This year I intend to discuss the basic principles of interpreting chest radiographs, under the heading, “The Beauty of Basic Knowledge”.
I plan to structure the discussion into three main parts, which will take us through the whole academic year:
This week’s case is the first chapter of my ‘painless approach to interpretation’. Interpreting chest radiographs is not difficult if we follow Confucius’ saying: “ A journey of a thousand miles begins with a single step”. As a clinical radiologist, my first step is to ask myself three questions:
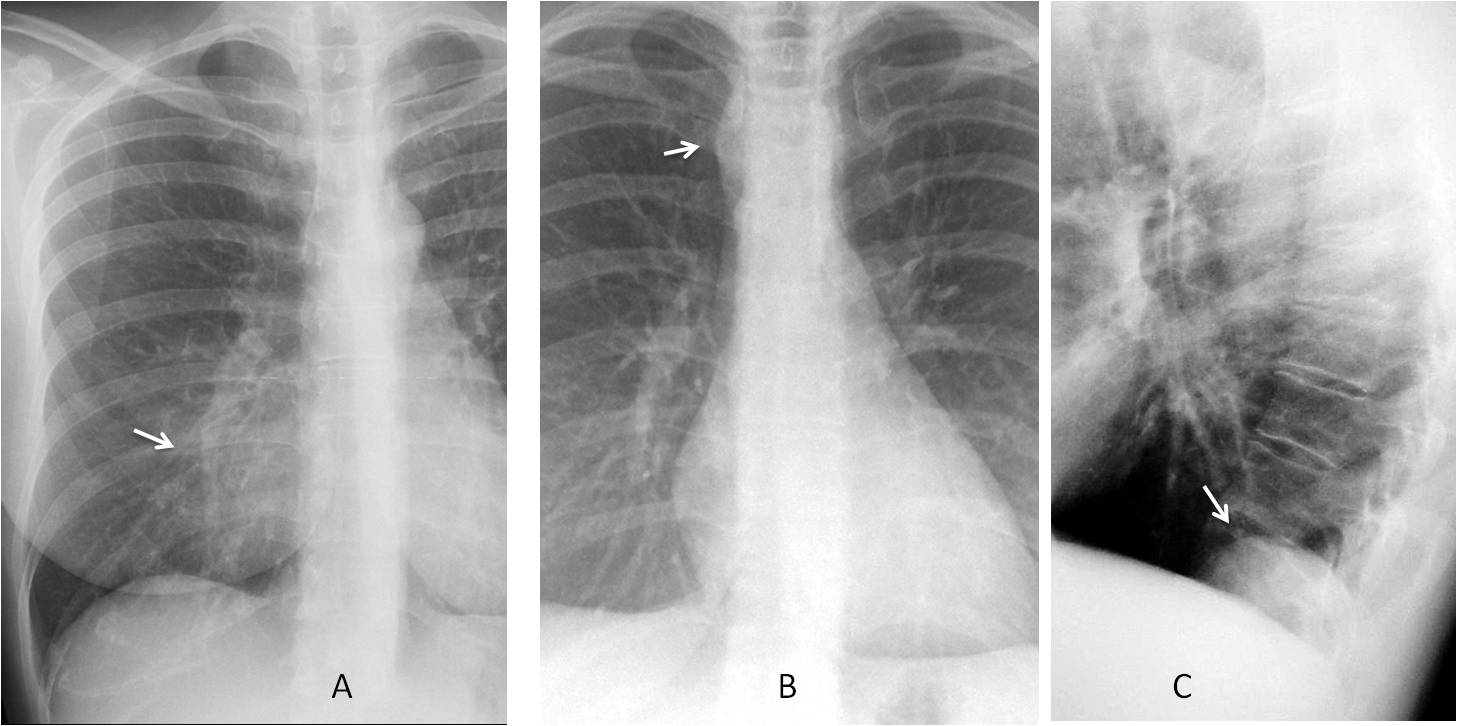
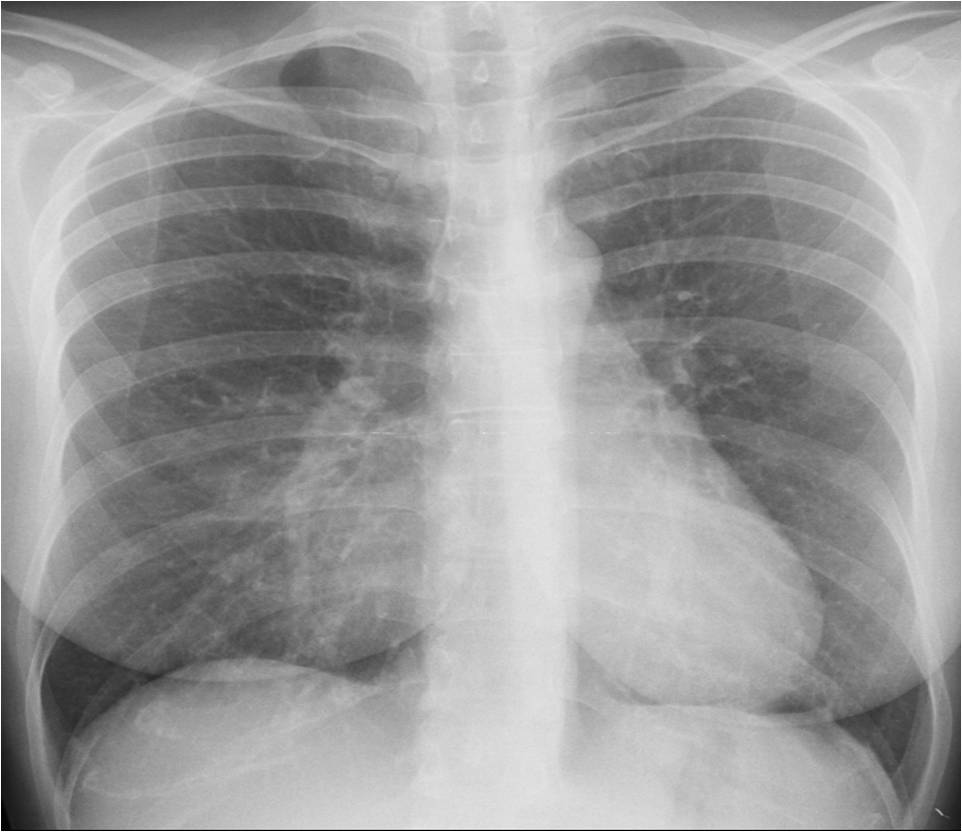
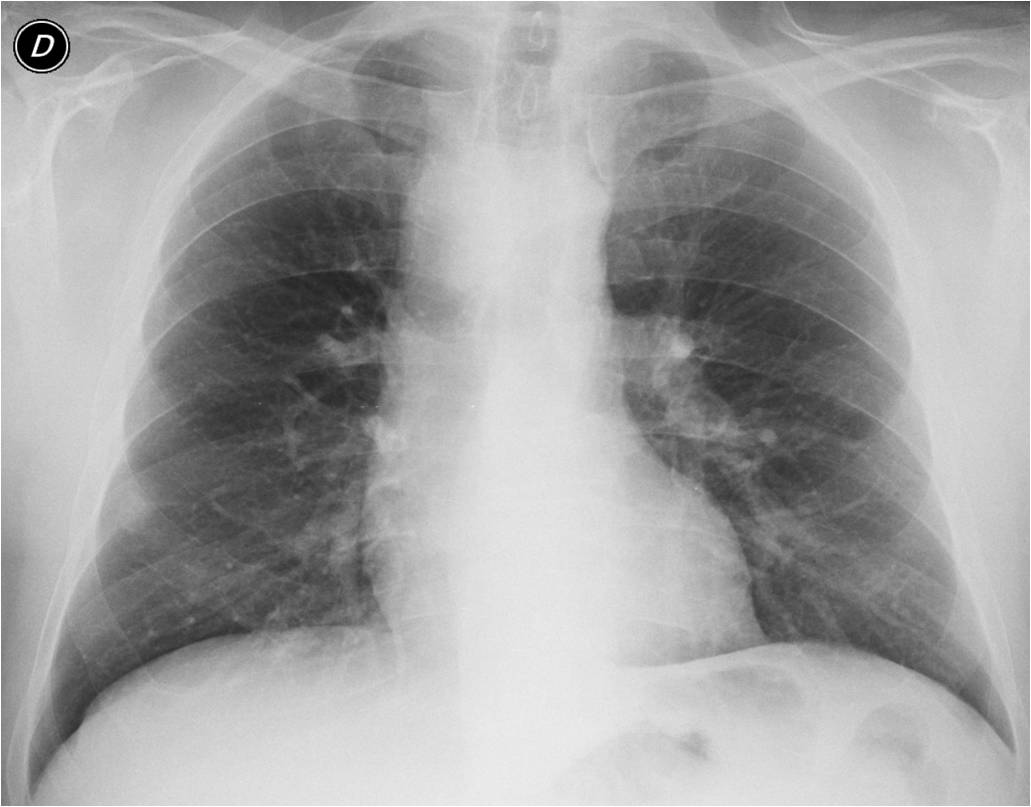
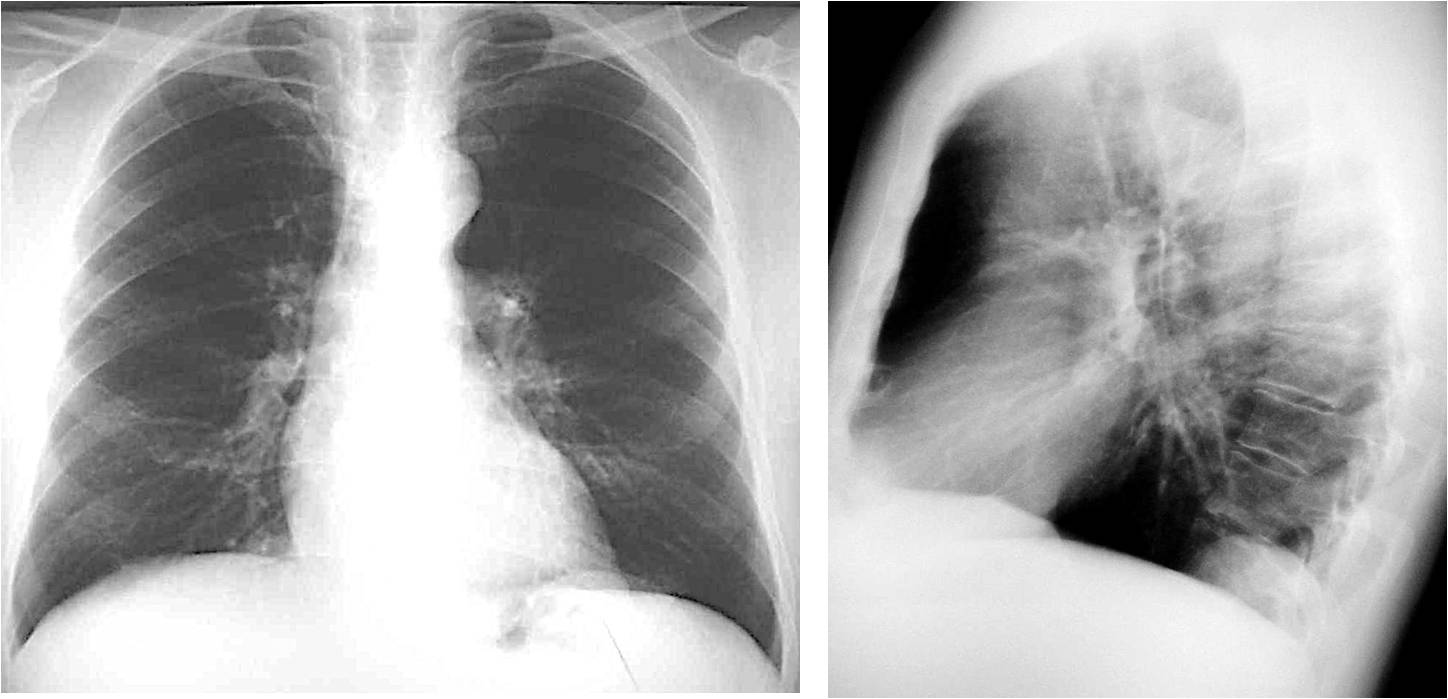
Today I’ll discuss the first question. Below you can see the chest radiographs of three different patients. Do you see any visible abnormality in any of them? Let me know in the comments section and come back on Friday for my answer.
