on both OP and IP images.
Additionally, IP and OP images can be subtracted, and this capability is also useful for differentiating between lesions with and without fat. Whereas fatty lesions show high SI on IP-OP subtraction images, lesions without fat show a complete absence of SI.
Chemical-shift imaging: Findings in a lesion without fatty component
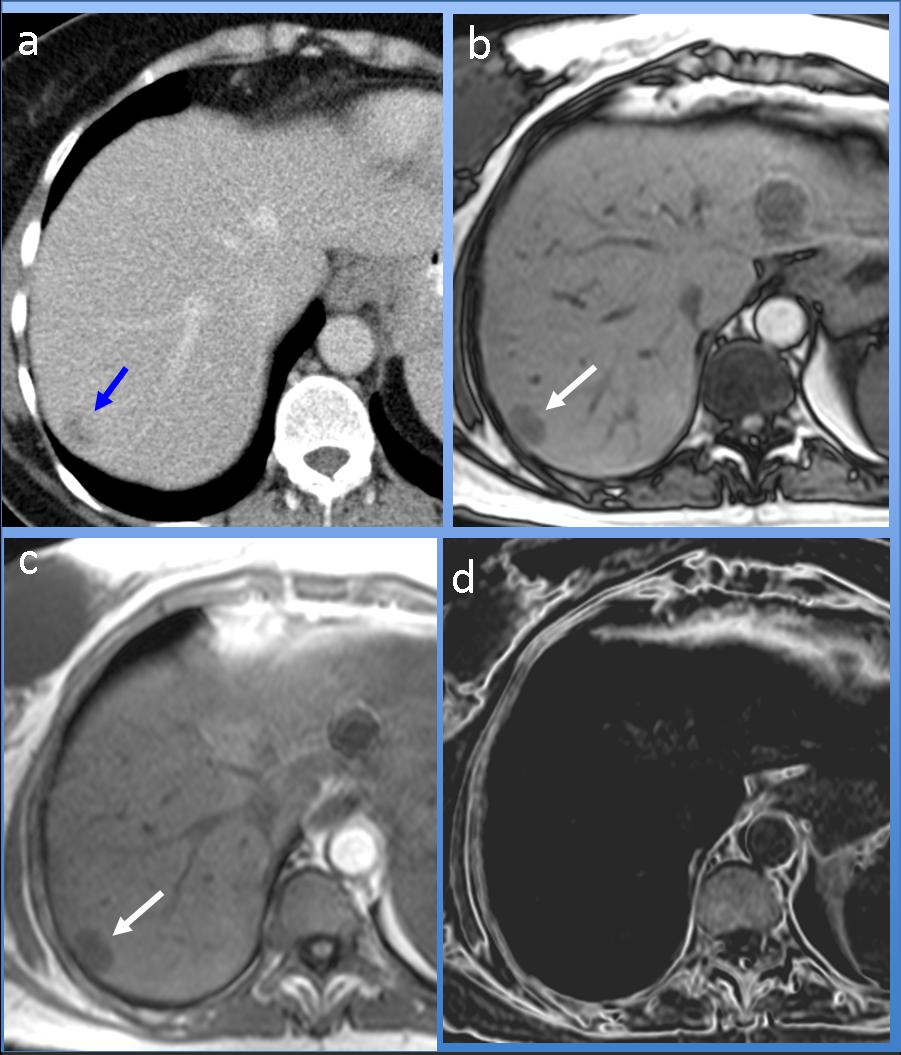
Fig. 3
Chemical-shift imaging in one case of liver lesions without fat: (a) On CT study, a hypodense nodule is seen in seg. VII (arrow). The SI of the nodule is the same in both OP (b) and IP (c) T1-w GE images (arrows), thus confirming the absence of fatty component in the nodule. (d) In the IP-OP subtraction image, the lesion shows total absence of signal intensity because there is no difference in SI between the IP and OP images.
Diagnosis: Liver metastasis
The differential diagnosis of nodular focal fatty infiltration of the liver includes other nodules that can have fatty component, like angiomyolipoma (AML), hepatocellular adenoma (HA) or hepatocellular carcinoma (HCC). AML, HA, and HCC are usually hypervascular lesions, in contrast to nodular fatty infiltration, which is not hypervascular. In addition, HA and HCC usually have a peripheral capsule, whereas fatty infiltration of the liver never has a capsule.
