José Vilar and Friends Case 46 (Update: Solution+Correction!)
Dear Friends,
This is a case that was provided to me some time ago by Dr Javier Lucaya, a superb pediatric radiologist from Barcelona.
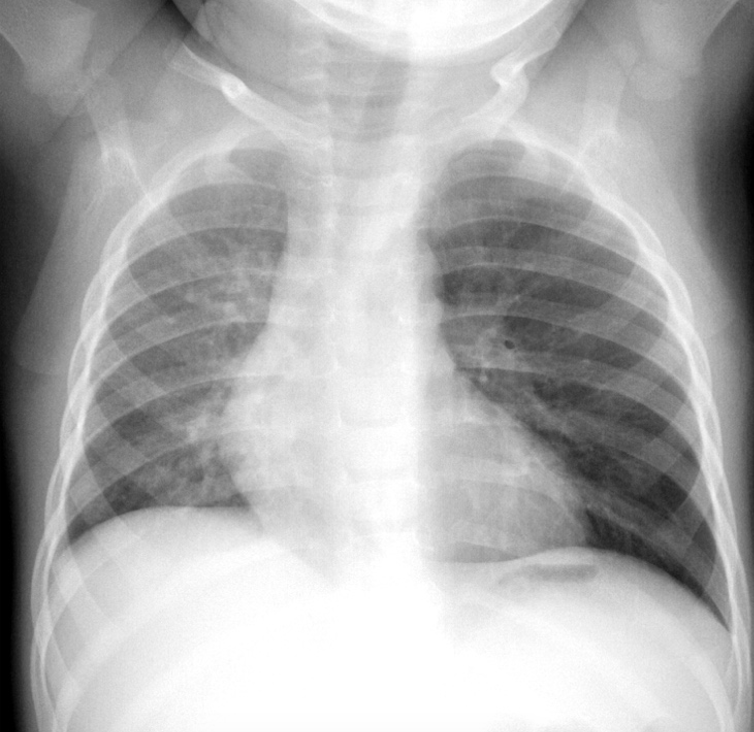
A two year old with acute severe cough.
What do you think and what would you do?
Update:
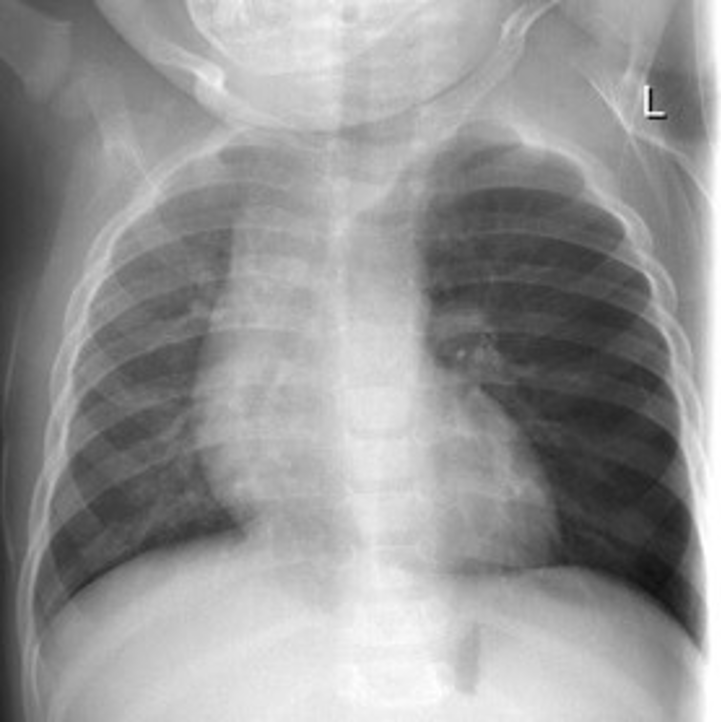
Here is the expiratory radiograph.
Two questions:
- How did we manage to obtain this radiograph?