First question: Is there any visible abnormality?
If you answered yes in all three cases, you’re right: Case 1 shows a pulmonary para-cardiac opacity (A, arrow), Case 2 shows a right mediastinal abnormality (B, arrow) and Case 3 shows a posterior extrapulmonary opacity (C, arrow).
Once an abnormality is found, the next step is to determine whether it is significant or not because this decision will influence our diagnostic approach.
We should mentally review the three main causes of non-significant findings:
1. Normal variants
2. Congenital malformations
3. Changes secondary to ageing
1. NORMAL VARIANTS
A number of normal anatomical variants may cause a confusing appearance on chest radiographs. It is important to know the most common ones to avoid mistaking them for pathology. Normal variants are well described in most textbooks and I cannot show them all here. As examples, I will cite two of the most common ones.
Case 1 is an example of a common normal variant: pectus excavatum (Fig. 1). It occurs in about 0.3% of the population and can cause findings of apparent cardiomegaly or blurring of the right heart border, simulating RML disease. In the PA view pectus excavatum can be suspected by the vertical path of the anterior ribs. The diagnosis is easily made in the lateral view.
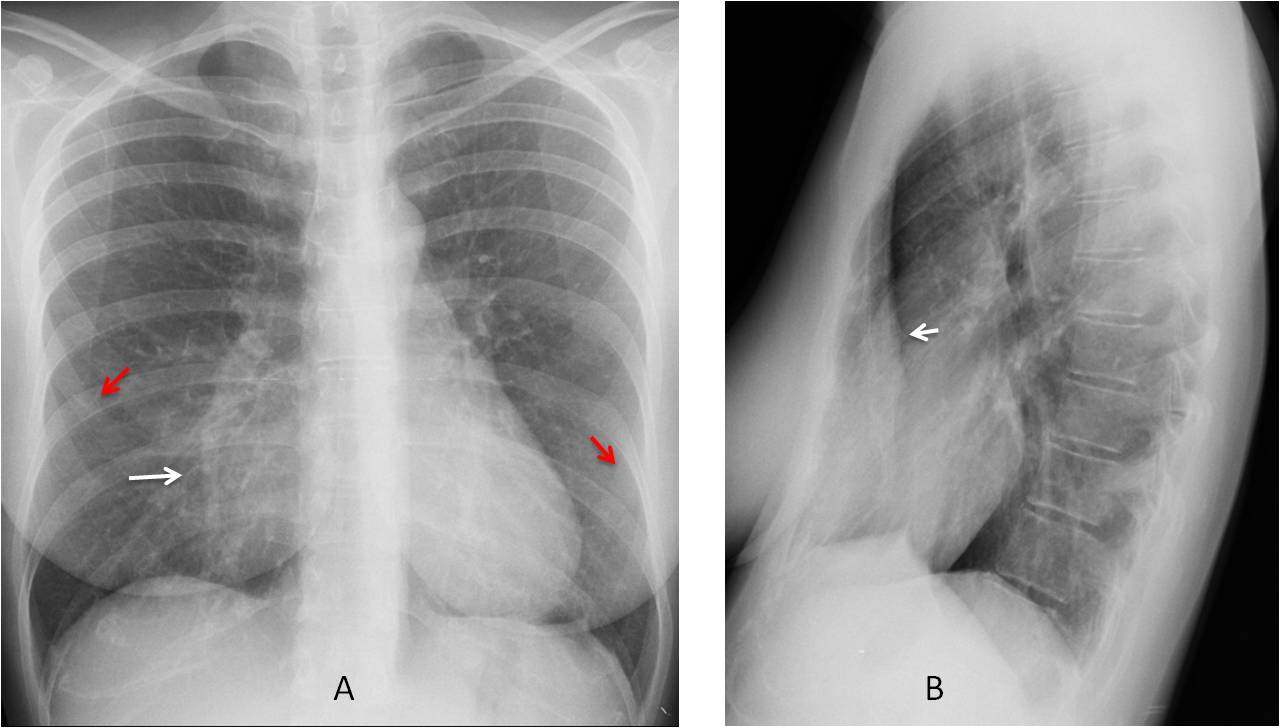
Fig. 1
Fig. 1: PA chest film shows an apparent opacity in the RML (A, white arrow). Note the vertical path of the anterior ribs (A, red arrows). The lateral view confirms that pectus excavatum (B, arrow) is the cause of the opacity.
