José Vilar and Friends Case 44 (Update: Solution!)
Hello everybody!
Let me show you a case from my file- A case that may teach something about chest radiography.
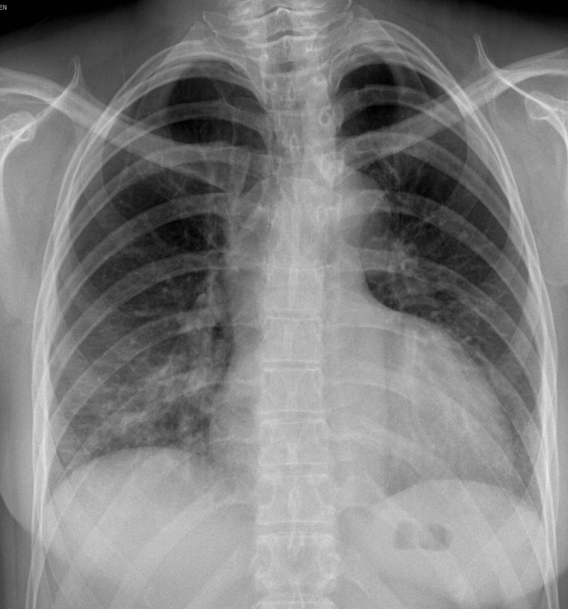
This is a 30-year-old woman, radiology technician, with a recent pneumothorax. ( “rule out pneumothorax ”).
How would you read this image?
Additional information:
Here is a radiograph obtained 5 minutes after the first one.
Can you explain what happened?

The explanation of this peculiar case next week…
Click here for the answer
This case is a bit tricky, but reflects something that may happen in real life. Indeed it happened to me when I was confronted with this chest radiograph of one of our technicians.
My first impression was that it was a different patient. When I was assured that it was really her, and knowing that she had a history of pneumothorax. In fact this was a case of catanemial pneumothorax (recurrent episodes of pneumothorax coinciding with menstruation ). I asked if this radiograph had been obtained with forced expiration. Yes, this was an expiratory radiograph, and this is the clue as was very well indicated by Dr.Doukopoulou (congratulations Anastasia for this!).

This PA chest radiograph shows an enlarged and deformed cardiac silhouette, linear markings and increased density in the lower lung fields.

All the apparent pathological signs disappeared in the PA radiograph in full inspiration obtained immediately.
Diagnosis: False cardiac and pulmonary pathology due to forced expiration
Why do I show this case? For several reasons:
- Chest radiographs should be obtained in deep inspiration except when we want to reveal air trapping in cases such as foreign body aspiration(in a child especially) or to detect tension pneumothorax. It was once used to assess the size of a pneumothorax the rationale being that an expiratory radiograph would better identify and measure the amount of pleural air, but several authors have demonstrated the low value of this technique as compared to the regular inspiratory chest radiograph, or Ultrasound.
- Very often, chest radiographs are not obtained in full inspiration and, as in this case, the heart may appear larger and the lung vessels loose definition. This occurs frequently in portable AP radiographs.
- Also, in CT, respiratory maneuvers are also used for different reasons, namely to detect air trapping and to detect tracheo-bronchial abnormalities.
- In both, radiographs and CT, respiratory maneuvers may alter the pulmonary structures. The changes in the interstitial pressure versus alveolar pressure in the lung modify the size of the vessels and other pulmonary structures, including pathology.
This is important as shown in this example from Alexander Bankier and colleagues in which a pulmonary nodule changes in size and morphology between inspiration and expiration (See how the posterior tracheal wall is flat in expiration)
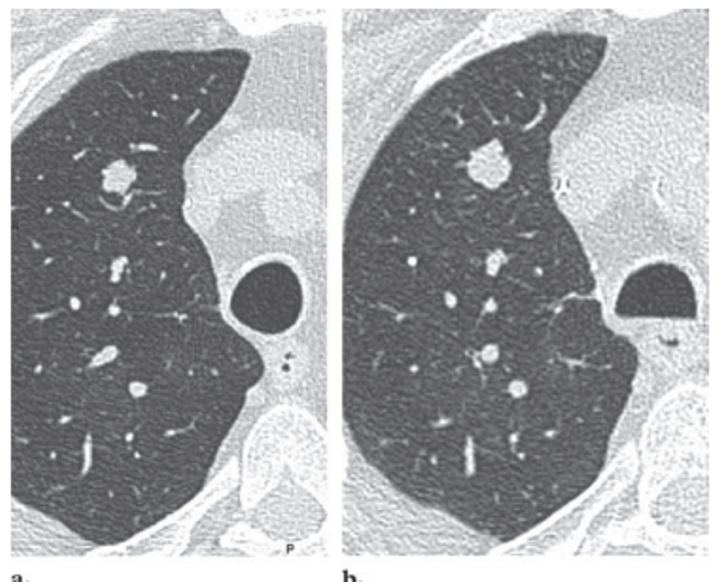
(from Bankier et al Radiographics 2008. (28) 919-931)
Points to remember:
- Forced expiration may alter significantly the cardiac shape and size and the lungs in a chest radiograph, and is a cause of diagnostic errors.
- Expiratory images may be useful to detect air trapping in the lungs, but not in evaluating pneumothorax.
- If expiratory images are obtained the technician should always indicate it in the images.


Gas superior mediastinum. ? Pneumomediastinum, dilated oesophagus
I can see that many people are looking at the case but only Samad Punekar has dared to say something. Well, this is a tricky case. No Samad there is no mediastinal pathology. In fact the patient is absolutely asymptomatic.
POSTURAL TILT
SCOLIOSIS
PARENCHYMAL CHANGES- VERY SMALL CYSTS IN RIGHT LOWER ZONE
SEPTAL THICKENKING
VISCERAL PLEURAL LINE IN RT UPPER ZONE PERIPHERY WITH MORE LUCENCY
A LATERAL VIEW CHEST IS DESIRABLE TO RULE OUT SOLITARY COLLAPSE OF VERTEBRAL BODY D5 OR D6—TO RULE OUT HISTEOCYTOSIS , SPONTANEOUS CLOSED PNEMOTHORAX
APPARENT CARDIOMEGALY
PROMINENT AORTIC OUTLINE
CONCAVE MPA
The second x ray shows hyperventilated lung fields both sides but the radiolucency is more on right side.
there is herniation of right upper lobe to the left with shift of ant mediastinal stripe to left side.
deep sulcus sign rt cp angle
more lucency over the rt dome
cardiac shift to left
gastric air shadow does not show fluid level suggesting supine projection
dorsal vertebra d5 appears compressed
are we dealing with pnemothorax in supine view or loculated more anteriorly
Now that we have the additional x-ray we can suspect that the first x-ray is expiratory (in order to detect a small pneumothorax), thus the cardiac silhouette appears enlarged and there are spurious basal opacities. Also, there is a linear oppacity at the right apex parallel to the mediastinal pleura.
The additional image shows a radiolucent area at the right lung apex that projects towards mediastinum.
I would say that most probably is an apical bulla with herniation and less probably a loculated pneumothorax.