José Vilar and Friends Case 37 (Update: Solution + Teaching cases)
Good day Friends,
From Hospital Universitario Dr. Peset ( Dr Edgar Lorente).here is a case to test your ability to catch important findings.
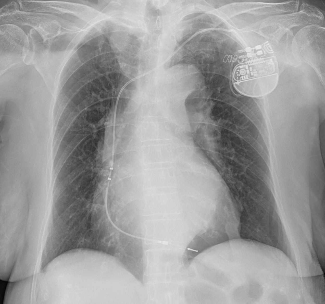
This is a 55 year old man that comes from the cardiology clinic. What would you report or do?
Additional information:
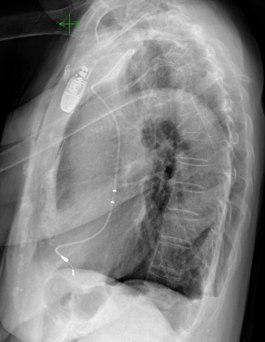
This is a lateral projection, always important as you know…
Do you see the pathology now?
Click here for the answer
OK colleagues, thank you for your participation. This time you were not too close to the diagnosis. Although I told you that the patient was coming from the cardiology clinic, I must say that she just had, a couple of hours before, a pacemaker implanted, and, as I told you later, she had chest pain.