Rhomboid fossa of the clavicle is another common variant that should be mentioned because it can simulate a lytic lesion, especially when it appears on only one side (Fig. 2). Rhomboid fossa results from the insertion of the costo-clavicular ligaments. It occurs in 30% of males and 5% of females and is more commonly seen in younger individuals, as it becomes less visible with age.
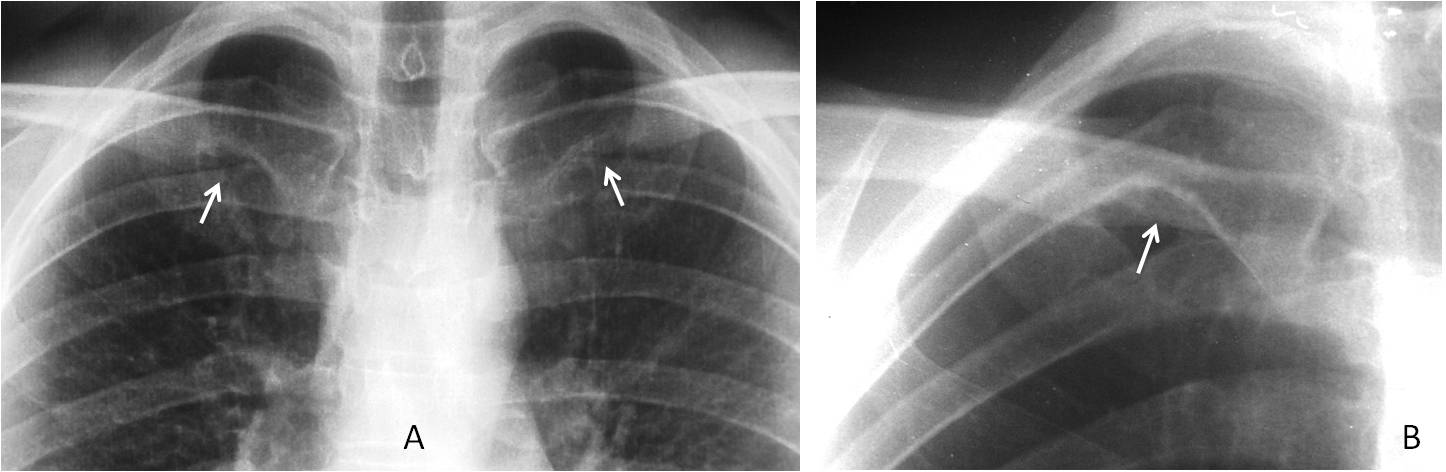
Fig. 2
Fig. 2: Examples of rhomboid fossa (RF) in two different patients. The first has bilateral RF (A, arrows), whereas the second has a single RF (B, arrow), which could easily be confused with a lytic lesion.
2. CONGENITAL MALFORMATIONS
Not uncommon in adults. It is important to be aware of these malformations because they may not be suspected in adult patients. Most are asymptomatic and easy to detect on chest radiographs if we aware of their existence.
Case 2 shows one of the most common congenital vascular malformations in adults: right aortic arch with an anomalous left subclavian artery (Fig. 3). It is asymptomatic and occurs in less than 1% of the population. Do not mistake it for a mediastinal mass or paratracheal lymph nodes.
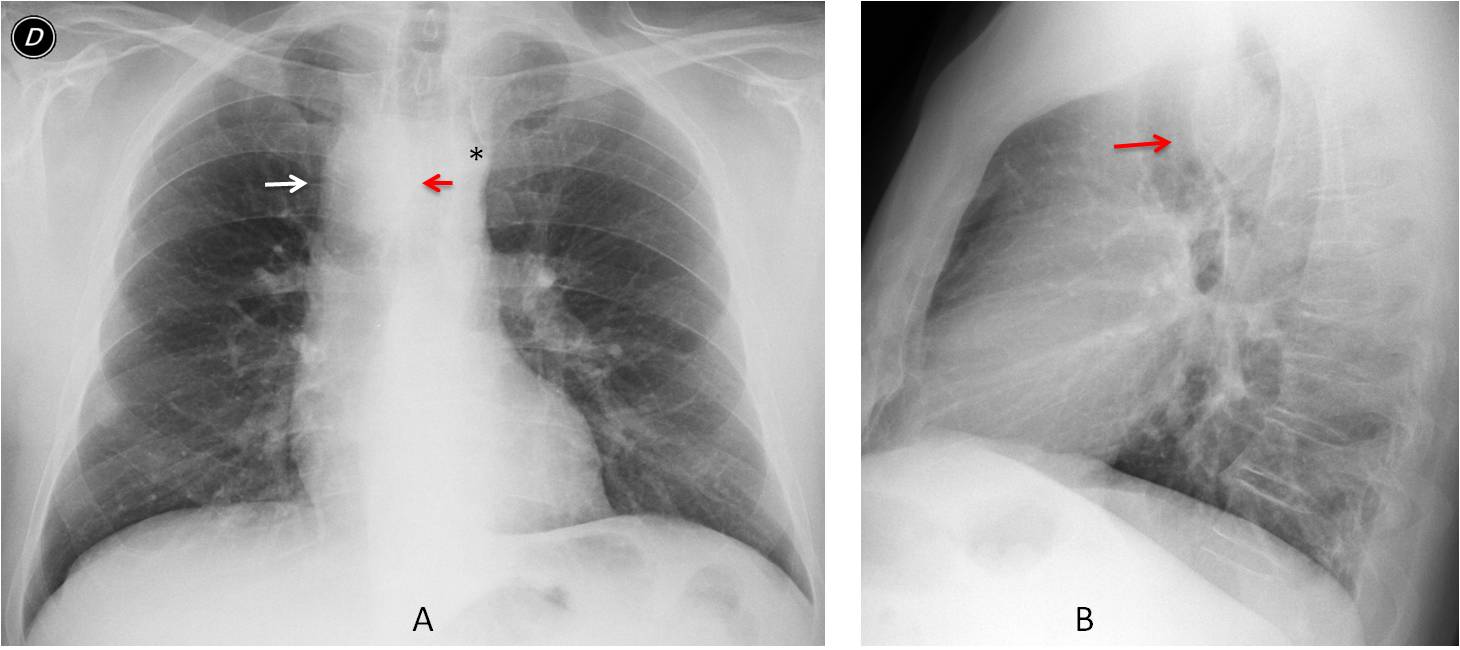
Fig. 3
Fig. 3: An apparent right mediastinal mass was found (A, white arrow) in this pre-op patient. The appearance is typical of a right aortic arch, with deviation of the trachea to the left (A, red arrow) and absence of the aortic knob on the left side (A, asterisk). The lateral view shows anterior displacement of the trachea by the posterior aortic arch (B arrow).