- Is the diagnosis clear now?
Click here for the answer
Edit: The original solution from yesterday contained a couple small mistakes that have now been corrected.
Hello everybody.
Many of the brave participants thought about the correct diagnosis: Foreign Body aspiration, and some correctly indicated how to proceed with expiratory images. Dr Kanakaraj pointed out the lateral decubitus. Good job!
These are the following findings in our case 46 that, as I indicated, was provided to me by Dr Javier Lucaya from Barcelona:
There is a clear difference in density of both lungs. The left lung is darker. This could raise several possibilities: Hyperlucent lung in Swyer James McLeod, Emphysema, Pneumothorax, absence of pectoral muscles or air trapped due to a bronchial obstruction. The first two possibilities are discarded, since there is an increase of volume of the left lung, and the soft tissues are symmetric. There are no signs of Pneumothorax, the lung vessels are stretched but well seen. But the most important data in this case is the clinical scenario: acute respiratory symptoms in a child.
This is why it it is crucial to demonstrate air trapping.
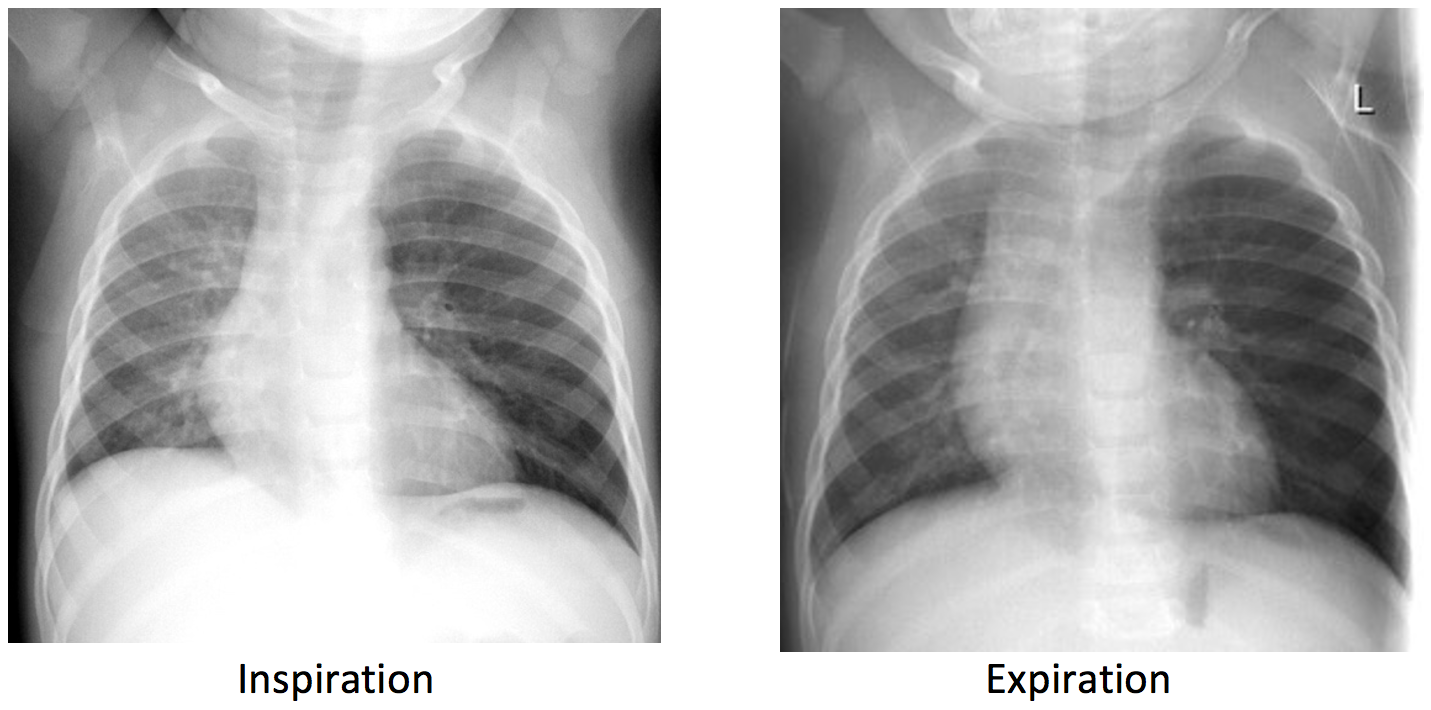
Air trapped in the lungs can be demonstrated easily with inspiratory and expiratory images. Yet, simple maneuver may be difficult to obtain in a child, and lead to inadequate or repeated images with an increase of radiation, as it also could occur performing fluoroscopy to identify a mediastinal shift.