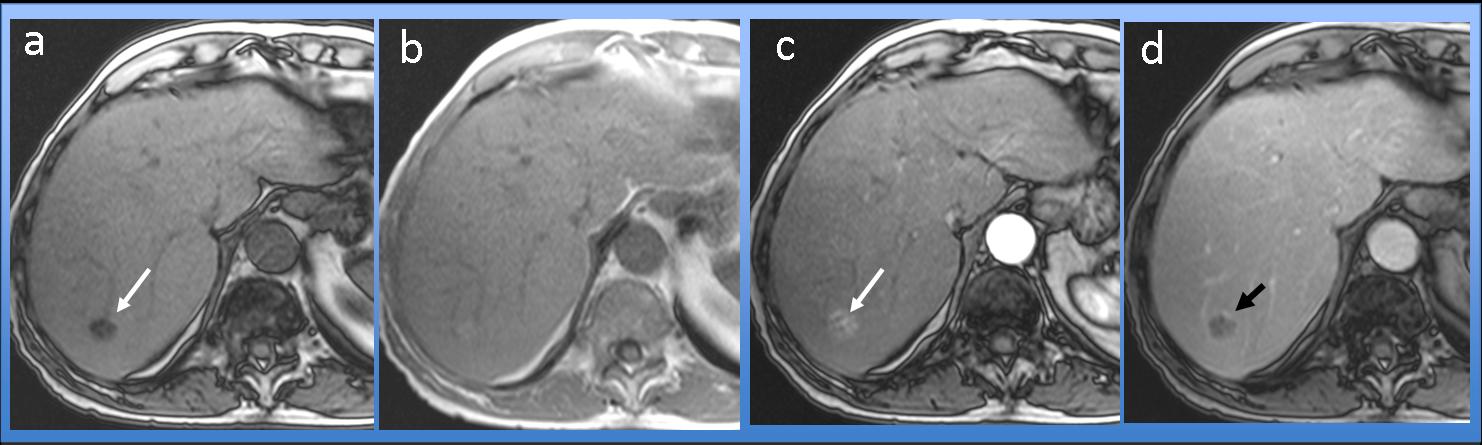
Fig. 4
Chemical-shift imaging in a case of hepatocellular carcinoma with fat. (a) OP T1-w GE image shows a hypointense nodule in seg. VII (arrow). (b) The nodule is almost imperceptible in the IP T1-w GE image. (c) On arterial phase Gd-enhanced OP T1-w imaging, the lesion is hypervascular (arrow). (d) A thin peripheral capsule is seen in the venous phase OP image (arrow).
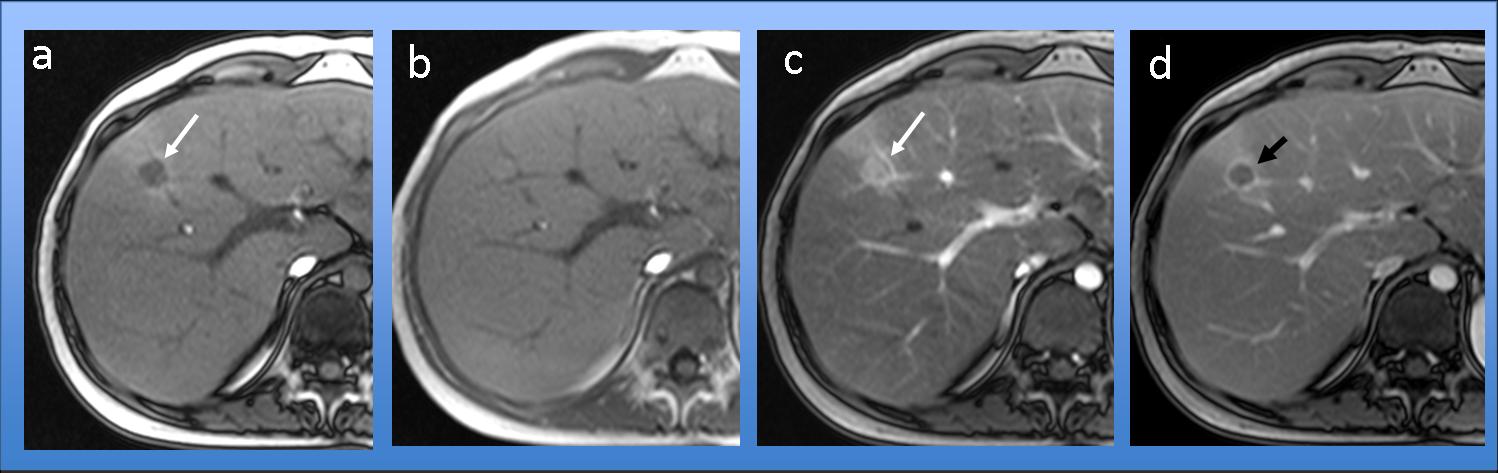
Fig. 5
Chemical-shift imaging in a case of hepatocellular adenoma with fat. (a) OP T1-w GE image shows a hypointense nodule in seg. IV (arrow). (b) The nodule is almost isointense and is imperceptible in the IP T1-w GE image. (c) On arterial phase Gd-enhanced OP T1-w imaging, the lesion is hypervascular (arrow). (d) A nice peripheral capsule (arrow) is seen in the venous phase OP image.