The diagnosis can be made with enhanced CT, but it’s cheaper to compare the image with previous films, which will show identical findings (Fig. 4).
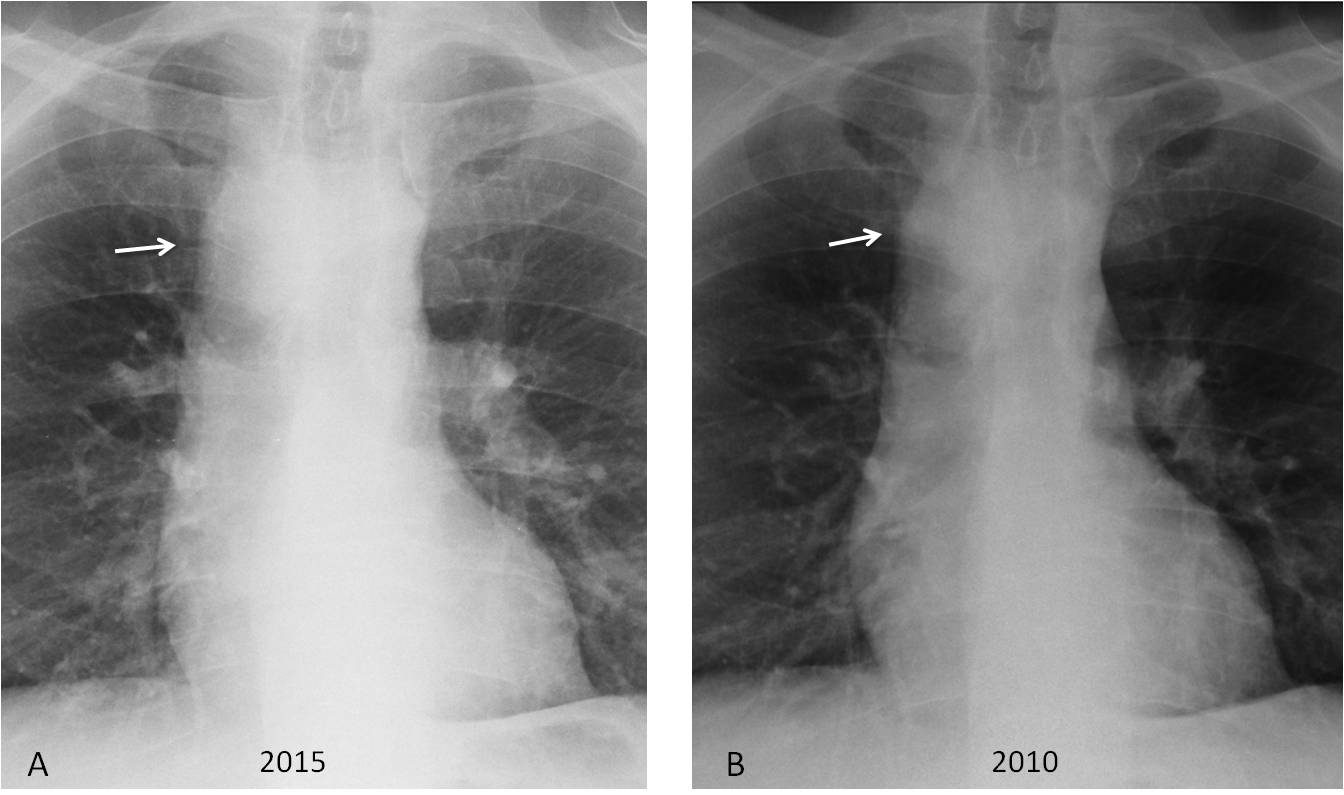
Fig. 4
Fig. 4: (same patient as Fig. 3). PA chest film taken five years earlier shows identical findings. The right aortic arch remains unchanged (A and B, arrows).
Many congenital malformations involve the lung. Most are asymptomatic and are first discovered in the adult age. Some of them were reviewed in Dr. Pepe’s Diploma Casebook Case #73. One of the most common is hypogenetic right lung (scimitar syndrome), which gives the chest radiograph a bizarre appearance (Fig. 5).