Now let’s look at the images.
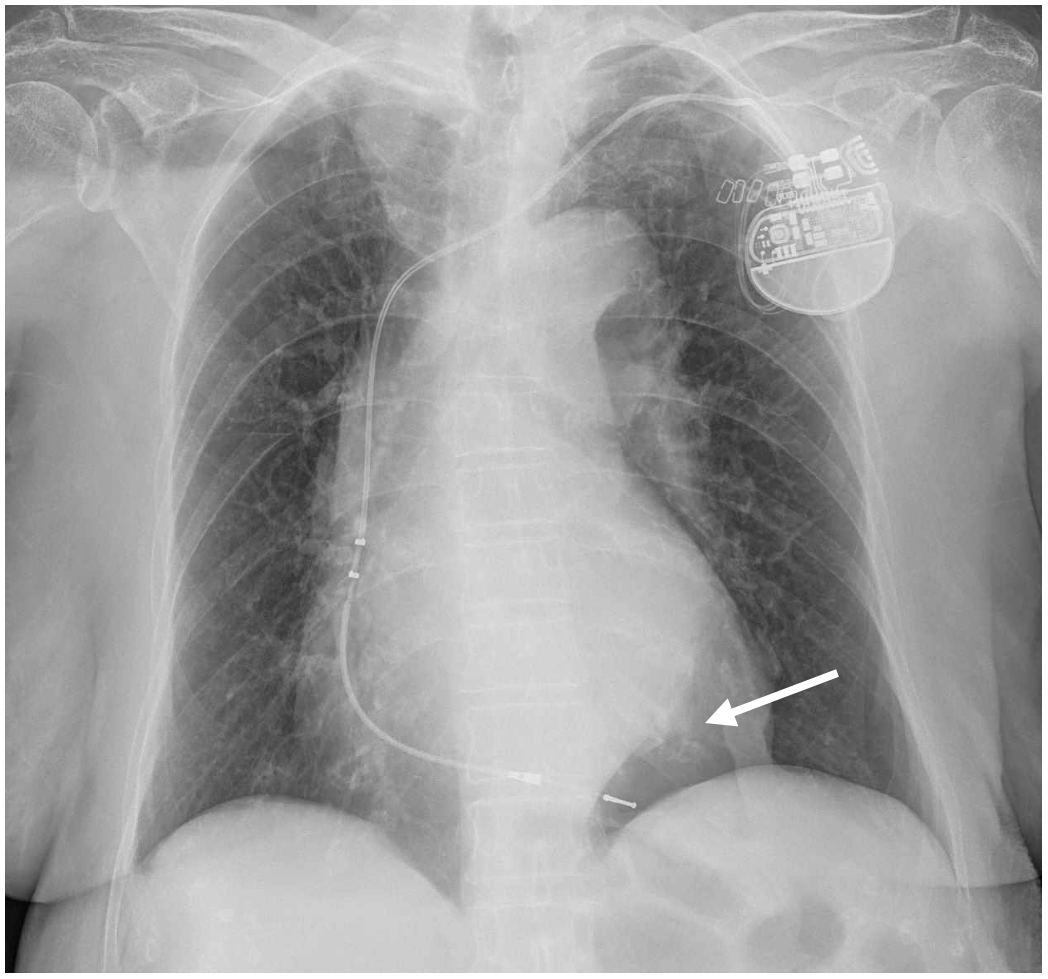
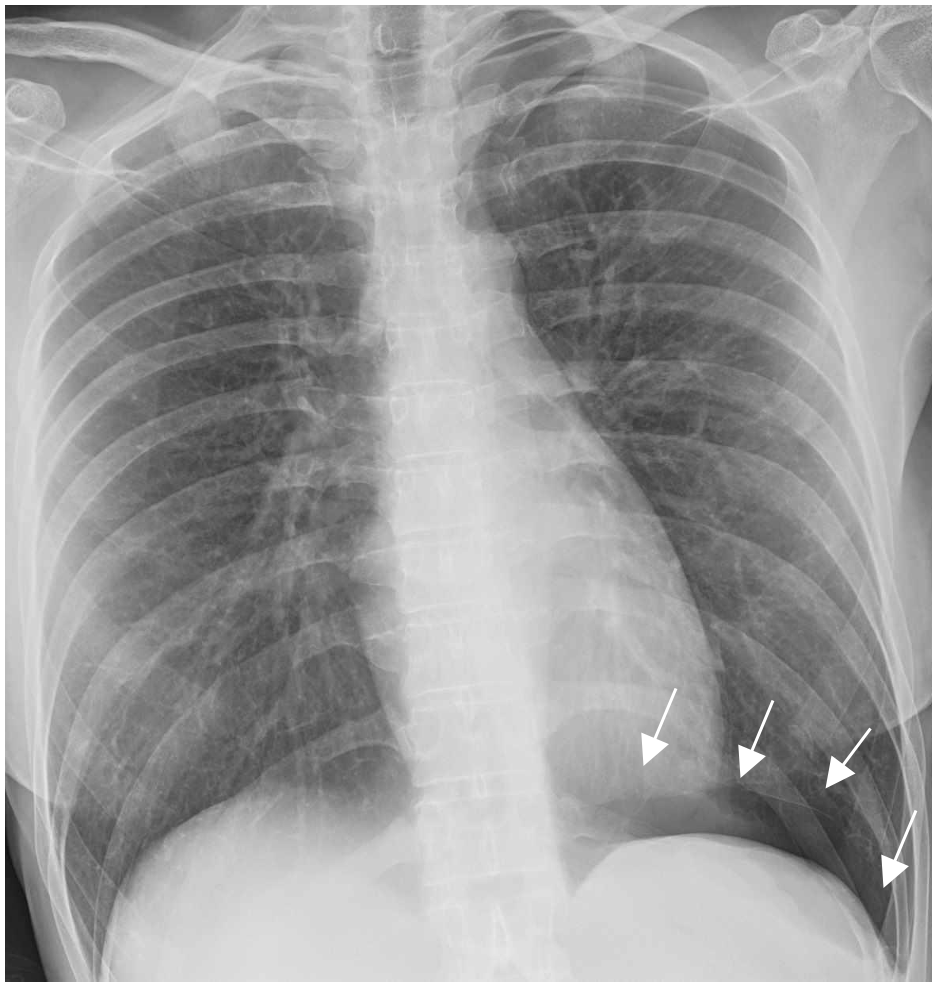
In the frontal view there is an obvious elongation of the aorta and branches and a pacemaker has been placed through the left side. The ancillary finding is the black area under the left ventricle (white arrow) with no vessel markings.
If you look at the lateral view you see (blue arrow) this air density outlining the left ventricle. It is worth to note also that the definition of the heart borders is quite sharp. There is a small air fluid level in the posterior left costophrenic angle (blue thin arrow).
