José Vilar and Friends Case 42 (Update: Solution!)
Dear friends,
We embark today in a case less focused in finding a radiologic sign and more in a clinical context, but, of course from the imaging point of view.
This case provided to me by Dr Ruben Ruiz, a senior resident and Dr Santiago Isarría already known in this blog, both from Hospital Universitario Dr. Peset in Valencia. Spain.
This is a 52-year-old woman with Lupus erythematosus and a history of cervical cancer treated with radiation therapy.
The lady complains of right chest pain at deep inspiration.

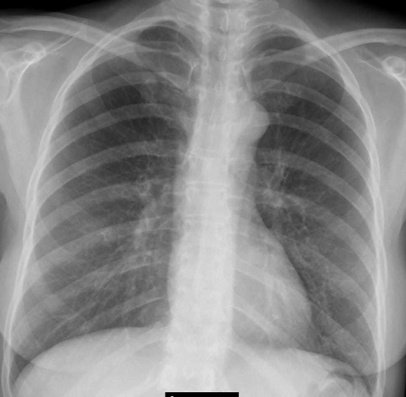
Previous Chest radiograph seven months before
What do you think? Please give me a differential diagnosis and I will provide you later with additional images.
Update: Additional Images
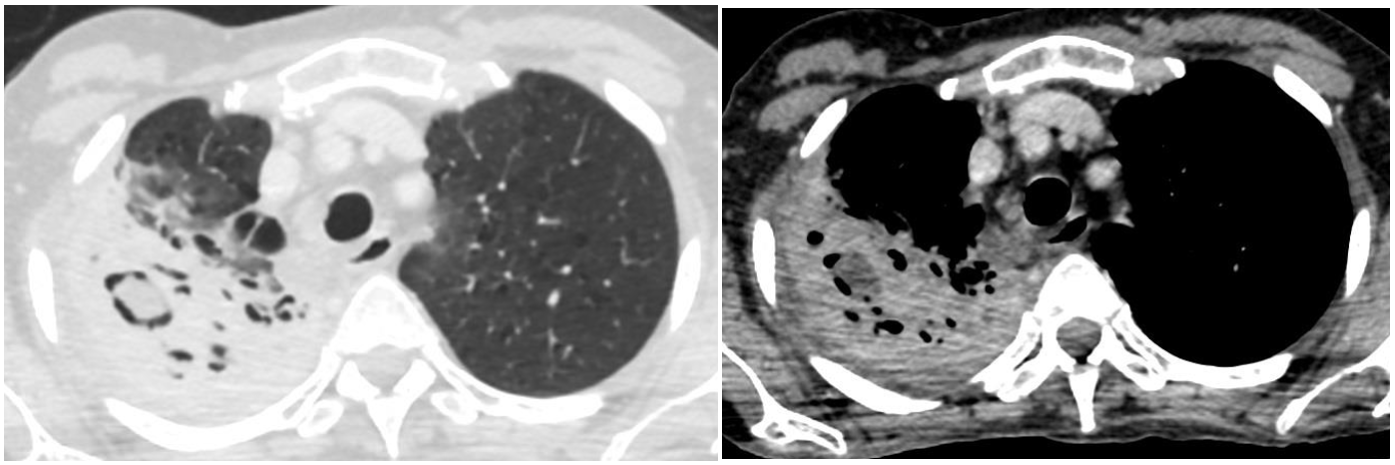
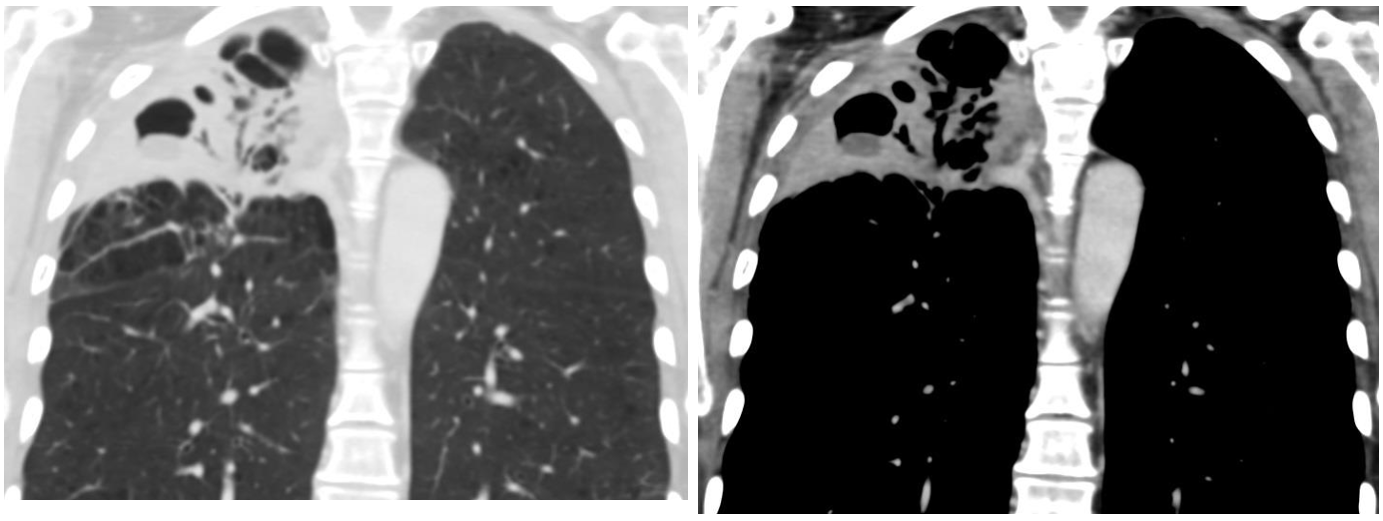
Here are some CT images. Although tuberculosis was suspected this was discarded after a thorough investigation.
Click here for the answer