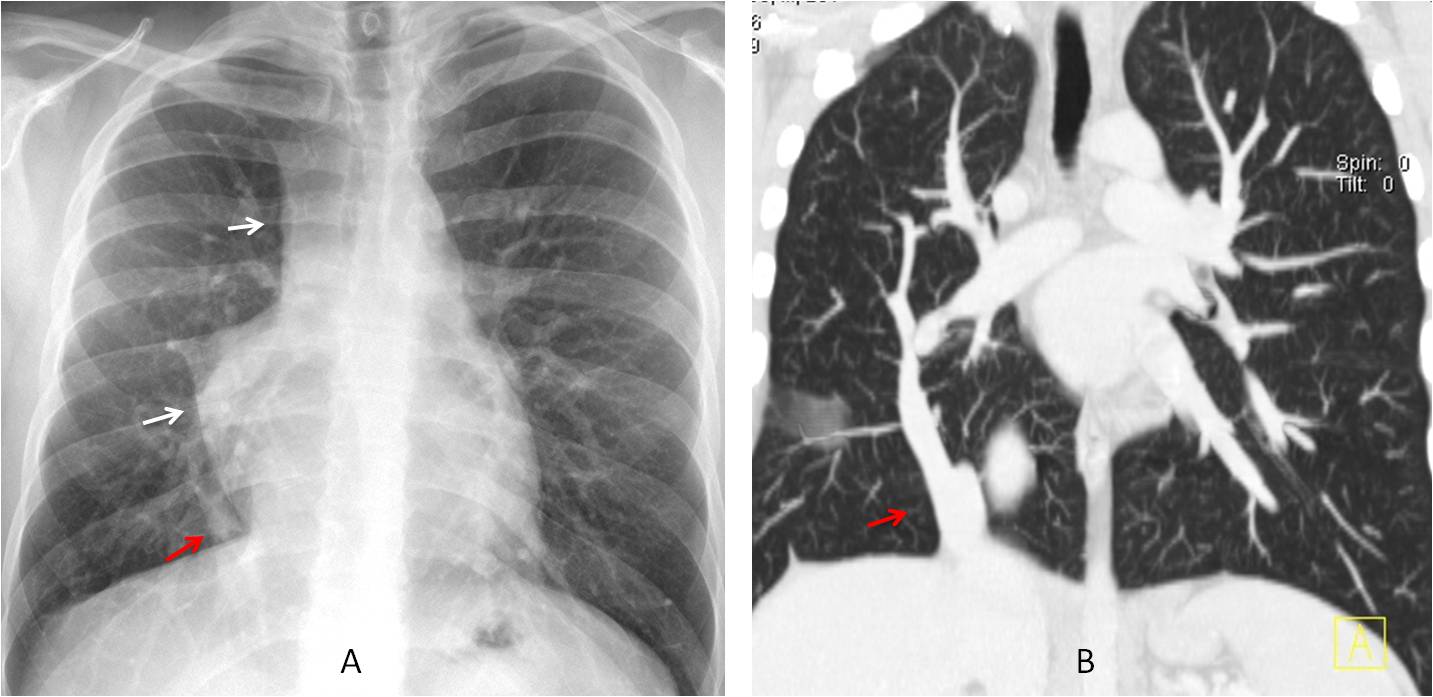
Fig. 5
Fig. 5: Hypogenetic right lung showing an abnormal mediastinal contour in the PA chest film (A, white arrows). Coronal CT shows a smaller right lung and the scimitar vein (A and B, red arrows), which is typical of this malformation.
3. CHANGES WITH AGEING
As we get older, morphologic and physiologic changes occur (aortic elongation, kyphosis, etc.) that alter the appearance of the chest. We should be familiar with the various changes that occur in the elderly chest to enable their differentiation from pathological conditions.
CASE 3 is an example of a normal occurrence in older persons: Bochladek hernia (Fig. 6), secondary to weakening of the muscle fibres of the diaphragm as a consequence of ageing. It creates bumps in the diaphragm that should not be confused with disease.