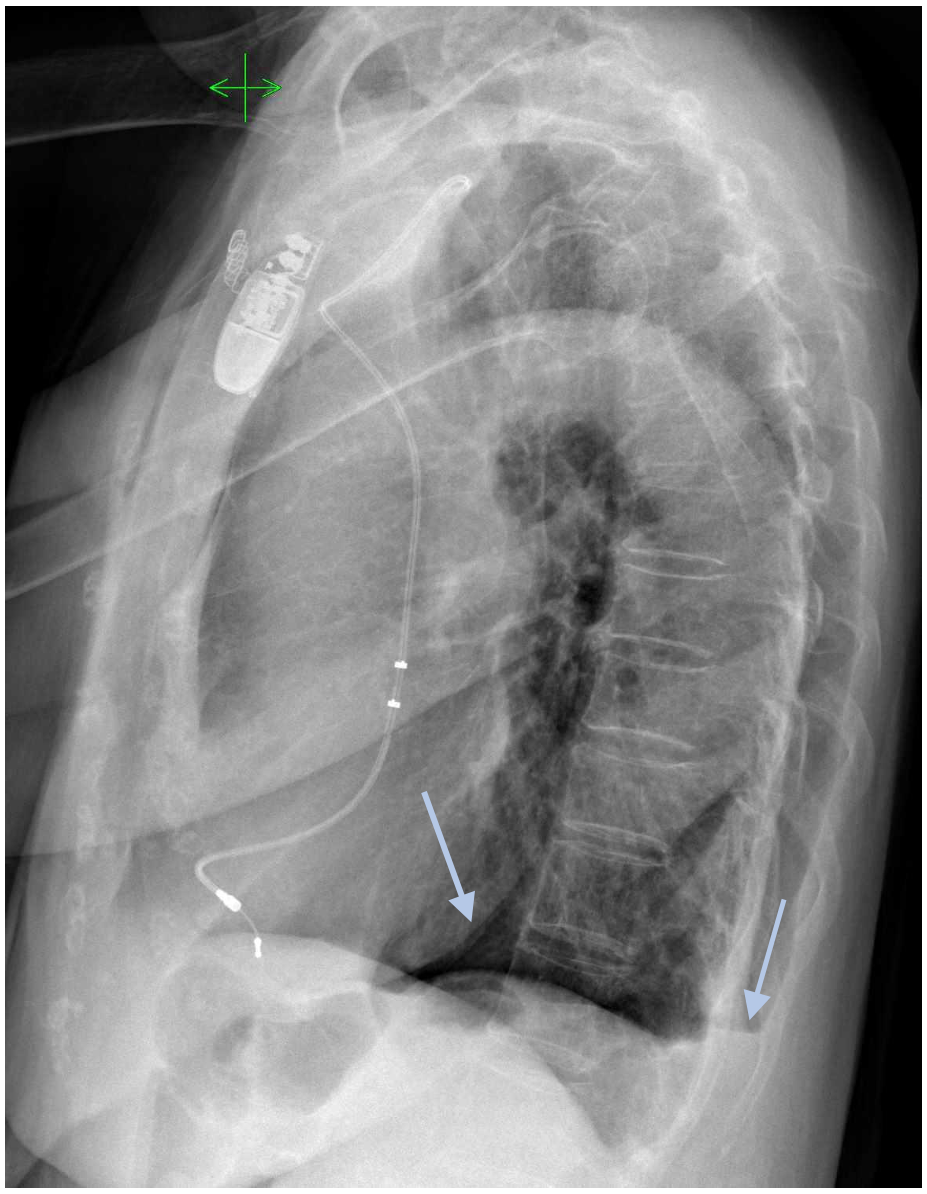
The presence of abnormal air in the chest after a pacemaker placement in a patient that refers chest pain must raise the suspicion of pneumothorax.
Bubbles of air in the pleura may sometimes appear below the heart and may be hard to see, especially in portable radiographs when the patient is supine. (In our case the patient was upright.)
DIAGNOSIS: PNEUMOTHORAX
Comment: It is very important to identify the presence of air in the pleura, especially after the patient has been submitted to invasive maneuvers in the chest.
To detect some pneumothoraces you must look for abnormal air densities with sharp definition of the nearby mediastinal structures. You should be especially aware of this possibility when reading portable radiographs.