This case was very well read by some of you, especially Anasthasia who did mention the diagnosis and the differential, and also Marcos. Well done.
Let us see what where the findings:


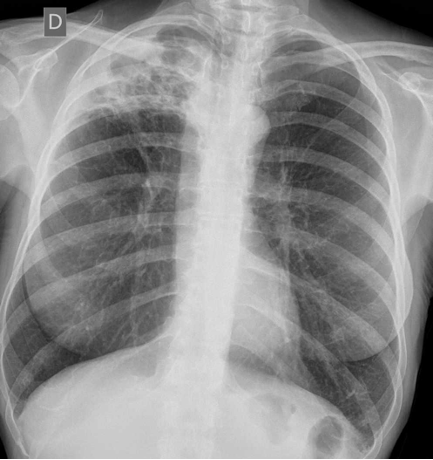
We have a study withy PA and Lateral projections showing an opacification of the right upper lobe with some loos of volume since the right hilum is elevated. The findings are better understood by looking at the radiograph obtained seven months before where there is no pathology in the right upper lobe and the hilum is in the normal situation.
The findings should make us think about an infectious pathology, being tuberculosis the first choice as Marcos indicated.
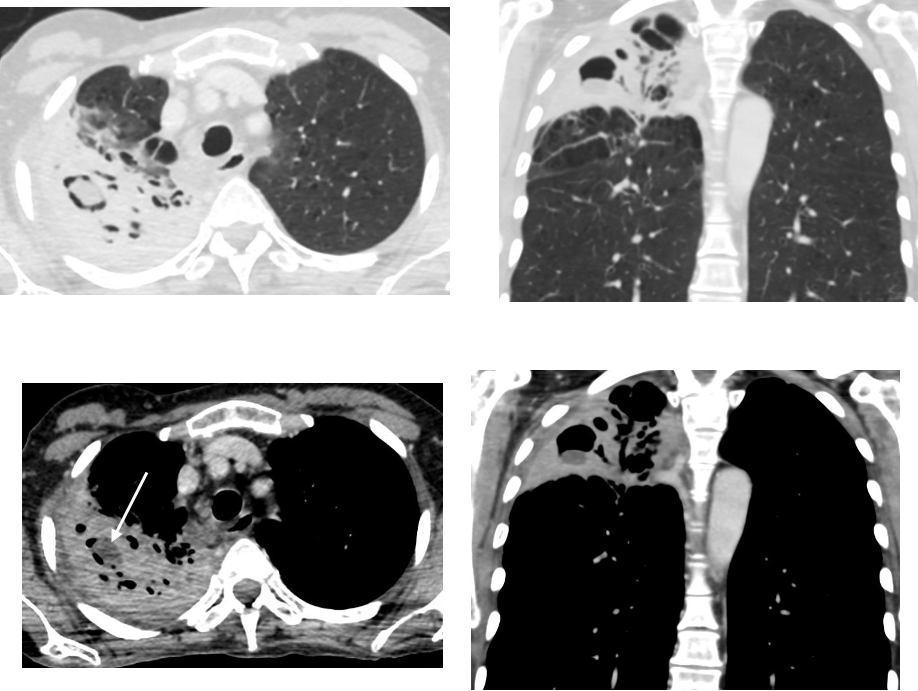
A CT was obtained and the findings confirm the presence of a right upper lobe consolidation with multiple areas of cavitation, air bronchograms and a larger cavity containing a hypodense nodular image. (Arrow). This lesion is not gravity dependent (remember that CT is supine).