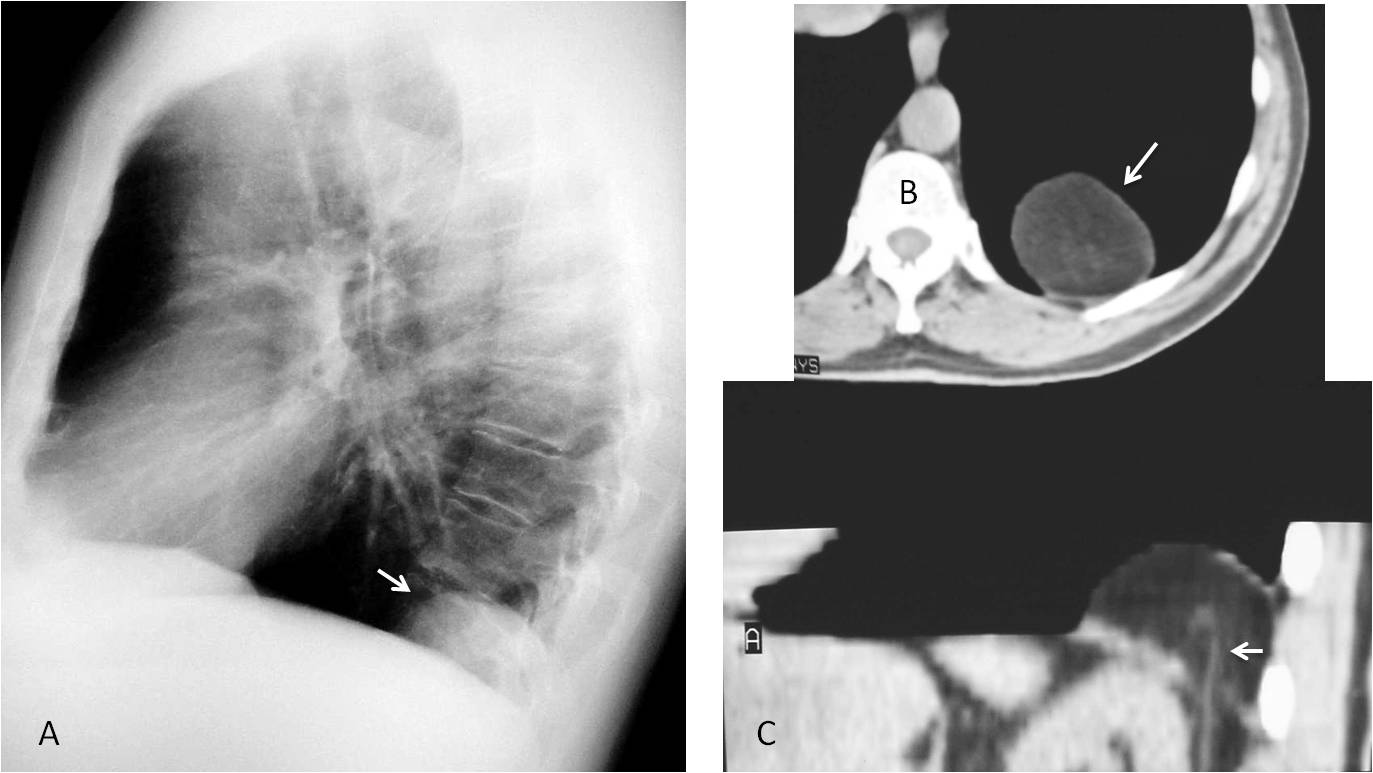
Fig. 6
Fig. 6: Bochladek hernia in a 65-year-old man, simulating a posterior mass (A, arrow). Axial CT demonstrates the fatty component (B, arrow). Sagittal CT demonstrates the rent in the diaphragm and a crossing abdominal vessel (C, arrow).
Calcification of the mitral annulus occurs in about 10 % of old persons, and is usually very obvious in the chest radiograph (Fig. 7). It should not be confused with calcium in the valve. Usually asymptomatic, it can occasionally cause mild valve dysfunction.
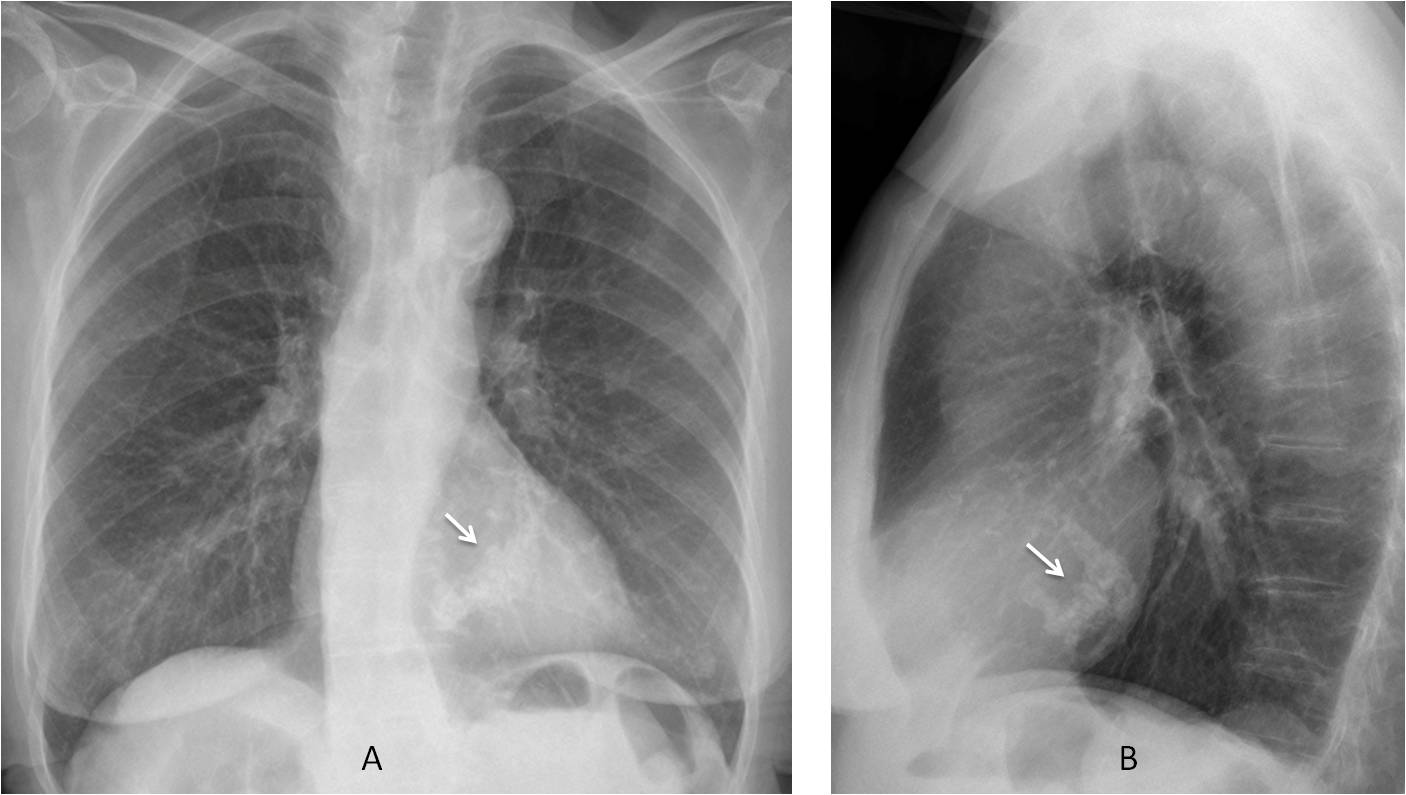
Fig. 7
Fig. 7: Calcification of the mitral annulus in a 78-year-old woman. Note the typical reversed C-shape of the calcium (A and B, arrows).