Two other examples:
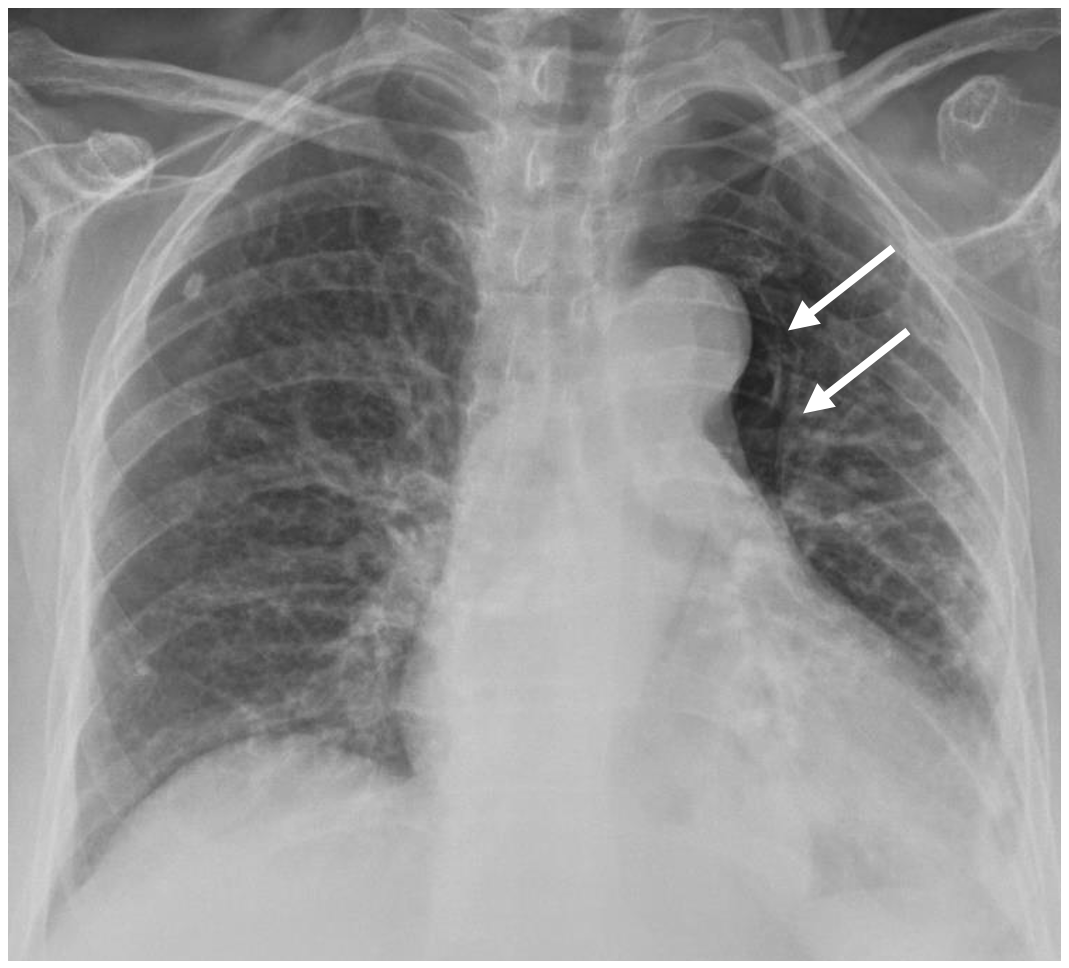
Case 1: Here is a case pneumothorax in an unusual location shown to me by Dr. Carmen Bodlak M.D, a young resident from Hospital Universitario Dr Peset. This patient had a needle biopsy of a pulmonary nodule and developed a small pneumothorax seen in this supine AP projection as a paramediastinal air collection. (Arrows).
Case 2: Supine radiograph in a case of spontaneous pneumothorax with a sub pulmonary location (arrows). See how the diaphragm is very sharp and the costophrenic angle is marked (deep sulcus sign).


The patient has chest pain
Greetings, this is my first time posting here, credits for nice cases 🙂 I am still quite at the beginning of my path, so I will be brutally honest and say I can’t help myself with the lateral projection, the only thing I see is that the part above the aorta is completely mottled.
What bothers me on the PA projection is the superior mediastinum and especially the right apex.
Would recommend a chest CT.
PA CXR shows increased cardiothoracic ratio with prominent aortic knuckle.
Lateral film shows prominent/dilated aorta..
case of aortic aneurysm???
Anuerysmal dilatation of aorta
I think, fracture of pacemaker lead And ascending aorta aneurysm and right plural effusion. (Please clinically correlate to rule out complicated dissecting aneurysm)