Air trapping: The expiratory radiograph shows a clear expansion of the left lung and a mediastinal shift to the right.
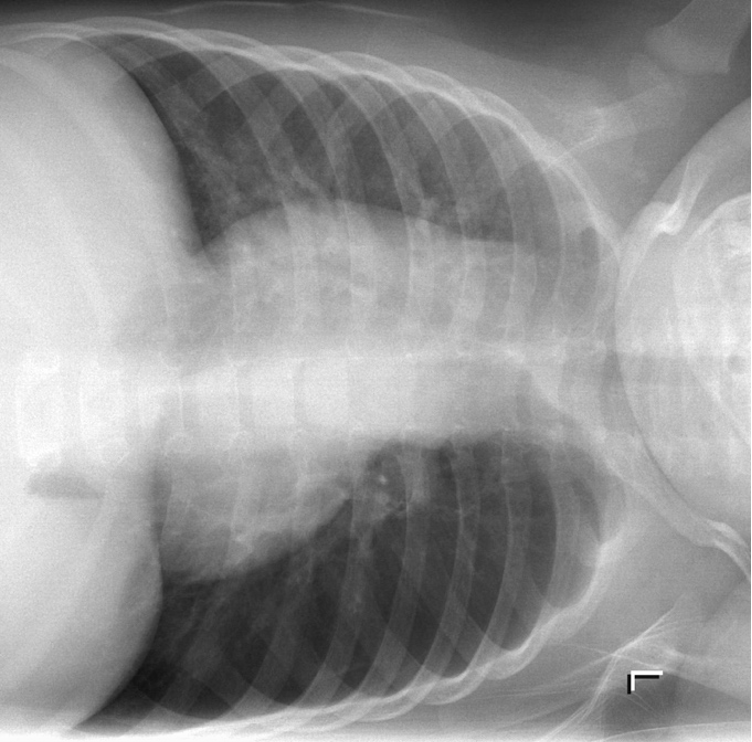
Now, I must confess that I cheated you a little bit, in order to enhance the topic. The expiratory image was not obtained in a supine position, but in a left lateral decubitus:
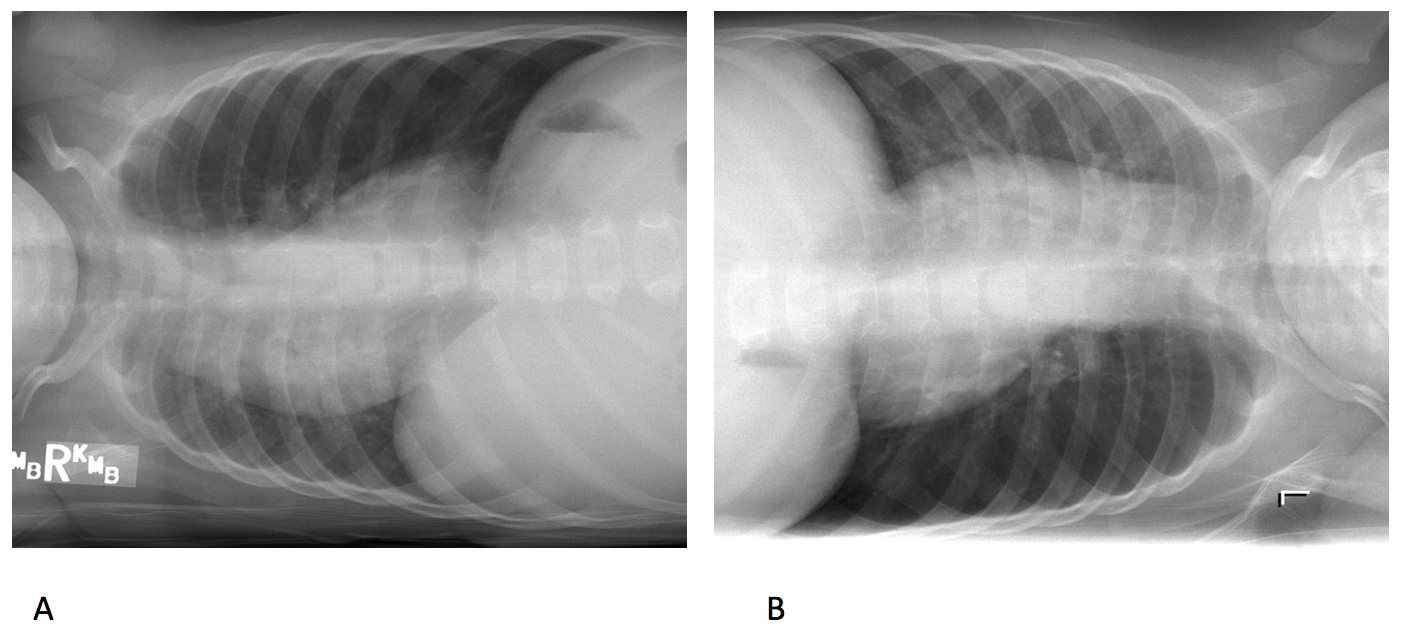
This simple way to obtain an expiratory radiograph was published in 1972 by Capitanio and colleagues. It consists in placing the child in the lateral decubitus with the pathological side down.
The rationale of this is that the dependent lung, due to the thoracic compression and gravity, tends to exhale the air in the lung and, thus, be in expiration, while the nondependent lung is not. As shown here, you can see the change using both lateral decubiti.
Notice how the right lung in our case in A diminishes it size and the left lung remains expanded in B.
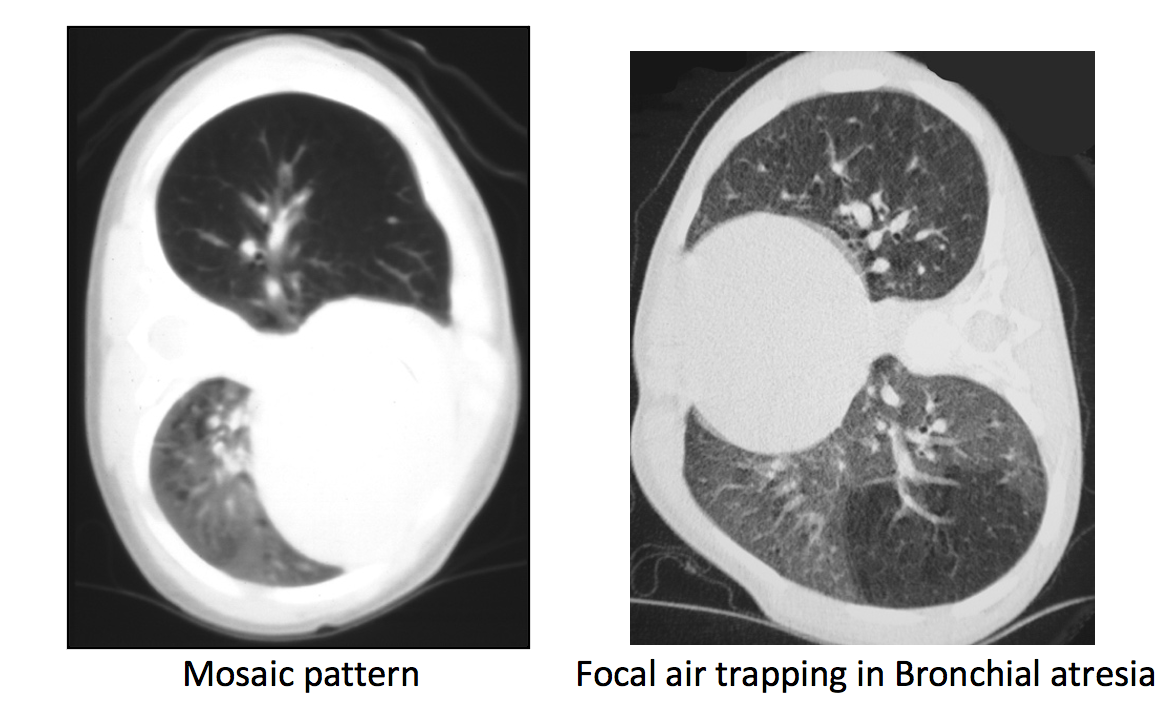
Lucaya and colleagues demonstrated how useful this maneuver is in other situations such as in cases of bronchiolitis or in partial bronchial atresia.
In conclusion and to remember:
- In the presence of a hyperlucent lung air trapping may help in the diagnosis.
- Air trapping in a child, or a non-collaborative patient, may be demonstrated using lateral decubitus radiographic projections or lateral decubitus CT.