Follow Dr. Pepe’s advice
Follow Dr. Pepe’s advice:
- Chemical-shift MR imaging differentiates between liver lesions with or without a fatty component. In lesions with a fatty component, there is a notable difference in SI between OP and IP images, whereas in lesions without fat, SI is the same on both OP and IP images.
- In IP-OP subtraction images, nodules with fat show a high SI and those without fat show absence of SI.
- Aside from nodular fatty infiltration of the liver, other liver lesions like AML, HA or HCC may contain fat. In these cases, the presence of a capsule or a high SI on Gd-enhanced arterial phase images helps to suggest the diagnosis.
References
- Martin J, Sentis M, Puig J et al. Comparison of In-phase and Opposed-Phase GRE and conventional SE MR pulse sequences
in T1-weighted imaging of liver lesions. J Comput Assist Tomogr 1996 Nov-Dec; 20 (6). 890-7 - Merkle EM, Nelson RC. Dual Gradient-Echo In-Phase and Opposed-Phase Hepatic MR Imaging: A useful Tool for Evaluating
More Than Fatty Infiltration or Fatty Sparing. Radiographics 2006;26:1409-1418
Case prepared by Julio Martin MD


Its nodular fatty infiltration of the liver because the signal falls in the oppossed-fase T1w.
I think that with the OP and the IP MRI sequences the findings suggest a Nodular fatty infiltration of the liver. Moreover that is one of the typical localization.
Nodular fatty infiltration of the liver.
In normal practice we should always look at the arterial phase – HCC might have a major fatty component. The arterial phase would show peripheral (most often continuous and heterogeneous) enhancement, most often with washout in the portal venous/hepatic venous phase.
Besides that, HCC is obviously unlikely here since there are no features of cirrhosis.
Should be the fatty infiltration of the liver.there is signal loss in the FS images suggesting as the fatty composition .there is No mass effect and therefore no findings of arteriel enhancment and anyportal shunting.however IF a patent has a history of malignancy in other sites,the lesion is almost % 90 Probably benign.
A follow up 3 months US should be offered.
L’esame tc mostra lesione ipodensa. L’esame rm con sequenze pesate in T1 GE in opposizione di fase, dimostra lesione ipointensa ed isointensa livello della porta hepatis. Tale lesione non può essere un hhc , perchè non era presente alla tc iniziale, si presenta in un fegato non cirrotico e non può raggiungere tali dimensioni in 9mesi. Restano pertanto 2 ipotesi:metastasi ed area focale di infiltrazione grassa.L’esame rm è stato eseguito , senza mdc, in condizioni basali(sufficienti pertanto a formulare una diagnosi) che è di area focale di grasso, per le caratteristiche di segnale GE T1 in opposizione di fase, per la sede(porta hepatis) e per la mancanza di effetto-massa.
Based on the chemical shift sequences, it’s focal fatty infiltration.
steatose focale segment IV coussinet graisseux
en opposition de phase le signal graisseux chutte
Aunque el cáncer de colon tiende a provocar metástasis hepáticas, por las características de la imagen se trataría de una lesión en relación con infiltración grasa focalizada en el segmento IV
2. Nodular fatty infiltration of the liver
Nodular fatty infiltration of the liver because the signal dropped in T1 opposite of phase.
Nodular fatty infiltration of the liver because the signal dropped in T1 opposite of phase and also there isn’t an enhancing rim of the lesion on CT ( as one would expect in a colon cancer metastasis)
Findings
Focal nodular lesion at the medial segment of left liver lobe, near the calciform ligament , which is a typical location of focal nodular fatty infiltration.
In addition the MRI out of face sequence states , that it is a fatty lesion
He had a recent previous ct, so if it is a hcc with a fatty component , we have to expect its existense at the previous exam.
Colon metastases very rarely have a fatty component.
The patient possibly receives chemotherapy , which has caused the diffuse fatty infiltration of the liver and has decreased substantially its attenuation. That is why we have the faulse impression of I.v constrast enhanced liver parechyma (no one tell us about I.v constrast administration)
The most suitable diagnosis could be focal nodular fatty infiltration
can i ask you to maintain us informed about updates on your site? lista de emails lista de emails lista de emails lista de emails lista de emails