In conclusion, the first step when looking at a chest radiograph is to determine if any visible anormality is present.
If an abnormality is detected, our next concern should be to exclude a non-significant finding to avoid an unnecessary (and costly) work up. To do that, we should be familiar with the most common normal variants and congenital malformations, as well as the appearance of the chest in persons of advanced age.

Dr. Pepe’s Teaching Points
Your first step when looking at a chest radiograph is to detect visible abnormalities
When abnormal features are present, exclude the following:
– Normal variants
– Congenital malformations
– Changes secondary to ageing


Hello after holiday
In 2 case there is round nodule projecting over anterior part of right VI rib.
In 3 case there is obvious well circumscribed lesion in left lower lobe laying on diaphragm.
In case 1 I cant find abnormality.
Greetings
Welcome back!
Hello professor!
In case 1 there seems to be blurring of the right cardiac border. It could be middle lobe consolidation, but pectus excavatum may also give this appearance. A profile x-ray might help.
In case 2 I see a nodule projected on the lower third of the right lung, at the level of the 8th rib (posteriorly), or 6th rib (anteriorly). It is round, well circumscribed and could be pulmonary. It could be a nipple, too, although I don’t see anything on the other side. Maybe some more radiographs with nipple markers might help, or we could go straight to CT.
In case 3 there is a lesion located in the posterior costophrening angle, possibly retrocardiac. Maybe a small Bochdalek hernia? Could be a lung tumor or pleural lesion as well. Moreover, it seems to me that the lungs are somewhat radiolucent, especially the left one. And I think there is a little hyperexpansion with elargement of the retrosternal clear space. Maybe COPD?
Have a closer look to case 2
In case 2 I’d add a right paratracheal lesion.
Additionally to the comment of Mauro I would describbe a prominent right-sided mediastinal contour, possibly of vascular origin. I do not think that the x-ray is significantly verrotated because the trachea is in the midline. It could be an anomaly of the aortic arch, maybe a right-sided aortic arch. In the differential list would be coarktation.
Best greeting.
in case number 2 of course
Good thinking
Case 1. Right cardiac silhouette is missing, probably because of something at medial lobe, such as consolidation. Pectus excavatum will be a good option too.
Case 2. Peripheral nodule at right inferior lobe, and probably a partially calcificied nodule next to left hilum. Thickening of right paratracheal line.
Case 3. Something proyected over lower posterior mediastinal.
Good morning, profesor:
Case 1: we can’t define cardiac border correctaly, maybe because the heart is rotated by a pectus excavatum. We don’t think there is consolidation.
Case 2: We think there is a right mediastinal bulging with extension to right paratracheal stripe. Vascular anomaly? Maybe there is no connection with the history of leg fracture.
Case 3: We see a mass with pleural base posteriorly, possibly related to a hernia.
In the first case, blurring vision of the right cardiac border may suggest pectus excavatum, lateral view is advisable.
In case number 2 there is a right para tracheal dense shadow with loss of the left aortic knob may represent right sided aortic arch, in addition to the the presence of a dense nodule in the right lower lateral zone ? metastases.
In the third case what I see is mild hyperinflated lungs specially upper and mid zones with reduced pulmonary vascularity, the presence of large emphysematous bullae is a possibility, while that radiodense structure in the posterior left para spinal region; I see the posterior left hemi diaphragm is continuous so I do not think its a hernia, so it could be a nerve sheath tumour,, thank you
1st case – pectus escavatum with concomitant changing of CXR appearance maybe consolidation of RML…need lateral view.
2nd case – amputation of right hilum possible pulmonary embolism with enlargement of the upper mediastinum, may be vascular – check CT 🙁 or RX.
3rd case – pulmonary scleroemphysema with a postero-basal ( LLL ) diaphragm opacity that might be either a transdiaphragm hernia or a fluid collection
1 pectus excavatum
2.right dose mediastinal widening maybe basilar abnormality
3. Bohdalik hernia
In case 1 I would like to see the lateral view, because the right border of the heart might be slightly out of place, this could be due to wall deformity (pectus excavatum).
Case 2 there is an increased density and enlargement of right paratracheal space although I can´t see tracheal displacement neither the aortic arch where it should be seen. This might be a vascular anomaly (Aortic arch developmental anomaly).
Case 3 there is a round lesion seen in both projections and my best guess here is a diaphragmatic lobulation in the posterior left diaphragm.
Dear friends, thanks for participating. Most of you gave the right answers (cases were not too difficult, really 😉 ).
See the discussion tomorrow and look at next week’s case. It is interesting.
[…] you may remember from Diploma Case 94, when I’m facing a chest radiograph I start by asking three […]
[…] Is there any visible abnormality? (Chapter 1) b) Is it intra or extrapulmonary? (Chapter 2) c) What does it look […]
[…] that we’ve looked at the three key questions to ask when facing a chest radiograph (chapters 1, 2 and 3), we move on to the interpretation of pulmonary […]