References:
- Capitanio MA, Kirkpatrick JA. Lateral decubitus film: an aid in determining air-trapping in children. Radiology 1972; 103:460-462 [Crossref] [Medline] [Google Scholar]
- Lucaya J, Gartner S, García-Peña P, Cobos N, Roca I, Liñan S. Spectrum of manifestations of Swyer-James-MacLeod syndrome. J Comput Assist Tomogr 1998; 22:592-597 [Crossref] [Medline] [Google Scholar]


Air trapping in the left lung (increased volume and hyperlucency). CT to look for endobronchial object? If history of infection maybe a Swyer James syndrome
CXR AP, hyperinflatted left lung with increases radiolecency,in comparison to right with mild shift mediastinum to right
In this age group foreign body aspiration should be seriously considered
Next step consultation of ENT (ear nose throat ) specialist for arranging bronchoscope examination
for both diagnosis and therapeutic intervention
The mediastinum is shifted to the right . The right ling is not well expanded . Compensatory hyper expantion of the left lung . Likely partial bronchial obstruction (? FB).
Left lung hyperinflation due to FB aspiration (check valve mechanism)
Left lung fields are overinflated with mild tracheal deviation to right.
Tracheal papillomatosis.
Left lung hyperinflation for FBA
Clear lung on the left, small, denser right lung with bronchial accent, right deviation from the mediatin without scoliosis, it reminds me of Mac Leod
Most of you are in the right track. Then what would you do?
May an expiration chest x ray be of help?
Exactly Lola!. The question is: how do you obtain an expiratory radiograph in a small child?
Requiring good technician,to time imaging when the child crying (at the end of crying sound and before the next breath)
When suspecting obstruction at tracheal bifurcation fluroscopy of the child may be done to look for pendulous movement of mediastinum in inspiration and expiration.
x ray taken with left lateral decubitus position,with horizontal x ray beam.
the fundus air shadow with fluid level suggest the position of the baby
the left lung shows emphysematous changes-obstructive type with shift of mediastinum and herniation of left lung across the midline.
I guess the expiratory chest x ray was obtained following Olla’s method.
There is air trapping on the left side and swift of the mediastinum towards the right side. This is produced by a valvular mechanism within the left bronchus. Would be a bronchoscopy the next step? Or would it be sensible to do a CT chest in order to identify if there is more than one foreign bodies?
May is here!