Once Tuberculosis was discarded the other most probable diagnosis was Semi invasive Aspergillosis.
This entity develops in patients with a mild immunosuppression such as diabetes, chronic steroid therapy, alcoholism..
The main features of semi invasive aspergillosis are related to the presence of necrosis (it is also called chronic necrotizing aspergillosis). Necrosis forms cavities and nodular hypodense areas such as the nodule in this case. This is not to be confused with an aspergilloma floating in a cavity that should have a higher density and be gravity.
dependent. Other findings may be thickening of the bronchial walls and pleura
The diagnosis (serological or sputum) can be obtained detecting with fungus cultures, with the galactomannan antigen (GA) , or by means of molecular biology (PCR rt). The bronchial aspiration material of our case revealed a positive GA ( <0,5) confirming the diagnosis of aspergillosis. Additionally, another opportunistic agent; candida albicans was also detected.
Points to remember:
- Aspergillosis occurs in patients with severe immunosuppression but also in other with mild immunosuppression.
- Radiological signs of semi-invasive aspergillosis may be easily confused with tuberculosis
- Again, remember the role of the chest radiograph and the value of previous images.


Upper lobe consolidation with some radiolucencies and volume loss. It could be radiation induce lung fibrosis but also an infection cause, more if is recieving inmune suppressive treatment like a tuberculosis reactivation with cavitation.
The third a usual lobar pmeumonia in a fibrotic upper lobe because of the radiotherapy
I just saw that 7 month earlier the upper lobe seems ok. So my first choice is tuberculosis
THERE IS PARENCHYMAL FIBROSIS, WITH SMALL CYSTIC LUCENCIES AND PLEURAL THICKENING CONFINED TO THE RIGHT UPPER ZONE- CONSISTENT WITH RADIATION PNEUMONITIS, FIBROSIS AND PLEURAL THICKENING.
THE RIGHT HILUM IS NORMAL- NOT ELEVATED, NOR ANY HILAR NODES OR MASS TO SUGGEST TOTAL RIGHT UPPER LOBE INVOLVEMENT.
THE REST OF THE LUNG FIELDS AND COSTOPHRENIC ANGLES ARE NORMAL.
THE PATHOLOGY CONFINES TO THE RADIATION PORT OR AREA ONLY
Consolidation with radiolucent areas located at the apical segment of the right upper lobe. The right hilum & the horizontal fissure are pulled towards the lesion. I would probably say that there is also peribronchial fibrosis.
It could be necrotizing pneumonia, pulmonary tuberculosis or necrotizing bronchopulmonary aspergillosis.
Ok. Most of you are in the right track. I am going to add some more images and I will then expect a diagnosis.
Aspergillus?
right upper zone collapse and shift of mediastinum towards right and elevation of right hilum. Areas of lucencies in the collapsed right upper zone. lateral radiograph suggests posterior and apical segment of right upper lobe involvement. same is confirmed on ct scan. ct scan also reveals a thick walled air filled cavity and some dependent hypodensity within with air crescent sign. diagnostic possibility of infectious etiology like fungal ball. patient has lupus so should be on immunomodulators plus last radiograph is normal. my 1st differential will b infectitious
Right upper lobe consolidation with cavitation, slight upward elevation of the right hilum, central mediastinum, no hilar LNs.
DD:
1-pneumonia? Nocardia.
2-Fungal infection.
3-less likely, lupus pneumonitis as it is more aggressive course clinically and affects more lung base
However, radiation-induced pneumonitis usually happens after radiation to chest maligancy.
Necrotising pneumonia due to opportunistic infection most probably caused by Aspergillus or Staphylococcus aureus.